Complications in Arthroscopic Surgery: Prevention, Recognition, and Management

Key Takeaway
Arthroscopic complications, though infrequent, can be devastating. Most iatrogenic injuries—including neurovascular trauma, chondral scuffing, and fluid extravasation—are preventable through meticulous preoperative planning, precise portal placement, and profound anatomical knowledge. This guide details the biomechanical pitfalls, step-by-step preventative surgical techniques, and evidence-based management protocols required to mitigate risks such as popliteal artery laceration, traction neurapraxia, and postoperative hemarthrosis during advanced arthroscopic procedures.
INTRODUCTION TO ARTHROSCOPIC COMPLICATIONS
Arthroscopy has revolutionized orthopedic surgery, offering minimally invasive solutions with accelerated rehabilitation protocols. However, the perception of arthroscopy as a "benign" intervention can lead to catastrophic iatrogenic injuries if fundamental surgical principles are ignored. Complications during or after arthroscopy are infrequent and, fortunately, usually minor. Most are entirely preventable with rigorous preoperative and intraoperative planning, meticulous attention to the details of basic techniques, and a profound understanding of three-dimensional cross-sectional anatomy.
Familiarity with local anatomy and the acquisition of psychomotor skills through cadaveric learning centers, fellowship training, and staying current with peer-reviewed specialty journals allow the surgeon to mitigate risks. Epidemiological data provides a critical baseline for understanding these risks. In 1986, Small reported a retrospective survey of 395,566 arthroscopies with an overall complication rate of 0.56%. Historically, the highest complication rates occurred during the adoption phase of newer procedures, such as meniscal repair (2.4%), anterior cruciate ligament (ACL) reconstruction (1.8%), and anterior staple capsulorrhaphy of the shoulder (5.3%).
A subsequent, highly accurate prospective study by Small in 1988 found a complication rate of 1.68% across 10,262 procedures. The most common complications identified were:
* Hemarthrosis: 60.1%
* Infection: 12.1%
* Thromboembolic disease: 6.9%
* Anesthetic complications: 6.4%
* Instrument failure: 2.9%
* Complex Regional Pain Syndrome (CRPS / RSD): 2.3%
* Ligament injury: 1.2%
* Fracture or neurological injury: 0.6% each
Contemporary studies of arthroscopic procedures demonstrate a less than 1% occurrence of major complications requiring secondary surgical intervention. However, site-specific complications—such as spontaneous pneumothorax following shoulder arthroscopy or popliteal artery laceration during knee arthroscopy—demand absolute vigilance.
PREOPERATIVE PLANNING AND WRONG-SITE SURGERY PREVENTION
The foundation of complication prevention begins long before the patient enters the operating theater. Having all clinical office notes, advanced imaging (MRI/CT), and orthogonal radiographs displayed in the operating room is mandatory.
Wrong-site surgery remains a devastating "never event" in orthopedic surgery. To alleviate potential confusion on a high-volume operative day, rigorous adherence to standardized protocols is required. The Sign Your Site program initiated by the American Academy of Orthopaedic Surgeons (AAOS) and the Universal Protocol recommendations of the Joint Commission mandate:
1. Preoperative verification of the operative site with the awake patient.
2. Marking of the operative site by the attending surgeon using an indelible marker.
3. A formal "time-out" immediately before the procedure begins for final verification of the patient, procedure, implants, and a final safety checklist.
Clinical Pearl: Having the patient actively participate by writing the word "YES" or "CORRECT" on the operative extremity, and "NO" on the nonoperative extremity, adds an invaluable layer of cognitive verification for the entire surgical team.
Fig. 47-9: Operative extremity has been marked by the patient and verified by the surgeon to prevent wrong-site surgery.
IATROGENIC INTRAARTICULAR DAMAGE
Chondral and Osteochondral Injury
Damage to intraarticular structures is arguably the most common technical complication of arthroscopy. Scuffing, scoring, or gouging of the articular cartilage by the sharp tip of the arthroscope trocar or motorized instruments occurs most frequently under the following conditions:
* Inexperienced arthroscopists utilizing poor triangulation techniques.
