-
Conditions of bone mineral density
-
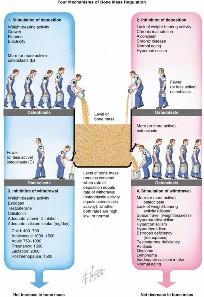
Bone mass is regulated by rates of deposition and withdrawal (
Fig.
1.20 ). - Osteoporosis
- Age-related decrease in bone mass
- Usually associated with estrogen loss in postmenopausal women ( Fig. 1.21)
- A quantitative, not qualitative, defect
- Mineralization remains normal
- World Health Organization’s definition
- Lumbar (L2–L4) density is 2.5 or more standard deviations less than mean peak bone mass of a healthy 25-year-old (T-score). 2. Osteopenia: bone density is 1.0–2.5 standard deviations less than the mean peak bone mass of a healthy 25-year-old. 4. Responsible for more than 1 million fractures per year
- Fractures of the vertebral body are most common.
- History of osteoporotic vertebral compression fractures are strongly predictive of subsequent vertebral fracture.
- After initial vertebral fracture, the risk for a second vertebral fracture is 20%.
- Vertebral compression fracture is associated with increased mortality rate.
- Incidence of vertebral compression fractures is higher among men than women.
- Lifetime risk of fracture in white women after 50 years of age: 75%
- The risk for hip fracture is 15%–20%.
- Risk factors ( Box 1.2)
- Cancellous bone is most affected.
- Clinical features
- Kyphosis and vertebral fractures
- Compression fractures of T11–L1 that create anterior wedge-shaped defects or centrally depressed codfish vertebrae
- Hip fractures
- Distal radius fractures
-
Type I osteoporosis (postmenopausal)
- Primarily affects trabecular bone
- Vertebral and distal radius fractures common
- Type II osteoporosis (age-related)
- Patients older than 75 years
- Affects both trabecular and cortical bone
- Related to poor calcium absorption
- Hip and pelvic fractures are common.
- Laboratory studies
- Obtained to rule out secondary causes of low bone mass:
- Vitamin D deficiency, hyperthyroidism, hyperparathyroidism, Cushing syndrome, hematologic disorders, malignancy
-
Complete blood cell count; measurements of serum calcium, phosphorus, 25(OH)D, alkaline phosphatase, liver enzymes, creatinine, and total protein and albumin levels; and measurement of 24-hour urinary calcium excretion
- Results of these studies are usually unremarkable in osteoporosis.
- Plain radiographs not helpful unless bone loss exceeds 30%
- Special studies
- Single-photon (appendicular) absorptiometry
- Double-photon (axial) absorptiometry
- Quantitative computed tomography (CT)
- Dual-energy x-ray absorptiometry (DEXA) 1. #### Most accurate with less radiation
- Biopsy
- After tetracycline labeling
- To evaluate the severity of osteoporosis and identify osteomalacia
- Histologic changes
- Thinning trabeculae
- Decreased osteon size
- Enlarged haversian and marrow spaces
- Treatment ( Fig. 1.22)
- Physical activity
- Supplements: 1000–1500 mg calcium plus 400–800 IU of vitamin D per day 1. More effective in type II (age-related) osteoporosis
- Bisphosphonates
- Inhibit osteoclastic bone resorption— direct anabolic effect on bone
- Categorized into two classes on the basis of presence or absence of a nitrogen side group:
-
Nitrogen-containing bisphosphonates—up to 1000-fold more potent in their antiresorptive activity
- Zoledronic acid (Zometa) and alendronate (Fosamax)
-
Inhibit protein prenylation within the mevalonate pathway, blocking farnesyl pyrophosphate synthase
-
Results in a loss of GTPase formation, which is needed for ruffled border formation and cell survival
- Non–nitrogen-containing bisphosphonates
- Metabolized into a nonfunctional ATP analogue, inducing apoptosis
-
Decreases skeletal
events in multiple myeloma -
Associated with osteonecrosis of the jaw
- Orthopaedic implications of bisphosphonate use
- Spine— reduced rate of spinal fusion in animal model ; withholding bisphosphonate is recommended after surgery.
-
Hip and knee—safe for use in cementless hip arthroplasty and cemented knee arthroplasty; may decrease rate of acetabular component subsidence

--- FIG. 1.20 Four mechanisms of bone mass regulation.
From Netter FH: CIBA collection of medical illustrations, vol 8: Musculoskeletal system, part I: Anatomy, physiology and developmental disorders, Basel, Switzerland, 1987, CIBA, p 181. - Fracture healing—no good data to recommend for or against use; will decrease future fracture risk
- Denosumab is a monoclonal antibody that targets and inhibits RANKL binding to the RANK receptor, which is found on osteoclasts.
- Other drugs (e.g., intramuscular calcitonin) may be helpful.
- Expensive and may cause hypersensitivity reactions
- Efficacy of bone augmentation with PTH, growth factors, prostaglandin inhibitors, and other therapies remains to be determined.
- Prophylaxis for patients at risk for osteoporosis
- Diet with adequate calcium intake
-
Weight-bearing exercise program

