INTRODUCTION TO COMPOSITE FREE TISSUE TRANSFERS
The neurovascular architecture of the foot renders it an exceptionally versatile donor site for complex microsurgical reconstruction. The ability to harvest thin, pliable, and sensate tissue—often with vascularized bone, tendon, or joint complexes—makes the foot an invaluable resource for addressing severe soft tissue and composite defects, particularly in the hand and contralateral lower extremity.
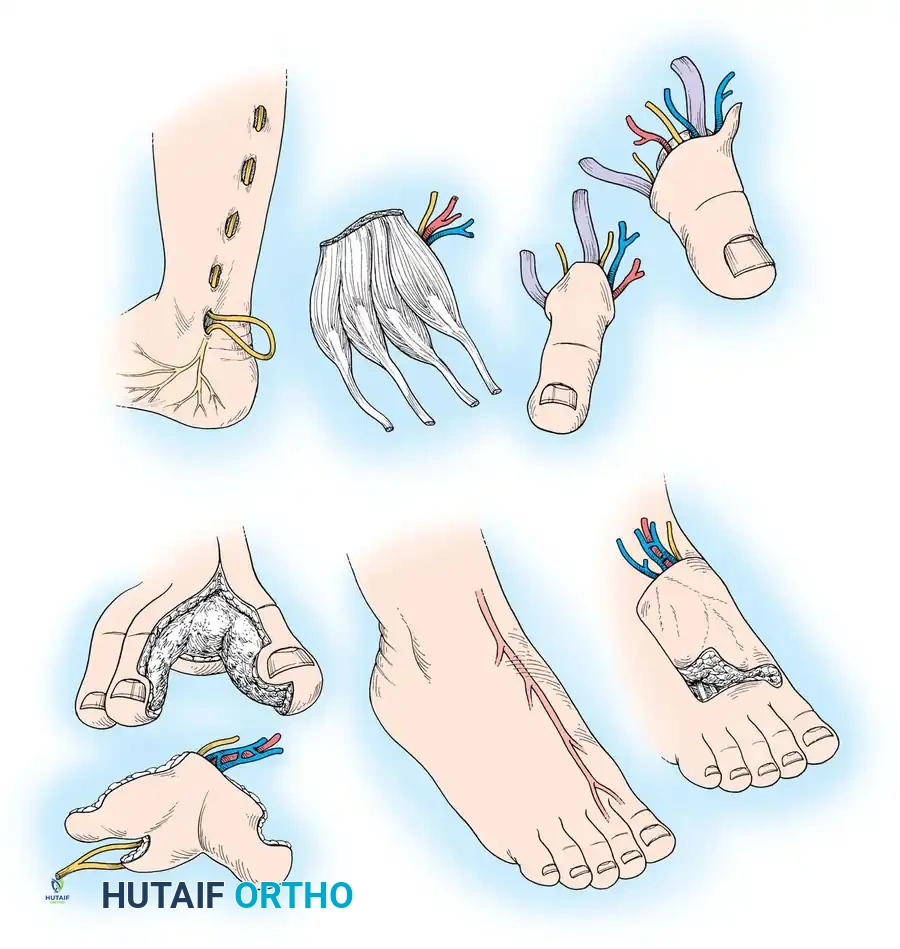
The spectrum of free tissue transfers available from the foot includes the dorsalis pedis flap, first web space flap, toe pulp transfers, "wraparound" flaps, vascularized joint transfers, epiphyseal transfers, and whole or partial great, second, and third toe transfers. Success in these demanding procedures requires an intimate understanding of the highly variable pedal vascular anatomy, meticulous microsurgical technique, and rigorous preoperative planning to mitigate donor site morbidity.
Surgical Warning: Donor site morbidity in the foot can be severe, including delayed wound healing, painful hypertrophic scarring, and gait disturbances. Strict adherence to anatomical planes, particularly preserving the extensor paratenon for skin grafting, is non-negotiable.
NEUROVASCULAR ANATOMY OF THE FOOT
A profound comprehension of the arterial, venous, and neural anatomy of the foot is the cornerstone of successful composite tissue transfer. The vascular tree of the foot is notorious for its anatomical variations, necessitating individualized preoperative assessment.
Arterial Supply and Critical Variations
The primary arterial inflow to the dorsum of the foot is the dorsalis pedis artery (DPA), a direct continuation of the anterior tibial artery. As it emerges deep to the inferior extensor retinaculum and crosses the ankle joint, it is reliably located between the extensor hallucis longus (EHL) tendon medially and the extensor digitorum longus (EDL) tendons laterally.
