INTRODUCTION TO CONGENITAL HYPEREXTENSION AND DISLOCATION OF THE KNEE
Congenital hyperextension and dislocation of the knee (CDK) represents a spectrum of rare, profound pediatric deformities characterized by the anterior displacement of the tibia relative to the femur. First described in the 19th century, this condition presents a complex reconstructive challenge for the pediatric orthopedic surgeon. The deformity is not merely an isolated capsular contracture but a multi-structural anomaly involving the extensor mechanism, collateral ligaments, cruciate ligaments, and the neurovascular bundle.
Understanding the pathoanatomy, associated syndromic conditions, and the precise biomechanical alterations is paramount. Management algorithms are highly dependent on the patient's age at presentation, the rigidity of the deformity, and the presence of concurrent musculoskeletal anomalies—most notably, developmental dysplasia of the hip (DDH).
CLASSIFICATION AND GRADING OF SEVERITY
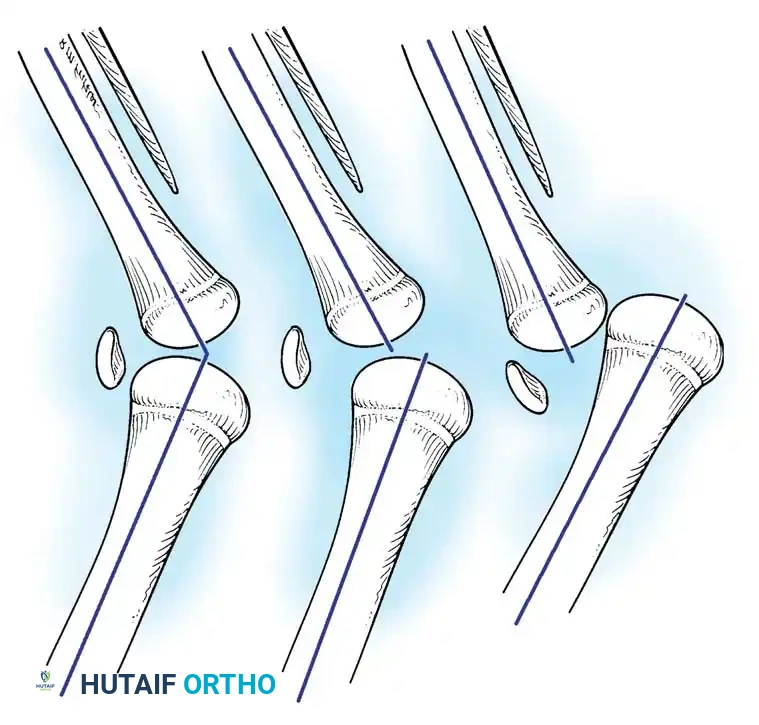
Congenital hyperextension of the knee is considered the lowest grade of a continuous spectrum of abnormalities. The condition is universally divided into three distinct grades based on the severity of the tibiofemoral displacement and the rigidity of the contracture.
- Grade 1 (Congenital Hyperextension): The tibia is hyperextended on the femur, but the articular surfaces remain congruent. The joint can typically be passively flexed to neutral or slightly beyond.
- Grade 2 (Congenital Hyperextension with Anterior Subluxation): The tibia is subluxated anteriorly on the femoral condyles. Joint congruity is partially lost, and passive flexion is significantly restricted by the contracted extensor mechanism.
- Grade 3 (Congenital Anterior Dislocation): Complete anterior dislocation of the tibia on the femur. The proximal tibia rests on the anterior aspect of the distal femur, and the femoral condyles are prominent posteriorly in the popliteal fossa.
Clinical Pearl: Differentiating between Grade 2 and Grade 3 is critical for treatment planning. Grade 3 dislocations often feature paradoxical extension, where the hamstring tendons subluxate anterior to the axis of rotation and act as knee extensors, severely complicating non-operative reduction.
ASSOCIATED MUSCULOSKELETAL ABNORMALITIES
Congenital hyperextension or dislocation of the knee is rarely an isolated finding; it is highly associated with skeletal abnormalities elsewhere in the extremity. The presence of CDK should immediately prompt a comprehensive evaluation for syndromic conditions (such as Larsen syndrome, arthrogryposis multiplex congenita, or myelomeningocele) and other packaging disorders.
In a landmark study of 155 children with congenital dislocation of the knee, Katz, Grogono, and Soper found other musculoskeletal abnormalities in 82 children, with 45 presenting with concurrent congenital dislocation of the hip (DDH). Similarly, in their focused study of 15 knees with congenital hyperextension and anterior subluxation of the tibia, Curtis and Fisher identified hip abnormalities in 11 patients.
Further reinforcing this association, Johnson, Audell, and Oppenheim found other abnormalities in 88% of their 17 patients, and Nogi and MacEwen reported congenital hip dysplasia in eight of 17 patients.