* "Tight" joints with limited capsular compliance.
* Prolonged, technically demanding procedures leading to surgeon fatigue.
Forcing the arthroscope or rigid instruments between closely apposed articular surfaces (e.g., the femoral and tibial condyles, or the humeral head and glenoid) can severely score the hyaline cartilage, precipitating progressive chondromalacia and secondary osteoarthritis.
Prevention and Biomechanics:
The joint must be opened using leverage, varus/valgus stress, or axial traction before instrument advancement. The arthroscope should slide effortlessly into the created space. The use of a thigh post or leg holder during knee surgery, and dedicated traction/distraction devices during shoulder, hip, and ankle procedures, is biomechanically essential to open the joint space.
Crucially, once the arthroscope is inserted between articular surfaces, distraction must be maintained. If distraction is released while the scope is intraarticular, withdrawing the scope will drag the metal sheath across the cartilage, causing severe linear scoring.
Damage to Menisci and the Infrapatellar Fat Pad
A poorly placed portal exponentially increases the difficulty of instrument passage and maneuverability. It is always preferable to abandon a suboptimal portal and establish an accessory portal rather than forcing instruments and causing iatrogenic damage.
The anterior horns of the medial or lateral menisci can be inadvertently incised or penetrated if the standard anteromedial or anterolateral portals are established too inferiorly. Conversely, if the portals are placed too centrally (too close to the patellar tendon), they will traverse the thickest portion of the infrapatellar fat pad. Repeated penetration and instrument toggling within the fat pad causes acute hemorrhage, visual obstruction, and subsequent hypertrophy or dense fibrosis (Hoffa's syndrome).
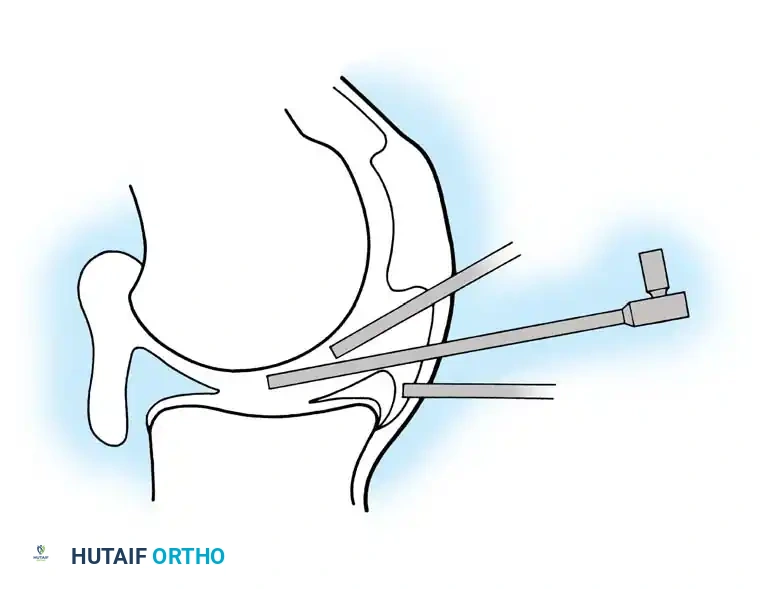
Fig. 47-10: Ideal placement of the cannula. If positioned too high, the angle of obliquity prevents visualization of the posterior horn. If positioned too low, the cannula penetrates the meniscus, limiting mobility and causing iatrogenic damage. Ideal placement is directly in the soft spot between the femur and tibia.
Cruciate Ligament Trauma
The anterior and posterior cruciate ligaments are at risk during aggressive meniscal excision, particularly when releasing the posterior horn intercondylar attachments. During ACL or PCL reconstructions, the intact reciprocal cruciate ligament is highly susceptible to iatrogenic injury when motorized shavers or burrs are utilized to aggressively debride the intercondylar notch (notchplasty).
EXTRAARTICULAR COMPLICATIONS: NEUROVASCULAR INJURY
Vascular Injuries: The Most Devastating Complication
Damage to major blood vessels around the joint is the most catastrophic arthroscopic complication, potentially leading to limb loss. Vascular injury typically occurs via direct penetration (scalpel, trocar, or motorized instrument) but can also result from mechanical compression secondary to massive fluid extravasation.