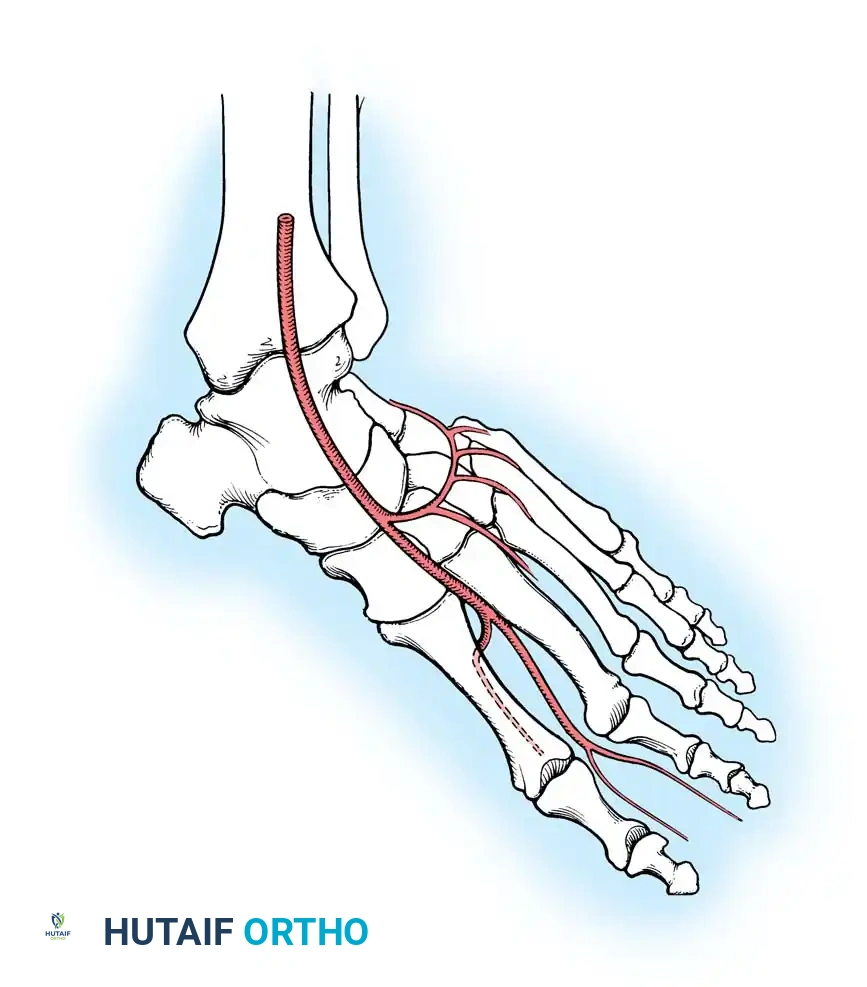
Passing distally over the tarsal bones, the DPA gives rise to the medial and lateral tarsal arteries. At the base of the metatarsals, it typically gives off the arcuate artery, which courses laterally to supply the second, third, and fourth dorsal metatarsal arteries.
The first dorsal metatarsal artery (FDMA) is the direct distal continuation of the DPA. It courses distally toward the first web space, supplying the dorsal skin, the first and second metatarsals, and the interosseous muscles. Near the first web space, the FDMA bifurcates: one branch passes deep to the EHL tendon to supply the medial aspect of the great toe, while the other divides to supply the adjacent sides of the great and second toes.
At the base of the first metatarsal, the deep plantar (communicating) artery branches from the DPA, diving plantarly between the heads of the first dorsal interosseous muscle to anastomose with the lateral plantar artery, thereby completing the plantar arterial arch. The first plantar metatarsal artery (FPMA) continues from this arch to supply the plantar aspects of the great and second toes.
Anatomical Variances of the First Metatarsal Artery
The anatomical course of the FDMA is highly variable and dictates the feasibility and approach for flap harvest.
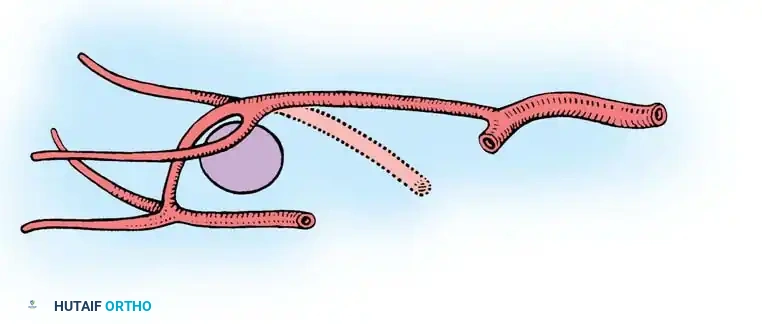
Independent cadaveric and clinical studies by May et al. and Gilbert demonstrated that the FDMA lies superficial to, or just within the substance of, the first dorsal interosseous muscle in 78% to 88% of cases (Type I). In the remaining cases, the artery dives deep, lying plantar to the first metatarsal (Type II).
Further studies by Buncke, Urbaniak, Leung, and Wong noted even greater variability, finding the FDMA dorsal to or within the muscle in only about 50% of patients. Other variations include an absent FDMA, reliance entirely on the plantar system, or hypoplasia of the DPA (normal diameter ranges from 1.8 to 3.0 mm).
Clinical Pearl: Always perform a preoperative Doppler ultrasound and, ideally, a two-plane angiography or MR angiography of the donor foot. If the DPA is absent, hypoplastic, or if the posterior tibial artery is occluded (making the foot reliant on the DPA for survival), the dorsalis pedis flap is strictly contraindicated.
Venous Drainage Systems
Venous outflow from the dorsum of the toes and foot is managed by a robust superficial venous network that coalesces into the dorsal venous arches. These arches feed into the greater saphenous vein medially and the lesser saphenous vein laterally.