Surgical Warning: In a child presenting with both congenital dislocation of the knee and congenital dislocation of the hip, surgical or conservative correction of the knee must precede treatment of the hip. A flexed knee is an absolute prerequisite for the application of a Pavlik harness or a spica cast required to treat DDH.
PATHOANATOMY AND BIOMECHANICS
The pathological condition varies directly with the severity of the deformity, but a universal finding across all grades is the severe contracture of the anterior capsule of the knee and the quadriceps mechanism.
Ligamentous and Capsular Alterations
As the severity of the anterior displacement of the tibia increases, profound intraarticular and extraarticular changes occur. Katz et al. found the cruciate ligaments in five knees to be either markedly attenuated or completely absent. They postulated that the basic embryological defect in congenital dislocation of the knee is the absence or hypoplasia of these ligaments. However, other investigators consider these findings to be a secondary result of the chronic dislocation rather than the primary cause.
In severe anterior dislocations (Grade 3), the collateral ligaments course anteriorly from their femoral attachments, altering their functional vectors.
Muscular and Patellar Dysplasia
Curtis and Fisher noted significant fibrosis and a loss of muscle bulk in the vastus lateralis. The suprapatellar pouch is frequently obliterated by the adherent quadriceps tendon, tethering the extensor mechanism to the anterior femur.
Furthermore, in more than half of the affected knees, the patella is hypoplastic, absent, or displaced laterally. The hamstring muscles in some patients with severe deformity subluxate anteriorly past the mechanical axis of the knee joint, causing them to function paradoxically as extensors of the knee in this deformed position.

CLINICAL EVALUATION AND IMAGING
Diagnosis is typically obvious at birth. The newborn presents with a knee locked in hyperextension. Deep transverse skin creases are often visible over the anterior aspect of the joint, indicating chronic intrauterine malpositioning. Palpation reveals prominent femoral condyles in the popliteal fossa, with the tibial plateau resting anteriorly.
Radiographic evaluation is essential to confirm the grade of dislocation and assess for associated dysplasias. Lateral radiographs will clearly demonstrate the anterior displacement of the tibia and fibula relative to the distal femur.

NON-OPERATIVE MANAGEMENT
The treatment of congenital hyperextension of the knee depends heavily on the severity of the subluxation or dislocation and the age of the patient.
In a newborn with mild-to-moderate hyperextension (Grade 1) or subluxation (Grade 2), conservative treatment methods are highly effective. These include:
* Serial Casting: Gentle manipulation followed by serial casting to gradually stretch the anterior structures and increase knee flexion.
* Pavlik Harness: Used for posturing the knee in a continued flexed position once adequate passive flexion is achieved.
* Traction: In some protocols, gentle longitudinal skin traction is utilized to distract the joint before attempting flexion, preventing iatrogenic cartilage damage.
Ko, Shih, and Wenger reported treating 24 congenital knee dislocations in 17 patients (ranging from 10 minutes to 26 days old) with immediate reduction, serial casting, or traction. At an average follow-up of almost 5 years, excellent or good results were obtained in all patients who had no associated syndromic anomalies.
Criteria for Non-Operative Success
Roach and Richards proposed two strict criteria for the successful non-operative treatment of congenital knee dislocation:
1. Radiographic evidence of concentric joint reduction.
2. Clinical achievement of knee flexion to 90 degrees or more.
According to most authors, non-operative treatment can be continued for up to 3 months. In children who do not respond to conservative measures, the use of skeletal traction for correction is an option, but the deformity is notoriously difficult to correct with this method alone, often necessitating surgical intervention.
OPERATIVE MANAGEMENT: INDICATIONS AND PLANNING
In older children with moderate or severe subluxation or dislocation, or in infants who have failed 3 months of conservative management, surgery is strictly indicated. Children with syndromic associations (e.g., arthrogryposis) frequently possess rigid, teratologic dislocations that are refractory to casting and require early surgical release.
Curtis and Fisher described a comprehensive procedure for the correction of congenital dislocation of the knee, which remains the gold standard and is recommended for children 6 to 18 months old. The technique combines anterior capsular release, lengthening of the quadriceps mechanism, and the release of intraarticular adhesions.
Surgical Pearl: Occasionally, the articular surfaces of the knee remain abnormal if the deformity recurs or if the joint was left dislocated for a prolonged period. Ideally, a functional range of motion can be obtained through soft tissue release. In rare, neglected cases in older children, a femoral shortening osteotomy or distal femoral flexion osteotomy may be required to reduce the joint without placing excessive tension on the neurovascular bundle.
SURGICAL TECHNIQUE: CURTIS AND FISHER PROCEDURE
The Curtis and Fisher technique is a meticulous, stepwise soft-tissue reconstruction designed to address every contracted structure preventing reduction and flexion.
Positioning and Approach
- Place the patient supine on the operating table. Apply a well-padded pediatric pneumatic tourniquet to the proximal thigh.
- Make a long anterior midline incision starting superomedially at the level of the middle third of the femur and extending inferolaterally to the tibial tuberosity.
- Develop full-thickness fasciocutaneous flaps to expose the anterior thigh muscles and the entire extensor mechanism.
