INTRODUCTION TO SHOULDER ARTHROSCOPY DYNAMICS
Shoulder arthroscopy presents unique physiological and anatomical challenges compared to arthroscopic procedures of the knee or ankle. The tissue planes penetrated by the arthroscope and working instruments—specifically the deltoid muscle, rotator cuff, and thick bursal tissues—are substantially thicker and more highly vascularized than the relatively thin, avascular capsule of the knee. Consequently, maintaining a clear visual field requires a meticulous, multimodal approach to hemostasis and fluid management.
For the practicing orthopedic surgeon, mastering these variables is not merely a matter of convenience; it is a fundamental requirement for the safe execution of complex procedures such as rotator cuff repairs, labral reconstructions, and subacromial decompressions. Failure to control intraarticular bleeding or mitigate fluid extravasation can lead to catastrophic complications, including airway compromise, compartment syndrome, and iatrogenic neurovascular injury.
PATIENT POSITIONING: THE "BEACH CHAIR" CONFIGURATION
The "beach chair" position is widely utilized in shoulder arthroscopy due to its excellent anatomical orientation, ease of conversion to an open procedure, and the ability to manipulate the arm freely through a physiological range of motion.

While the beach chair position leverages gravity to assist with venous drainage—thereby naturally reducing venous bleeding in the surgical field—it introduces significant anesthetic complexities. The upright posture creates a hydrostatic gradient between the heart and the brain.
Surgical Warning: When utilizing the beach chair position, surgeons and anesthesiologists must account for the discrepancy between the blood pressure measured at the brachial artery and the actual cerebral perfusion pressure. For every inch of vertical height between the blood pressure cuff and the external auditory meatus, the mean arterial pressure (MAP) decreases by approximately 0.77 mm Hg. In older patients or those with cerebrovascular disease, aggressive hypotensive anesthesia in this position can precipitate cerebral ischemia.
CONTROL OF BLEEDING DURING ARTHROSCOPY
In addition to the judicious use of an arthroscopic radiofrequency ablation or electrocautery device, three primary techniques are employed to control intraarticular and subacromial bleeding.
1. Automated Arthroscopy Infusion Pumps
The foundation of visual clarity is the maintenance of a constant, regulated fluid flow and pressure. An automated arthroscopy pump should be utilized to maintain an intraarticular pressure of 60 to 70 mm Hg. Inflow is typically established through the arthroscopy sheath (utilizing a high-flow 6-mm inflow cannula). However, during extensive extraarticular procedures such as acromioplasties, a dedicated, separate inflow cannula may be indicated to optimize flow dynamics.
The physiological impact of pressurized fluid on the surrounding musculature has been extensively studied:
* Lee et al. utilized slit catheters to measure intramuscular deltoid pressure in 24 patients undergoing shoulder arthroscopy. They observed that compartment pressures transiently spiked to 50 mm Hg during pump infusion. Crucially, in all patients, these pressures normalized within 30 minutes postoperatively, despite the shoulders remaining clinically tense and swollen.
* Ogilvie-Harris and Boynton evaluated 25 arthroscopic shoulder procedures (including 20 acromioplasties) and reported that baseline deltoid pressures increased from 12 mm Hg to a peak of 120 mm Hg. Remarkably, within 4 minutes of terminating the fluid infusion, pressures returned to baseline. Electromyographic (EMG) follow-up revealed no evidence of ischemic muscle damage.
These data confirm that while infusion pumps generate transiently high intramuscular pressures, their use remains a highly safe and effective option for shoulder arthroscopy when utilized within standard parameters.
2. Pharmacologic Adjuncts: Epinephrine
A highly effective, low-risk measure to induce local vasoconstriction is the addition of epinephrine to the irrigation fluid. The standard protocol involves adding 1 mL of 1:1000 epinephrine to each 3000-mL bag of normal saline or lactated Ringer's irrigant.
This dilute concentration (1:3,000,000) provides excellent alpha-1 adrenergic receptor-mediated vasoconstriction of the capillary beds within the bursa and synovium. Provided the patient exhibits stable cardiovascular hemodynamics and lacks specific cardiac contraindications (e.g., severe arrhythmias or unstable angina), this mixture is exceptionally safe and rarely precipitates systemic anesthetic complications.
3. Hypotensive Anesthesia
Perhaps the most potent technique for optimizing the visual field is the implementation of controlled hypotensive anesthesia. The goal is to maintain a systolic blood pressure between 90 and 100 mm Hg.
Clinical Pearl: The critical metric for hemostasis is the pressure gradient between the patient's systolic blood pressure and the arthroscopic pump pressure. Maintaining a systolic-to-pump pressure gradient of approximately 30 mm Hg effectively tamponades capillary bleeding without requiring dangerously high intraarticular fluid pressures.
If a gravity-based fluid system is used instead of a mechanical pump, elevating the fluid bags exactly 3 feet above the level of the patient's heart produces a hydrostatic pressure of approximately 66 mm Hg. However, as previously noted, hypotensive anesthesia must be strictly avoided or heavily modified in elderly patients positioned in the beach chair configuration due to the risk of cerebral hypoperfusion.