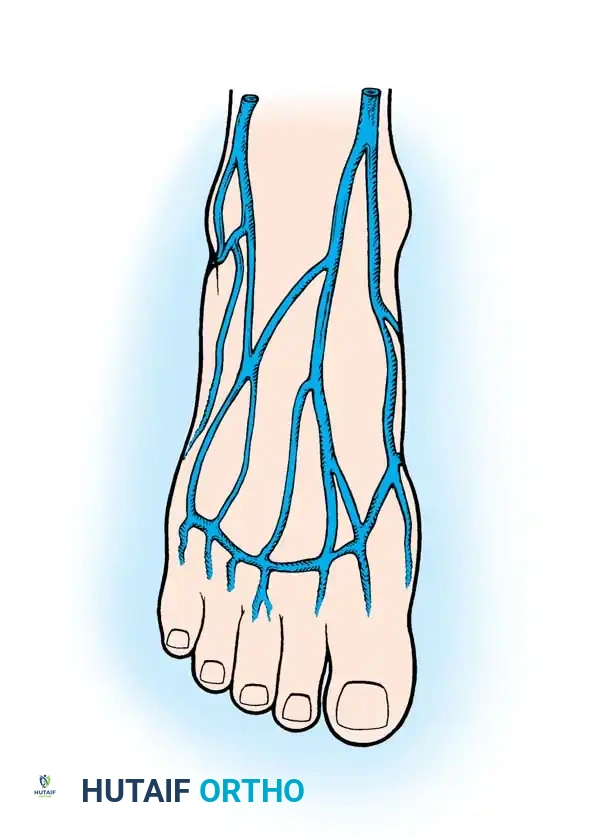
When harvesting flaps from the foot, the superficial venous system (specifically the greater saphenous vein or its major tributaries) is the preferred venous pedicle due to its large caliber and reliable drainage. Additional deep venous drainage occurs via the venae comitantes accompanying the dorsalis pedis artery, which can be used as a secondary or alternative venous anastomosis.
Cutaneous Innervation
The foot provides excellent options for sensate free flaps, crucial for reconstructing tactile surfaces like the hand or weight-bearing areas of the heel.
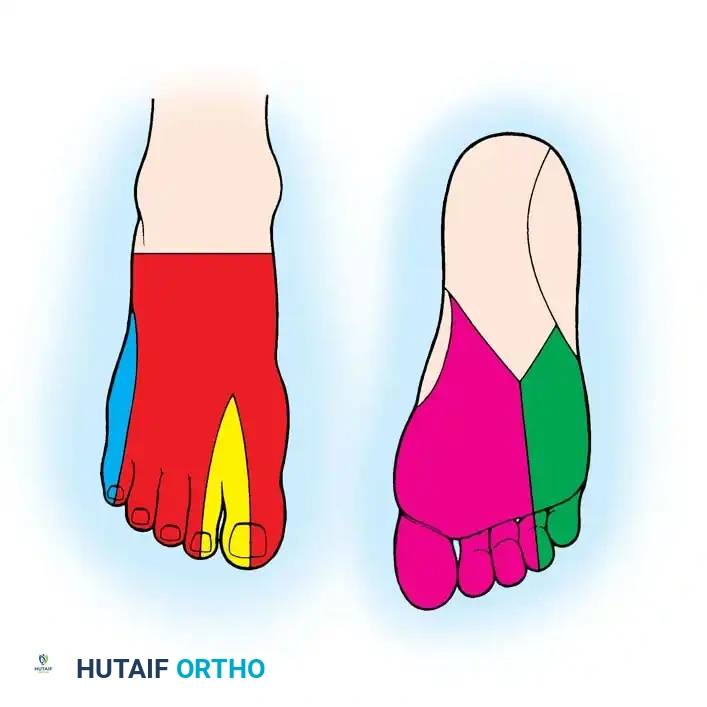
- Superficial Peroneal Nerve: Supplies the majority of the dorsal skin of the foot and toes.
- Deep Peroneal Nerve: Provides discrete sensory innervation to the first web space.
- Medial Plantar Nerve: Digital branches supply the plantar surface of the great toe and adjacent toes, offering critical glabrous skin innervation.
- Sural Nerve: Supplies the lateral aspect of the foot and is frequently harvested as a vascularized or non-vascularized nerve graft.
THE DORSALIS PEDIS FREE FLAP
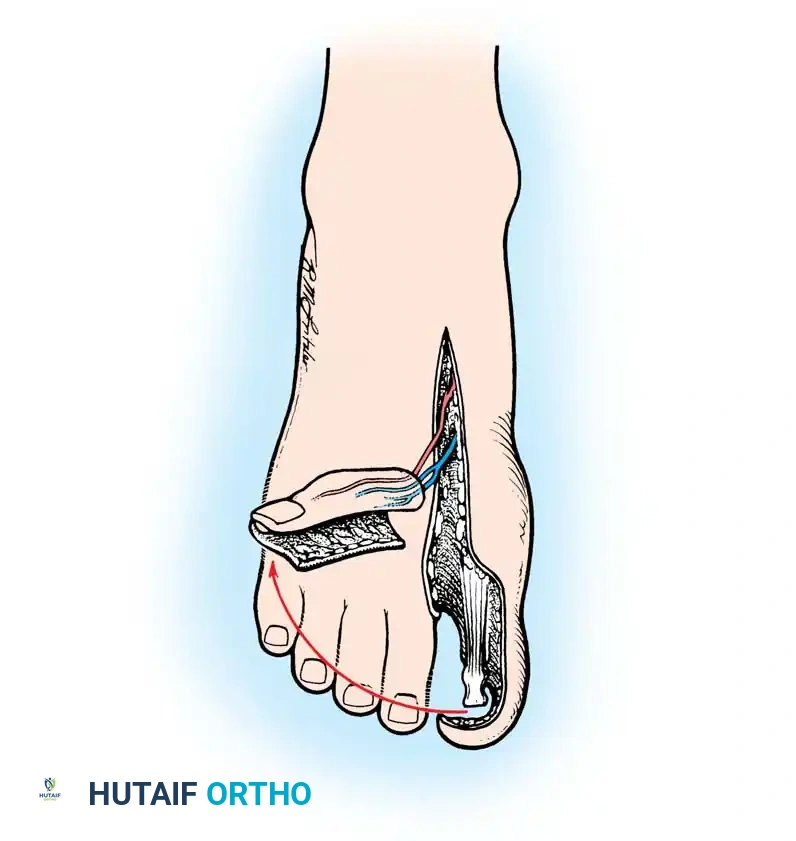
The dorsalis pedis flap is a highly versatile fasciocutaneous or composite flap. It is particularly valuable for resurfacing defects in the palm, thumb web space, and contralateral foot where thin, pliable, and sensate tissue is required.