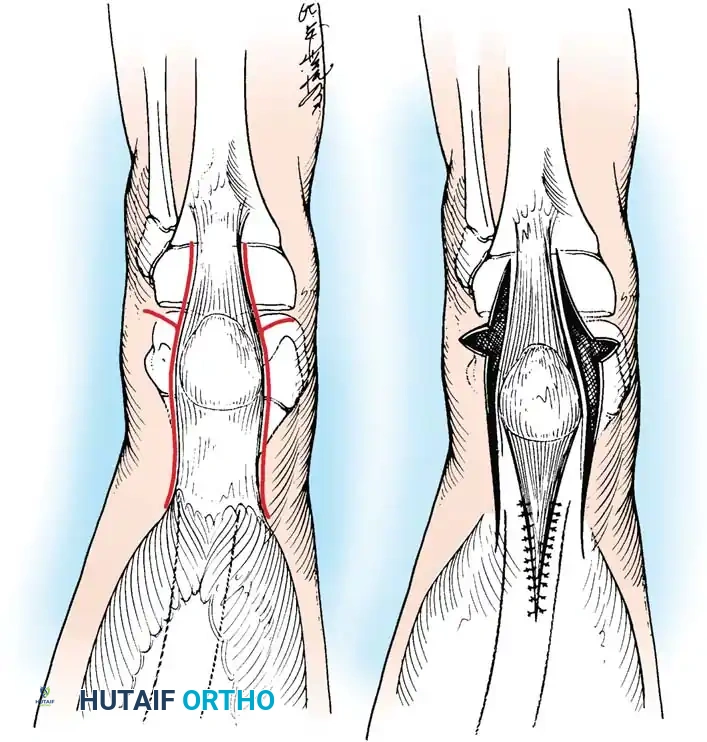
Quadriceps Lengthening
- Divide the quadriceps mechanism superior to the patella using either an inverted V-shaped incision or a Z-plasty.
- Note: The inverted V-shaped incision provides a robust tongue of tissue superior to the patella that is highly suitable for the secure attachment of the proximal muscle mass after the extensor mechanism has been lengthened.
Capsular Release and Ligamentous Mobilization
- Perform a transverse division of the anterior capsule. Extend this capsulotomy incision posteriorly to the borders of the tibial (medial) and fibular (lateral) collateral ligaments.
- Carefully mobilize and displace these collateral ligaments posteriorly as the knee is gently flexed. This step is critical to relocate the axis of rotation to its anatomic position.
- If the patella is displaced laterally (a common finding), release the lateral part of the patellar tendon and the fibrotic vastus lateralis. This allows the patella to be mobilized and centralized to its proper location within the femoral trochlea.
- Release any tight iliotibial band structures. If the fibular collateral ligament remains a tethering force against flexion, it may require fractional lengthening.
Extensor Mechanism Realignment and Closure
- Mobilize all normal-appearing quadriceps muscle tissue. Align the muscle mass in the long axis of the femur to ensure it exerts a direct, centralized pull on the patella.
- Suture the lengthened quadriceps mechanism. Meticulously repair the vastus medialis muscle to the lengthened rectus femoris to enhance dynamic medial stabilization and prevent lateral patellar subluxation.
- Evaluate the tracking of the patella by taking the knee through a range of motion from full extension to 90 degrees of flexion. Ensure the joint reduces concentrically without excessive tension.
- Deflate the tourniquet, achieve meticulous hemostasis, and close the wound in layers.
- Apply a long leg cast with the knee flexed to 30 degrees.
Pitfall: Do not cast the knee in maximum flexion (e.g., 90 degrees) immediately postoperatively. The anterior skin, which has been chronically contracted, will be placed under extreme tension, leading to a high risk of catastrophic skin necrosis and wound dehiscence.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management following a Curtis and Fisher release requires a delicate balance between protecting the soft tissue repair and preventing intraarticular arthrofibrosis.
Phase 1: Initial Immobilization (0 to 2 Weeks)
The patient remains in the initial long leg cast flexed at 30 degrees. If the anterior skin was noted to be under excessive tension during closure, the cast can be changed at 2 weeks under outpatient anesthesia to inspect the wound and incrementally increase flexion.
Phase 2: Mobilization (4 to 6 Weeks)
At 4 to 6 weeks postoperatively, the cast is completely removed. Active and passive range-of-motion exercises are initiated. In older, cooperative patients, continuous passive motion (CPM) machines can be utilized to regain motion and prevent the reformation of intraarticular adhesions during the first 3 to 6 weeks after surgery.
Phase 3: Long-Term Bracing (6 to 12 Months)
To protect the lengthened quadriceps and prevent a recurrence of the hyperextension deformity, a custom-molded long leg brace (KAFO) is worn for 6 to 12 months. The brace is typically locked to prevent terminal extension while allowing free flexion. Regular clinical and radiographic follow-up is mandatory to monitor joint congruity, patellar tracking, and the development of the femoral condyles.