MANAGEMENT OF FLUID EXTRAVASATION
Fluid extravasation is significantly more problematic in shoulder arthroscopy than in knee arthroscopy. The increased depth of the soft tissue envelope traversed by the instruments makes the reinsertion of displaced cannulas exceedingly difficult. Each time an instrument is blindly passed, or a "new" micro-tract is created during portal re-entry, the surrounding tissue is traumatized, exacerbating fluid leakage into the deltoid and pectoral fascia.
Extraarticular Dynamics
Procedures performed in the subacromial space (e.g., subacromial decompression, distal clavicle excision, rotator cuff repair) are inherently extraarticular. Unlike the glenohumeral joint, the subacromial space lacks a robust, watertight capsule. Consequently, fluid extravasation into the surrounding soft tissues can be profound.
In a landmark study, Lo and Burkhart evaluated 53 patients immediately following shoulder arthroscopy and documented an average fluid weight gain of 8.7 lbs (approximately 3.9 liters of retained fluid).
Mitigation Strategies
To minimize extravasation, established portals must be meticulously maintained. Surgeons should utilize:
* Interchangeable Cannula Systems: Allowing instruments to be swapped over a switching stick without losing the established tract.
* Threaded Cannulas: Preventing the cannula from backing out of the tissue during instrument withdrawal.
* Rubber Diaphragm Seals: Preventing fluid egress when the cannula is empty.
ANATOMICAL LANDMARKS AND PORTAL PLACEMENT
As shoulder arthroscopy has evolved to encompass highly complex reconstructive procedures, the number of described portals has proliferated. Unfortunately, portal nomenclature can be confusing, with various authors utilizing identical descriptive terms for anatomically distinct sites.
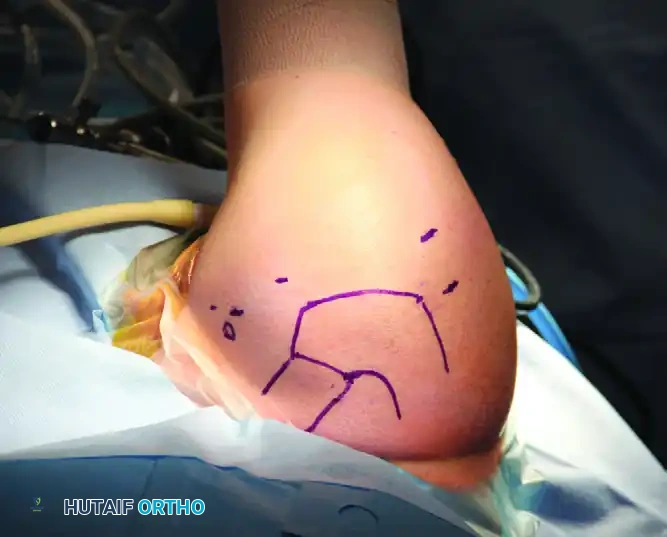
Before establishing any portal, a rigorous understanding of the local surface anatomy and underlying neurovascular structures is mandatory. Precise preoperative marking of bony landmarks is the first critical step.
Neurovascular Structures at Risk
The two structures at highest risk during shoulder arthroscopy are the axillary nerve and the suprascapular nerve.
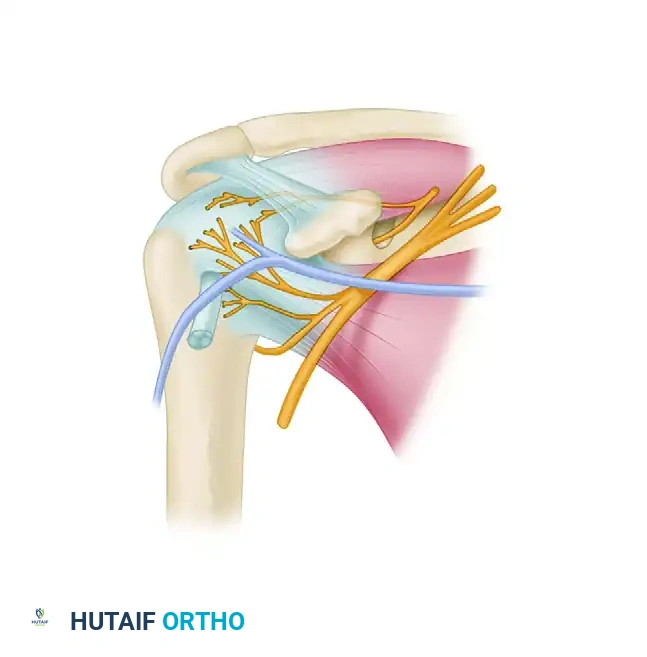
- Axillary Nerve: This nerve is vulnerable during the placement of anterior, posterior, and lateral portals. It courses inferior to the glenohumeral joint and winds around the surgical neck of the humerus. Nassar et al. demonstrated that the distance from the acromioclavicular (AC) joint to the axillary nerve is approximately 7.9 cm in men and 6.37 cm in women. The low anterior portal (often used for inferior capsular work) passes within 1 cm of the cephalic vein and must be established with direct intraarticular visualization to avoid the axillary nerve.