Advantages and Disadvantages
Advantages:
* Large-caliber arteriovenous pedicle (DPA and saphenous vein).
* Long vascular pedicle can be dissected (up to 10 cm or more).
* Can be innervated via the superficial peroneal nerve.
* Extremely thin and pliable tissue.
* Can be harvested as a composite flap including the second metatarsal bone or extensor tendons.
* Capable of providing a relatively large skin paddle (up to 10 cm × 10 cm in select patients).
Disadvantages:
* Technically demanding and tedious dissection.
* High risk of donor site morbidity (delayed healing, painful hypertrophic scarring, skin graft failure over tendons).
* Restricted size in patients with smaller feet (often limited to 7 cm × 7 cm).
* Absolute contraindication if the posterior tibial artery is compromised or if the DPA is absent/hypoplastic.
Preoperative Planning
A two-team approach is mandatory to minimize ischemia time and operative duration. The recipient site must be thoroughly debrided and the recipient vessels isolated and prepared before the donor pedicle is divided. Arteriography of both the donor foot and the traumatized recipient limb is highly recommended to map vascular anomalies and zones of injury.
🔪 Surgical Technique 60-29: Dorsalis Pedis Flap Elevation
-
Marking and Positioning:
- Identify and outline the course of the dorsalis pedis artery using a handheld Doppler probe.
- Place the foot in a dependent position to engorge the superficial veins. Map the dorsal venous arch and the greater saphenous system with a surgical marker.
- Design the flap dimensions based on the recipient defect. The proximal limit is generally the inferior extensor retinaculum; the distal limit is approximately 2 cm distal to the palpable DPA pulse (near the metatarsophalangeal joints).
- Crucial Boundary: Limit the medial border to the EHL tendon and the lateral border to the fifth toe EDL tendon. Extending beyond these borders drastically increases the risk of donor site skin graft failure.
-
Initial Dissection:
- Exsanguinate the limb with an Esmarch bandage and inflate the pneumatic tourniquet.
- Begin the incision on the medial border of the outlined flap.
- Critical Step: The dissection must remain strictly superficial to the extensor paratenon. Stripping the paratenon will leave bare tendon, resulting in inevitable failure of the subsequent split-thickness skin graft.
-
Pedicle Isolation:
- Dissect laterally toward the EHL tendon and incise the deep fascia overlying it.
- Proceed deep to the periosteum of the first metatarsal to identify the DPA, its venae comitantes, and the deep peroneal nerve.
- If a sensate flap is planned, identify the branches of the superficial peroneal nerve proximally, transect them, and include them within the flap tissue.
-
Distal and Lateral Dissection:
- Continue dissection laterally and distally to expose the origin of the FDMA, the deep plantar (communicating) artery, and the arcuate artery.
- Isolate, ligate, and transect the deep plantar artery as it dives between the heads of the first dorsal interosseous muscle.
- Composite Harvest: If vascularized bone is required, perform osteotomies to include a portion or all of the second metatarsal at this stage.
-
Flap Elevation:
- Elevate and transect the extensor hallucis brevis (EHB) tendon. While some surgeons include the EHB with the flap, leaving the muscle belly in the donor bed can significantly improve the vascularity of the bed for skin grafting.
- Continue distal dissection, keeping the FDMA superficial to the dissection plane. Incise the distal margins of the flap.
- Ligate and divide the terminal arterial branches to the toes.
-
Pedicle Lengthening and Harvest:
- If a longer pedicle is required, perform a Z-lengthening incision over the extensor retinaculum. Dissect the DPA and anterior tibial artery proximally.
- Release the tourniquet to confirm flap perfusion and achieve meticulous hemostasis of the donor bed.
- Once the recipient site is fully prepared, ligate the proximal pedicle, transfer the flap, and immediately apply a meshed split-thickness skin graft to the donor site. Immobilize the foot in a posterior splint.
FIRST WEB SPACE AND TOE PULP TRANSFERS
The first web space and the plantar pulp of the toes offer specialized, glabrous skin that is biomechanically and functionally analogous to the palmar skin of the hand.
Rationale and Advantages
Pioneered by Gilbert et al. in 1975, the first web space free tissue transfer revolutionized hand reconstruction, particularly for severe thumb web space contractures and digital resurfacing.
Advantages:
1. Superior Sensibility: The two-point discrimination (2-PD) of the toe pulp ranges from 10 to 18 mm, offering excellent potential for functional sensory recovery when anastomosed to digital nerves.