Knee: The popliteal artery is at extreme risk during posterior horn meniscectomy or meniscal repair. The artery lies immediately posterior to the capsule. Blind use of arthroscopic knives or aggressive motorized shaving near the posterior capsule can result in direct laceration. During inside-out meniscal repairs, both the popliteal artery and vein have been captured or lacerated by suture needles exiting posteriorly.
Surgical Prevention: Most surgeons now mandate a formal posteromedial or posterolateral safety incision for inside-out repairs. This involves blunt dissection down to the capsule and the placement of a broad retractor (e.g., a spoon or popliteal retractor) to physically shield the neurovascular bundle before passing needles. Furthermore, extensive arthroscopic synovectomies have been associated with injury to the genicular arteries, leading to postoperative arteriovenous fistulas or pseudoaneurysms.
Ankle: The anterior tibial artery is highly vulnerable during anterior approaches for ankle arthroscopy, particularly with the anterocentral portal, which is now largely abandoned. Posteromedial portals are similarly contraindicated due to the immediate proximity of the posterior tibial artery.
Elbow: The brachial artery may be lacerated during the establishment of anteromedial or anterolateral portals. Furthermore, high-pressure fluid extravasation can rapidly compress this vessel within the tight antecubital fossa, leading to acute compartment syndrome.
Shoulder: The axillary artery may be injured if an instrument plunges errantly through the inferior axillary pouch. More commonly, axillary vessel occlusion is secondary to massive fluid extravasation or excessive, prolonged arm traction. Additionally, the acromial branch of the coracoacromial artery is frequently transected lateral to the AC joint during arthroscopic subacromial decompression and coracoacromial ligament resection, requiring meticulous electrocautery.
Neurological Injuries
Nerve injuries manifest through several mechanisms: direct sharp trauma (scalpel/trocar), traction neurapraxia (overdistraction), mechanical compression (fluid extravasation or tourniquet ischemia), or complex regional pain syndrome (CRPS).
Step-by-Step Prevention of Nerve Injury:
1. Superficial Incision: Use a #11 blade to incise only the epidermis and dermis. Never plunge the scalpel into the subcutaneous tissue.
2. Blunt Dissection: Use a small hemostat to bluntly spread the subcutaneous tissues and capsule before introducing the cannula.
3. Blunt Trocars: Routinely use blunt (conical) trocars rather than sharp trocars to enter the joint space.
4. Padding and Positioning: Meticulously pad all bony prominences (e.g., the fibular head to protect the common peroneal nerve).
Knee: The infrapatellar branch of the saphenous nerve and the sartorial branches of the femoral nerve are the most frequently injured cutaneous nerves. Their anatomical variability means occasional injury may be unavoidable, particularly with accessory portals. While usually resulting in benign localized hypesthesia, painful neuromas can form, requiring surgical excision. Increased utilization of protective posteromedial/posterolateral incisions has dramatically reduced saphenous and peroneal nerve injuries during meniscal repairs.
Shoulder: The axillary nerve, coursing along the deep surface of the deltoid, is at risk if anterior or posterior portals are placed too inferiorly. Traction neurapraxia of the brachial plexus is a significant risk during shoulder arthroscopy in the lateral decubitus position.
Surgical Warning: The position that places maximal traction stress on the brachial plexus is 30 degrees of forward elevation combined with 70 degrees of abduction. Traction weight should be minimized (typically 10-15 lbs) and carefully monitored.
Elbow: Neurovascular injury is the primary risk of elbow arthroscopy. Anterior portals endanger the radial and posterior interosseous nerves laterally, and the median nerve medially. Posteromedial portals place the ulnar nerve at direct risk. Nerve palsies post-elbow arthroscopy are usually transient, often resulting from local anesthetic diffusion, tourniquet ischemia, or blunt contusion. Rheumatoid arthritis and severe flexion contractures are significant risk factors for temporary nerve palsy due to altered anatomical landmarks.