--- FIG. 1.21 Age-related changes in density and architecture of human trabecular bone from the lumbar spine. With progressive age, there is a quantitative decrease in bone, but the mineralization (qualitative) remains the same. B ox 1 . 2 R i s k F a c t or s for t h e Dev el opmen t of O s t eopor os i s 1. White race, female gender, northern European descent (fair skin and hair) - Sedentary lifestyle
- Thinness
- Smoking
- Heavy drinking
- Phenytoin (impairs vitamin D metabolism)
- Diet low in calcium and vitamin D
- History of breastfeeding
-
Positive family history of osteoporosis
• Premature menopause
From Keaveney TM, Hayes WC: Mechanical properties of cortical and trabecular bone, Bone 7:285–344, 1993. - Estrogen therapy evaluation at menopause
- Other causes of decreased mineral density
- Idiopathic transient osteoporosis of the hip
- Uncommon; diagnosis of exclusion
- Most common during third trimester of pregnancy in women but can occur in men
- Groin pain, limited ROM, and localized osteopenia without a history of trauma
- Treatment: analgesics and limited weight bearing
- Generally self-limiting and tends to resolve spontaneously after 6–8 months
- Stress fractures may occur.
- Joint space remains preserved on radiographs.
- Osteomalacia
- Femoral neck fractures are common.
- Qualitative defect
-
Defect of mineralization results in a large amount of unmineralized osteoid.
- Causes:
- Vitamin D–deficient diet
- GI disorders
- Renal osteodystrophy
- Certain drugs
- Aluminum-containing phosphate-binding antacids; aluminum deposition in bone prevents mineralization
-
Phenytoin (Dilantin)

--- FIG. 1.22 Treatment options for osteoporosis. Adapted from Simon SR, editor: Orthopaedic basic science, Rosemont, IL, 1994, American Academy of Orthopaedic Surgeons, p 174. - Alcoholism
- Radiographic findings
- Looser zones (microscopic stress fractures)
- Other fractures
- Biconcave vertebral bodies
- Trefoil pelvis
- Biopsy (transiliac) required for diagnosis
-
Widened osteoid seams are histologic
findings. - Treatment: usually includes large doses of vitamin D
- Osteoporosis and osteomalacia are compared in Fig. 1.23.
- Scurvy
- Vitamin C (ascorbic acid) deficiency
- Produces a decrease in chondroitin sulfate synthesis
-
Leads to defective collagen growth and repair

 FIG. 1.23 Comparison of osteoporosis and osteomalacia.
FIG. 1.23 Comparison of osteoporosis and osteomalacia.
From Netter FH: CIBA collection of medical illustrations, vol 8: Musculoskeletal system, part I: Anatomy, physiology and developmental disorders, Basel, Switzerland, 1987, CIBA, p 228. - Also leads to impaired intracellular hydroxylation of collagen peptides
- Clinical features:
- Fatigue
- Gum bleeding
- Ecchymosis
- Joint effusions
- Iron deficiency
- Radiographic findings:
- May include thin cortices and trabeculae and metaphyseal clefts (corner sign)
- Laboratory studies: normal results
- Histologic features
- Primary trabeculae replaced with granulation tissue
- Areas of hemorrhage
-
Widening of the zone of provisional calcification in the physis
- Greatest effect on bone formation in the metaphysis
- Marrow packing disorders
- Myeloma, leukemia, and other such disorders can cause osteopenia.
- Lead poisoning
- Results in short stature and reduced bone density
- Lead alters the chondrocyte response to PTH-related protein and TGF-β.
- Increased osteodensity
- Osteopetrosis (marble bone disease)
- Result of decreased osteoclast (and chondroclast) function: failure of bone resorption
- Osteopoikilosis (spotted bone disease)
- Islands of deep cortical bone appear within the medullary cavity and the cancellous bone of the long bones
- Especially in the hands and feet
- These areas are usually asymptomatic
- This disease is accompanied by no known incidence of malignant degeneration.
- Paget disease of bone (osteitis deformans)
- Elevated serum alkaline phosphatase and urinary
Decoding Bone Mineral Density Conditions: Osteoporosis & Beyond
Updated: Feb 2026
70 Views
Key Medical Takeaway
In this comprehensive guide, we discuss everything you need to know about Decoding Bone Mineral Density Conditions: Osteoporosis & Beyond. Bone mineral density conditions primarily include osteoporosis and osteopenia. Osteoporosis signifies an age-related decrease in bone mass, defined by lumbar density 2.5 or more standard deviations below a healthy 25-year-old’s peak bone mass (T-score). Osteopenia is when bone density is 1.0–2.5 standard deviations less. Both are quantitative defects that increase fracture risk.
Table of Contents

Keywords