2. Glabrous Skin: The tissue is durable, hairless, and resists shear forces, perfectly mimicking palmar skin.
3. Reliable Vascularity: Supported by the robust FDMA and plantar arterial systems.
4. Versatility: Can be combined with the dorsalis pedis flap for massive defects or utilized as a "wraparound" flap for thumb reconstruction.
5. Low Morbidity: When closed primarily or grafted successfully, donor site morbidity is minimal compared to the dorsalis pedis flap.
Disadvantages:
* Requires a highly skilled two-team microsurgical approach.
* Risk of complete flap loss secondary to microvascular thrombosis.
* Potential for cold intolerance and hypersensitivity in the reconstructed digit (reported in up to 73% of patients by Ratcliffe and McGrouther).
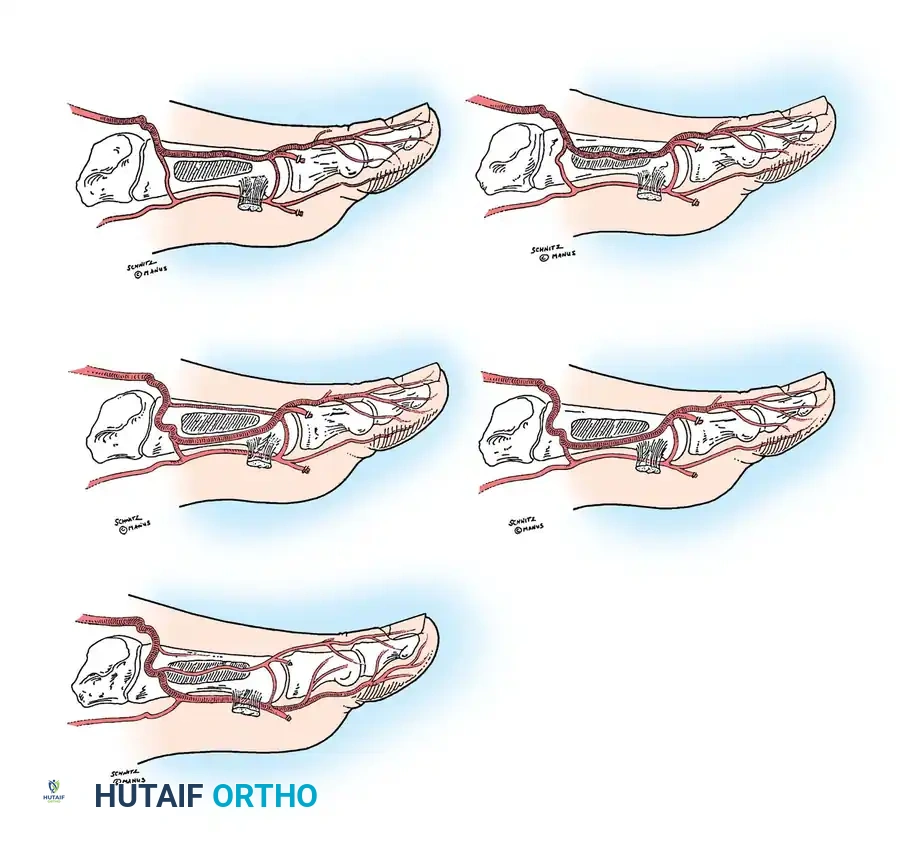
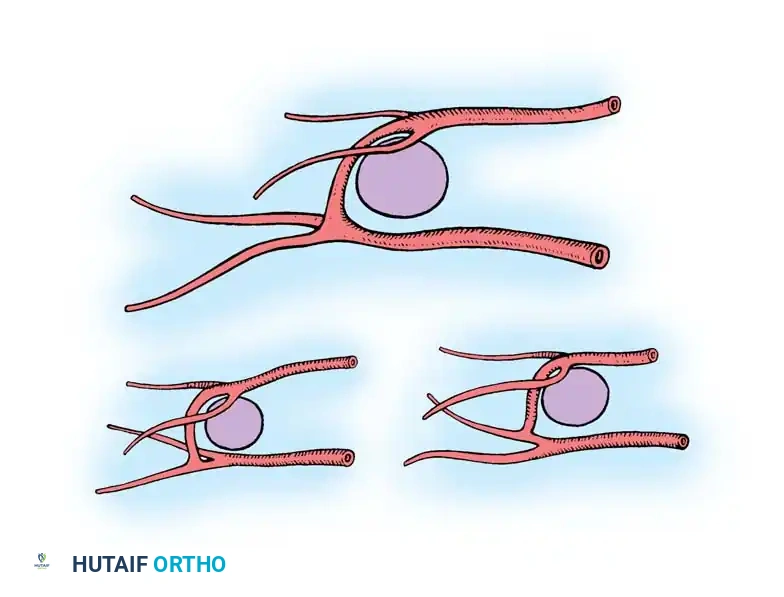
Anatomical Considerations of the First Web
The vascular dominance of the first web space relies on the terminal branches of the FDMA and the FPMA. May et al. identified three distinct patterns of the distal communicating artery (the terminal continuation of the FDMA) joining the plantar digital arterial system. Understanding these anastomotic patterns is vital when dissecting the distal pedicle to ensure adequate perfusion to the harvested pulp or web space skin.
TOE-TO-HAND TRANSFERS AND WRAPAROUND FLAPS
For traumatic amputations of the thumb or fingers, composite toe transfers provide unparalleled functional and aesthetic restoration. The great toe, second toe, or customized "wraparound" flaps can be harvested based on the specific reconstructive requirements.