- Suprascapular Nerve and Artery: These structures are at risk during posterior and superior portal placement. They are located approximately 2 cm medial to the standard posterior portal site. Bigliani et al. mapped the suprascapular nerve, finding it located just 1.8 cm from the posterosuperior labrum and 2.5 cm from the superior glenoid tubercle.
Surgical Pitfall: When establishing lateral portals to access the glenohumeral space, the trocar must be directed to enter medial to the rotator arch to avoid iatrogenic damage to the cuff insertion and to stay clear of the axillary nerve's lateral trajectory.
STEP-BY-STEP GUIDE TO SPECIFIC ARTHROSCOPIC PORTALS
Arthroscopic portals are categorized by the anatomical space they access: the glenohumeral joint, the subacromial space, and the acromioclavicular joint. Proper spacing and angulation are crucial, particularly when multiple accessory portals are required for anchor insertion and suture management.
The Posterior Portal (The Primary Viewing Portal)
The posterior portal is the universal starting point for shoulder arthroscopy. It provides a panoramic diagnostic view of the glenohumeral joint and serves as the visual guide for establishing all subsequent anterior and superior portals.
- Location: The classic "soft spot" is located 1.5 to 3.0 cm inferior and 1.0 cm medial to the posterolateral tip of the acromion.
- Anatomy: This portal exploits a true internervous plane between the infraspinatus (innervated by the suprascapular nerve) and the teres minor (innervated by the axillary nerve).
- Technique: Palpate the posterior soft spot. Direct the trocar anteriorly and slightly medially, aiming toward the coracoid process. The surgeon will feel two distinct "pops"—the first as the trocar pierces the posterior deltoid fascia, and the second as it penetrates the posterior glenohumeral capsule.
Anterior Portals
Anterior portals are primarily working portals used for labral repairs, biceps tenodesis, and subscapularis work. They are established under direct intraarticular visualization (inside-out or outside-in technique) using the posterior portal for viewing.
* Standard Anterior Portal: Located in the rotator interval, bounded superiorly by the biceps tendon, inferiorly by the subscapularis tendon, and medially by the glenoid rim.
* Low Anterior Portal (5 O'clock Portal): Used for inferior Bankart repairs. Extreme caution is required as this portal passes perilously close to the cephalic vein and the axillary nerve.
Superior and Lateral Portals
- The Neviaser Portal (Suprascapular Portal): Located in the V-shaped fossa bounded by the clavicle anteriorly, the acromion laterally, and the scapular spine posteriorly. It is highly useful for superior labrum anterior and posterior (SLAP) repairs. It can be used safely provided the arm is positioned in no more than 45 degrees of abduction with no forward flexion during trocar introduction. In this specific position, the suprascapular artery and nerve are relaxed and out of the trajectory path.
- The Wilmington Portal: A posterolateral portal used for SLAP repairs. It is established approximately 1 cm anterior and 1 cm lateral to the posterolateral acromial corner. Surgeons must be aware that this portal directly crosses the supraspinatus tendon at its myotendinous junction.
Acromioclavicular (AC) Joint Portals
Arthroscopy of the AC joint is technically demanding due to the exceptionally tight joint space. The primary portals are the anterior and posterior AC portals, positioned immediately adjacent to the superior acromioclavicular ligament to preserve its stabilizing function.
Clinical Pearl: If AC joint arthroscopy or a distal clavicle excision is planned, an 18-gauge spinal needle should be inserted into the AC joint at the very beginning of the surgical case. Because subacromial fluid extravasation rapidly distorts superficial anatomy, identifying the narrow AC joint space later in the procedure becomes exceedingly difficult without fluoroscopic assistance.
POSTOPERATIVE PROTOCOLS AND COMPLICATION MANAGEMENT
Following shoulder arthroscopy, the immediate postoperative phase requires vigilant monitoring for complications related to fluid extravasation and patient positioning.
- Neurological Assessment: A thorough neurovascular examination must be documented in the Post-Anesthesia Care Unit (PACU). Specifically, the function of the axillary nerve (deltoid contraction, sensation over the lateral shoulder) and the musculocutaneous nerve (biceps contraction, lateral forearm sensation) must be verified to rule out traction neuropraxia or direct iatrogenic injury.
- Airway Monitoring: In cases of massive fluid extravasation (particularly after prolonged subacromial procedures), fluid can track medially along the fascial planes of the neck, leading to tracheal compression and airway compromise. Patients exhibiting excessive cervical swelling or stridor require immediate evaluation and potential delayed extubation.
- Compartment Syndrome: While rare, deltoid compartment syndrome can occur. The transient pressure spikes noted by Lee et al. typically resolve, but persistent, out-of-proportion pain accompanied by a tense, non-compressible deltoid warrants immediate investigation.
By adhering to strict hemostatic protocols, maintaining precise fluid management, and respecting the complex neurovascular anatomy during portal placement, orthopedic surgeons can consistently achieve optimal outcomes in advanced shoulder arthroscopy.