LIGAMENTOUS, TENDINOUS, AND SOFT TISSUE COMPLICATIONS
Iatrogenic Ligament and Tendon Tears
Knee: The medial collateral ligament (MCL) can be inadvertently lacerated by accessory medial portals. More commonly, it is ruptured by the application of severe, uncontrolled valgus stress in an attempt to open a tight medial compartment. This risk is magnified when a rigid thigh holder is used, acting as a fixed fulcrum.
Shoulder: Superior portals traversing the lateral aspect of the rotator cuff must be avoided. Passing large cannulas through the tendinous portions of the supraspinatus or infraspinatus can cause significant fraying, structural rupture, or dense scarring that precipitates secondary subacromial impingement.
Ankle and Knee Tendons: During ankle arthroscopy, the anterior tibial, peroneal, and extensor digitorum longus tendons must be carefully mapped and avoided. In the knee, the patellar tendon can be damaged by repeated, rough passage of instruments through a transpatellar (central) portal. If a transpatellar approach is mandatory, the tendon incision must be made strictly vertically, parallel to the collagen fibers, to minimize structural trauma.
Fluid Extravasation and Compartment Syndrome
Extravasation of pressurized irrigating solution into the periarticular soft tissues is ubiquitous. While usually benign and self-absorbing, the potential for catastrophic compartment syndrome must be recognized.
This is particularly dangerous in shoulder arthroscopy, where portals traverse thick muscular envelopes and bursae. Massive extravasation can compress the neurovascular bundle within the axilla, resulting in vascular compromise or severe brachial plexopathy.
In the knee, Noyes and Spievack demonstrated that rupture of the suprapatellar pouch is frequent during high-pressure arthroscopy. Fluid can dissect along the superficial femoral artery directly into the femoral triangle. Similarly, rupture of a semimembranosus bursa allows fluid to dissect deep into the fascial compartments of the calf, mimicking or causing acute compartment syndrome.
Prevention: Tense, high-pressure distention of the knee must be avoided, especially when the knee is maintained in deep flexion (which increases intraarticular pressure). Automated pressure-controlled inflow pumps must be carefully monitored, typically keeping pressures below 40-50 mm Hg unless transiently needed for hemostasis.
POSTOPERATIVE COMPLICATIONS AND PROTOCOLS
Hemarthrosis
Hemarthrosis is the most frequent postoperative complication, occurring most commonly following lateral retinacular releases and extensive synovectomies.
* Pathoanatomy: The superior lateral geniculate artery is routinely transected during a lateral retinacular release. The inferior lateral geniculate artery is vulnerable just anterior to the popliteal hiatus during lateral meniscectomy.
* Management Protocol: While small effusions are managed with rest, ice, and compression, a tense, painful, and persistent unexplained hemarthrosis requires immediate evaluation. Appropriate vascular studies (Doppler ultrasound or CT angiography) and hematological clotting profiles should be obtained. Aspiration may be required to relieve pain and prevent capsular stretching, followed by a compressive Jones dressing.
Thromboembolic Disease (DVT and PE)
Deep vein thrombosis (DVT) and pulmonary embolism (PE) are potentially lethal complications. Fortunately, their incidence is low following routine arthroscopy (0.13% to 0.17% clinically symptomatic). However, venographic studies by Stringer et al. revealed asymptomatic DVT in up to 4.2% of patients post-knee arthroscopy.
* Postoperative Protocol: Routine chemical prophylaxis is not universally mandated for simple arthroscopy in healthy patients. However, mechanical prophylaxis (early mobilization, ankle pumps) is essential. Chemical prophylaxis (e.g., LMWH or direct oral anticoagulants) should be strongly considered for high-risk patients (history of VTE, oral contraceptive use, obesity, or prolonged procedures requiring extended tourniquet times).
Conclusion
The mastery of arthroscopic surgery requires far more than technical dexterity; it demands a profound respect for anatomy and an unwavering commitment to safety protocols. By anticipating anatomical pitfalls, utilizing meticulous portal placement techniques, and respecting the biomechanical limits of joint distraction and fluid pressure, the orthopedic surgeon can effectively eliminate the vast majority of arthroscopic complications.
You Might Also Like