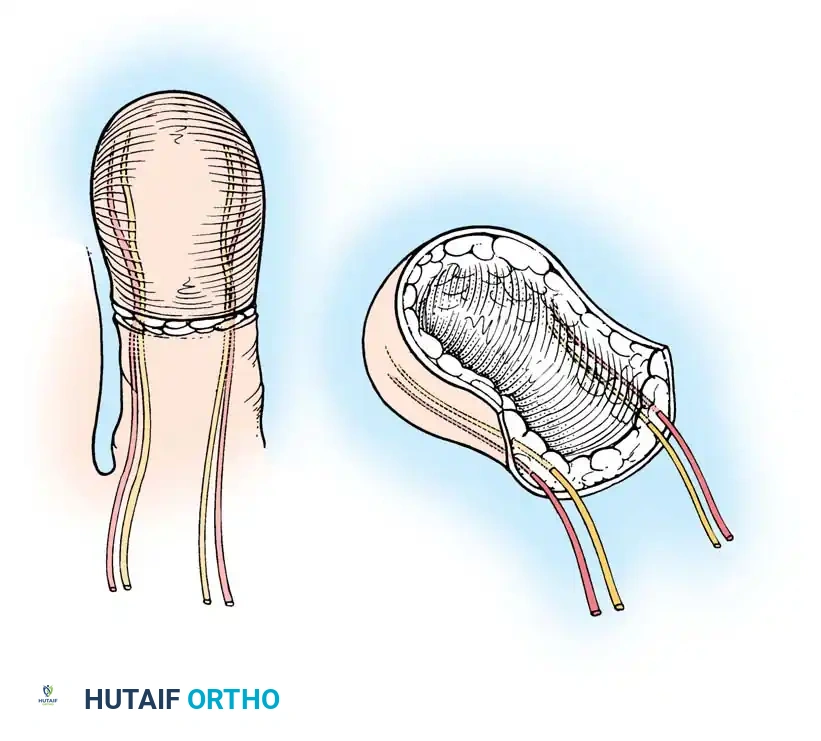
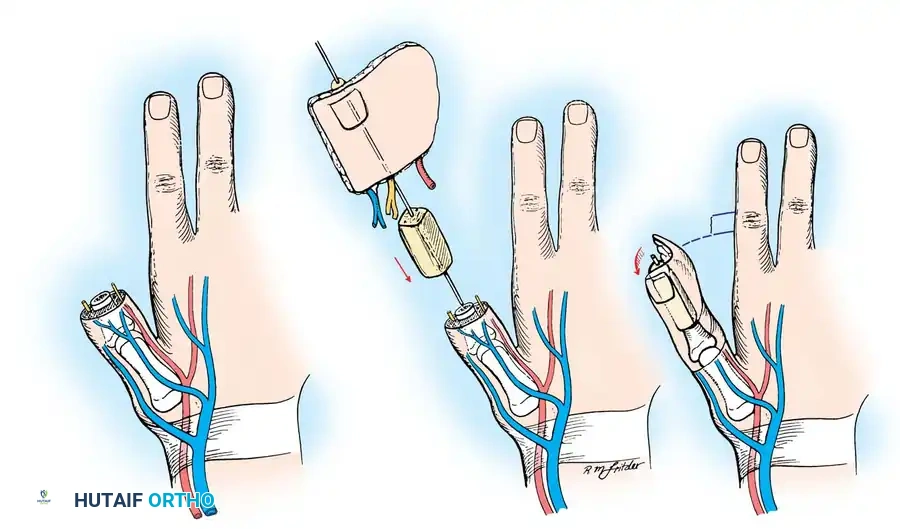
The Wraparound Flap
The wraparound flap involves harvesting the skin, nail bed, and a sliver of distal phalanx from the great toe, leaving the core bone and contralateral neurovascular bundle intact. This tissue is then "wrapped" around an iliac crest bone graft at the recipient thumb site.
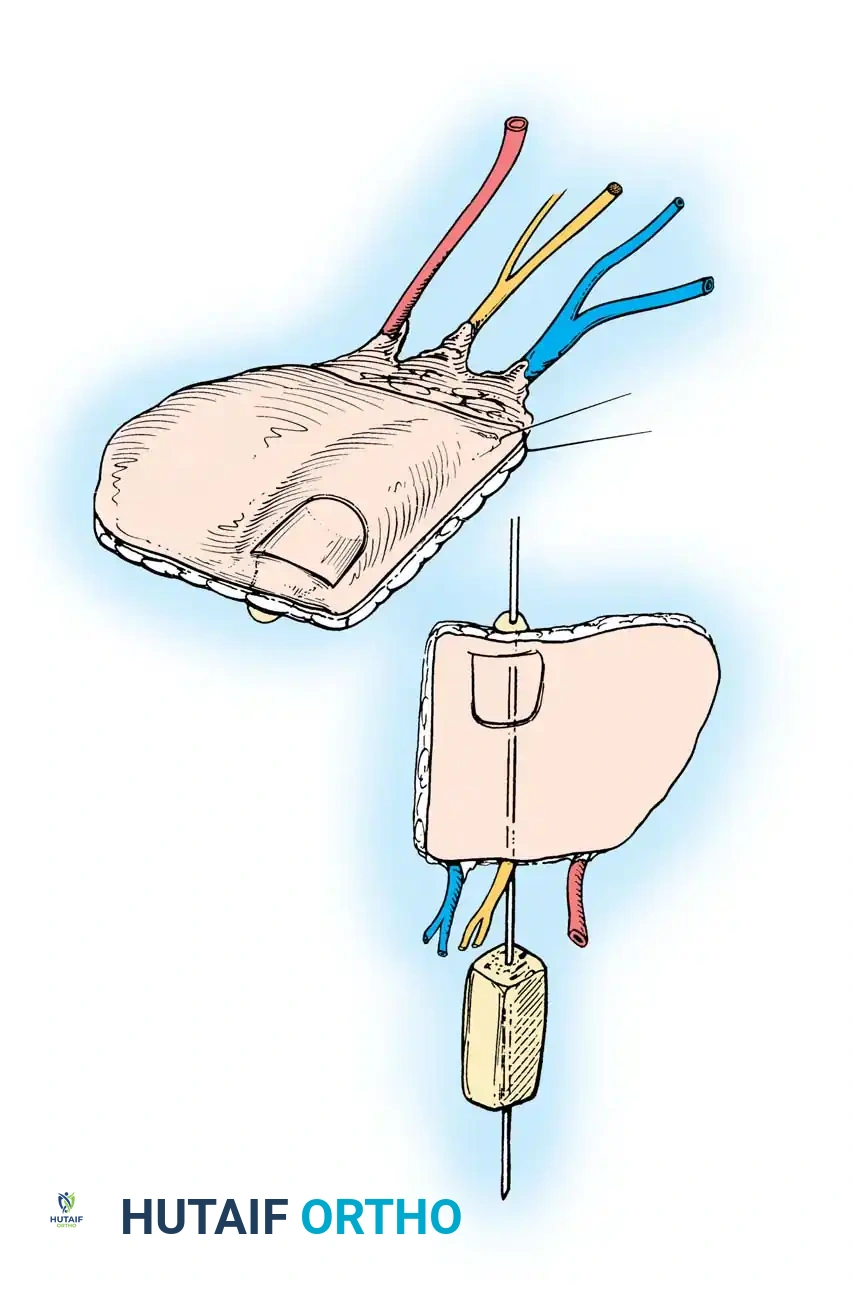
This technique preserves the structural integrity of the donor great toe, significantly reducing gait morbidity while providing a highly aesthetic and functional thumb reconstruction.
Second and Third Toe Transfers
When full joint articulation and tendinous structures are required, whole toe transfers are indicated. The second toe is frequently chosen for finger reconstruction due to its proportional size and the minimal donor site morbidity following ray amputation and primary closure of the foot.
During harvest, the plantar and dorsal digital nerves are carefully dissected and tagged. The flexor and extensor tendons are transected proximally to provide sufficient length for interlacing at the recipient site. The vascular pedicle (typically the FDMA and dorsal venous system) is traced proximally to ensure adequate caliber for microvascular anastomosis.
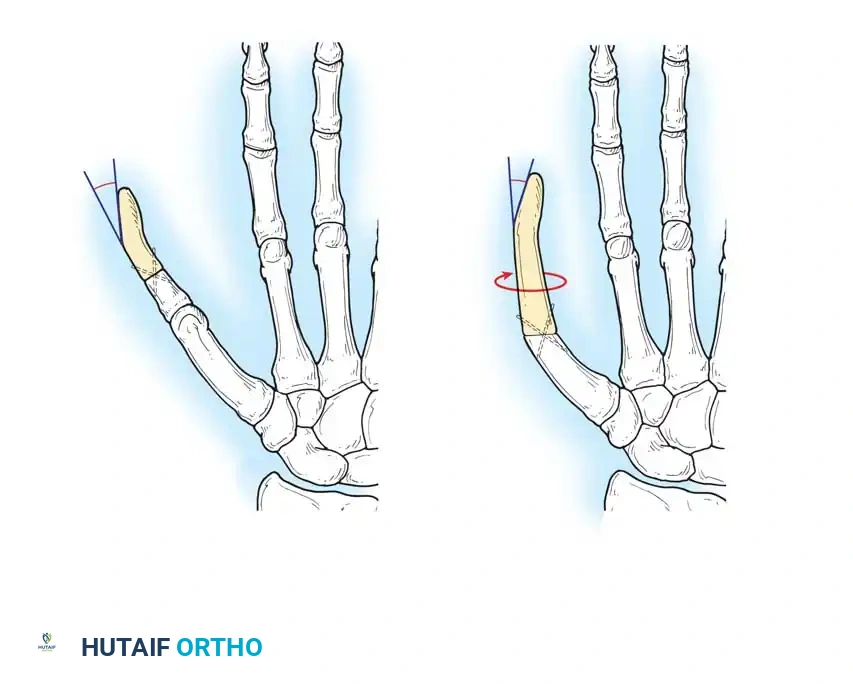
Surgical Pearl: When harvesting a second toe, preserve the deep transverse metatarsal ligament if possible, or meticulously repair it to prevent splaying of the forefoot and subsequent metatarsalgia.
POSTOPERATIVE PROTOCOLS AND COMPLICATION MANAGEMENT
The success of a composite free tissue transfer extends well beyond the operating room. Strict postoperative management is critical to prevent vasospasm and thrombosis.
Flap Monitoring and Environment
- Temperature Control: The patient's room must be kept warm (ambient temperature > 75°F / 24°C) to prevent peripheral vasoconstriction.
- Monitoring: Clinical assessment of flap color, capillary refill, and turgor is paramount. Surface Doppler mapping of the arterial pedicle should be performed hourly for the first 48 hours, then every 2-4 hours.
- Positioning: The recipient limb must be strictly elevated to promote venous drainage and reduce edema. The donor foot must also be elevated and immobilized in a well-padded posterior splint to protect the skin graft.
Anticoagulation and Medications
While protocols vary by institution, a common regimen includes:
* Intravenous hydration to maintain euvolemia and optimize cardiac output.
* Aspirin (81 mg to 325 mg daily) for antiplatelet effect.
* Dextran 40 or low-dose Heparin infusions may be utilized in cases of complex anastomoses or known hypercoagulable states, though their routine use is debated due to bleeding risks.
* Strict prohibition of smoking, nicotine products, and caffeine for a minimum of 6 weeks postoperatively to prevent catastrophic vasospasm.
Managing Complications
If arterial insufficiency (pale, cool flap with loss of Doppler signal) or venous congestion (purple, engorged flap with brisk capillary refill) is detected, immediate surgical re-exploration is mandatory. Time is tissue; delays beyond a few hours often result in irreversible no-reflow phenomenon and complete flap loss.
Donor site complications, particularly following dorsalis pedis flap harvest, require aggressive management. Areas of skin graft loss over tendons should be treated with meticulous local wound care, enzymatic debridement, and occasionally, secondary coverage with local rotational flaps or negative pressure wound therapy once granulation tissue forms.
CONCLUSION
Composite free tissue transfers from the foot represent the pinnacle of reconstructive microsurgery. By mastering the intricate and variable neurovascular anatomy of the foot, the reconstructive surgeon can unlock a vast armamentarium of tissues capable of restoring profound functional and aesthetic deficits. Rigorous patient selection, meticulous surgical execution, and vigilant postoperative care remain the triad of success in these complex procedures.
📚 Medical References
- free tissue transfer for emergency salvage of traumatic below-knee amputation stumps, Plast Reconstr Surg 98:538, 1996.
- Jensen JS, Paulsen M, Krosnick M: Through-knee amputations, Acta Orthop Scand 53:463, 1982.
- Kasabian AK, Glat PM, Eidelman Y, et al: Salvage of traumatic below-knee amputation stumps utilizing the fi let of foot free fl ap: critical evaluation of six cases, Plast Reconstr Surg 96:1145, 1995.
- Kjøble J: The surgery of the through-knee amputation. In Murdock G, ed: Prosthetic and orthotic practice, London, 1970, Edward Arnold. Kock HJ, Friederichs J, Ouchmaev A, et al: Long-term results of through-knee amputation with dorsal musculocutaneous fl ap in patients with end-stage arterial occlusive disease, World J Surg 28:801, 2004.
- Loder RT, Herring JA: Disarticulation of the knee in children: a functional assessment, J Bone Joint Surg 69A:1155, 1987.
- MacKenzie EJ, Bosse MJ, Castillo RC, et al: Functional outcomes following trauma-related lower-extremity amputation, J Bone Joint Surg 86A:1636, 2004.
- Mazet R Jr, Hennessy CA: Knee disarticulation: a new technique and a new knee-joint mechanism, J Bone Joint Surg 48A:126, 1966.
- Mazet R Jr, Schmitter ED, Chupurdia R: Disarticulation of the knee: a follow-up report, J Bone Joint Surg 60A:675, 1978.
- Mohler DG, Kessler JI, Earp BE: Augmented amputations of the lower extremity, Clin Orthop Relat Res 371:183, 2000.
- Moore WS, Henry RE, Malone JM, et al: Prospective use of xenon Xe 133 for amputation level selection, Arch Surg 116:86, 1981.
- Murdock G: Knee-disarticulation amputation, Bull Prosthet Res 9:14, 1968.
- Nehler MR, Coll JR, Hiat WR, et al: Functional outcome in a contemporary series of major lower extremity amputations, J Vasc Surg 38:7, 2003.
- Persson BM: Sagittal incision for below-knee amputation in ischaemic gangrene, J Bone Joint Surg 56B:110, 1974.
- Pinzur MS, Bowker JH: Knee disarticulation, Clin Orthop Relat Res 361:23, 1999.
- Pinzur MS, Gottschalk F, Smith D, et al: Functional outcome of below-knee amputation in peripheral vascular insuffi ciency: a multicenter review, Clin Orthop Relat Res 286:247, 1993.
- Pinzur MS, Smith DG, Daluga DJ, et al: Selection of patients for through the knee amputation, J Bone Joint Surg 70A:746, 1988.
- Porter JM, Baur GM, Taylor LM Jr: Lower extremity amputations for ischemia, Arch Surg 116:89, 1981.
- Rayman G, Krishnan ST, Baker NR, et al: Are we underestimating diabetes-related lower-extremity amputation rates? Results and benefi ts of the fi rst prospective study, Diabetes Care 27:1892, 2004.
- Robinson KP: Skew fl ap below-knee amputation, Ann R Coll Surg Engl 73:155, 1991.
- Robinson KP, Hoile R, Coddington T: Skew fl ap myoplastic below-knee amputation: a preliminary report, Br J Surg 69:554, 1982.
- Rogers SP: Amputation of the knee joint, J Bone Joint Surg 44A:1697, 1962.
- Saleh M, Datta D, Eastaugh-Waring SJ: Long posteromedial myocutaneous fl ap below-knee amputation, Ann R Coll Surg Engl 77:141, 1995.
- Sandnes DK, Sobel M, Flum DR: Survival after lower-extremity amputation, J Am Coll Surg 199:394, 2004.
- Smith DG, Fergason JR:
