INTRODUCTION TO ARTHROSCOPIC COMPLICATIONS
Complications during or after arthroscopy are infrequent and, fortunately, are usually minor in severity. However, the minimally invasive nature of arthroscopic surgery can sometimes lull the unwary surgeon into a false sense of security. Most complications are entirely preventable with rigorous preoperative and intraoperative planning, coupled with an uncompromising attention to the details of basic surgical techniques.
Mastery of local and regional anatomy is the cornerstone of safe arthroscopy. Furthermore, gaining familiarity with new techniques through accredited learning centers, operating alongside experienced colleagues, reviewing surgical videos, and staying current with peer-reviewed specialty journals allows the surgeon to assimilate valuable information from the collective experiences of the orthopedic community.
Clinical Pearl: The most effective management of an arthroscopic complication is its absolute prevention. A deep, three-dimensional understanding of joint anatomy and the biomechanical behavior of arthroscopic instruments is non-negotiable for the operating surgeon.
PREOPERATIVE PLANNING AND SITE VERIFICATION
Before any operative procedure commences, having all comprehensive office notes, advanced imaging (MRI/CT), and plain radiographs available in the operating room is mandatory. The cognitive rehearsal of the procedure, including the anticipation of potential anatomical variants, significantly reduces intraoperative errors.
The Universal Protocol and Wrong-Site Surgery Prevention
Wrong-site surgery remains a catastrophic, yet preventable, "never event" in orthopedic surgery. Before entering the operating room, the surgeon must review the surgical procedure directly with the patient. Historically, having the patient write the word “wrong” on the nonoperative extremity was utilized to alleviate possible confusion on a long, fatiguing operative day. Today, standardized protocols have superseded this practice.
The Sign Your Site program initiated by the American Academy of Orthopaedic Surgeons (AAOS) and the Universal Protocol recommendations mandated by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) dictate a strict sequence of preoperative verification. This includes:
* Preoperative verification of the operative site with the awake patient.
* Unambiguous marking of the operative site by the attending surgeon using a permanent marker.
* A formal, structured “time out” immediately before the incision, involving the entire surgical, anesthesia, and nursing team.
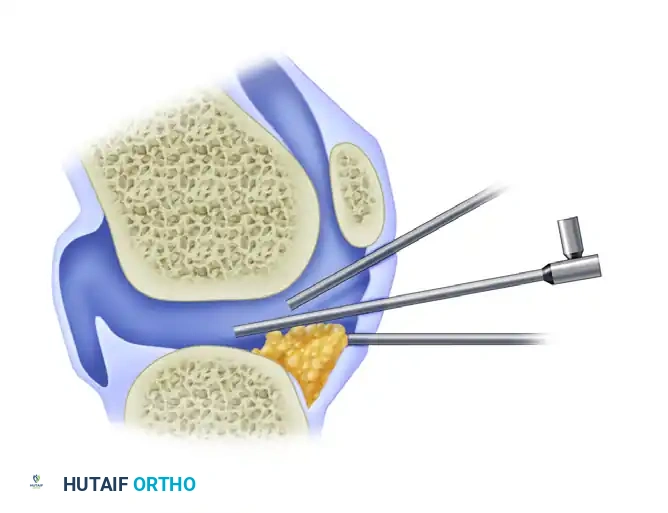
FIGURE 49-9: The operative extremity has been clearly marked by the surgeon prior to draping, adhering to the Universal Protocol to prevent wrong-site surgery.
INTRAOPERATIVE FUNDAMENTALS: PORTAL PLACEMENT AND BIOMECHANICS
The genesis of many arthroscopic complications—ranging from iatrogenic cartilage damage to poor visualization—lies in suboptimal portal placement. Portals must be established with precision, respecting the underlying intra-articular structures and the trajectory required for instrumentation.
The Biomechanics of Cannula Trajectory
When establishing portals, particularly the standard anterolateral and anteromedial portals in the knee, the angle of obliquity is critical. The ideal placement of the cannula or trocar is directly in the anatomical "slot" between the femoral condyle and the tibial plateau.
Surgical Pitfall: If the portal is positioned too high (superiorly), the angle of obliquity becomes too steep. This trajectory causes the instruments to abut the femoral condyle, making it biomechanically impossible to visualize or instrument the posterior horn of the meniscus. Conversely, if the portal is placed too low (inferiorly), the cannula can inadvertently penetrate directly through the anterior horn of the meniscus, causing iatrogenic tearing and severely limiting both the field of view and the mobility of the arthroscope.

FIGURE 49-10: Ideal placement of the cannula. If it is positioned too high, the angle of obliquity is such that the posterior horn cannot be seen; if it is too low, the cannula can go through the meniscus and limit view or mobility. Ideal placement is directly in the slot between the femur and tibia.
To avoid these complications, portals should be marked appropriately before the joint is distended. The surgeon must ensure that the scalpel penetrates the skin only (using a #11 blade). Subsequently, a hemostat should be used to spread the subcutaneous tissues down to the joint capsule, pushing away superficial nerves and vessels. Finally, blunt trocars should be routinely used to enter the joint capsule to prevent scuffing of the articular cartilage.
FLUID MANAGEMENT AND COMPARTMENT SYNDROMES
Arthroscopy relies on fluid distention to maintain the optical cavity and provide hemostasis. However, increased compartment pressure may occur during surgery from fluid extravasation into the surrounding soft tissues. This must be vigilantly monitored during all extensive procedures, particularly those involving capsular releases, extra-articular procedures, or prolonged operative times.
Pathophysiology of Fluid Extravasation
Fluid can escape the joint capsule through portal sites, iatrogenic capsular rents, or anatomical weak points (such as the popliteus hiatus in the knee). When fluid accumulates in the fascial compartments of the extremity, interstitial pressure rises. If this pressure surpasses the capillary perfusion pressure, tissue ischemia ensues, leading to a surgical emergency: compartment syndrome.
Prevention and Intraoperative Management
By utilizing gravity inflow or maintaining lower automated pump pressures (typically 30–40 mm Hg for the knee, adjusted for mean arterial pressure) and ensuring adequate fluid outflow, the vast majority of extravasation complications can be avoided.
If excessive extravasation is noted intraoperatively (manifesting as severe swelling, induration, and loss of palpable landmarks), the following step-by-step protocol must be initiated:
1. Halt Inflow: Immediately stop the fluid inflow and assess the joint.
2. Decompress: Release any constricting dressings, drapes, or tourniquets.
3. Positional Drainage: Place the extremity at the level of the heart to optimize venous and lymphatic return without compromising arterial inflow.
4. Mechanical Milking: Wrap the extremity with an Esmarch bandage from distal to proximal, and then remove it. This technique mechanically forces the extravasated fluid out of the interstitial spaces and back toward the joint or systemic circulation.
Surgical Warning: Persistence of elevated compartment pressure despite these maneuvers is a dire warning sign. The extremity must be formally evaluated using a compartment pressure monitor. If pressures remain within 30 mm Hg of the patient's diastolic blood pressure (Δp ≤ 30 mm Hg), emergent fasciotomy is indicated following established guidelines for acute compartment syndrome.
NEUROLOGICAL COMPLICATIONS
Nerve injuries in arthroscopy are rare but can lead to profound postoperative morbidity, chronic pain, and litigation. The mechanisms of nerve injury are multifactorial and include:
* Direct Trauma: Laceration or contusion from a scalpel, sharp trocar, or motorized shaver.
* Traction: Neurapraxia resulting from overdistraction of the joint.
* Compression: Mechanical compression from instruments, positioning devices (e.g., thigh posts), or fluid extravasation.
* Ischemia: Prolonged ischemia from excessive or uncalibrated tourniquet use.
* Complex Regional Pain Syndrome (CRPS): Formerly known as reflex sympathetic dystrophy (RSD), this can arise from a poorly defined mechanism of injury to the anatomical nervous system following even minor cutaneous nerve damage.
Prevention Strategies
Many of these complications can be avoided by adhering to strict surgical principles:
* Marking portals accurately based on palpable bony landmarks.
* Using a "skin-only" incision technique.
* Spreading subcutaneous tissues bluntly with a hemostat.
* Routinely utilizing blunt trocars for capsular penetration.
* Maintaining proper joint distention and avoiding excessive mechanical distraction.
* Meticulously padding all nerve and bony prominences during patient positioning.
* Minimizing tourniquet time through improved surgical technique and anatomical familiarity.
Nerve Injuries in Knee Arthroscopy
Sensory and motor nerves near the knee joint are at risk during portal creation and instrumentation. The inferior branches of the saphenous nerve (specifically the infrapatellar branch) and the sartorial branches of the femoral nerve are the most commonly injured cutaneous nerves.
The anatomical location of these numerous cutaneous branches is highly variable; therefore, occasional injury to a small terminal branch may be unavoidable, especially if multiple accessory portals are utilized. In most instances, the resulting hypesthesia is of minor clinical consequence and causes no functional deficit. However, on occasion, a painful neuroma may develop, requiring subsequent surgical resection and burying of the nerve stump into muscle or bone.
Historical Context and Incidence:
In Small’s landmark retrospective report, 229 nerve injuries were reported across a massive cohort of knee arthroscopies. Specifically, 30 saphenous nerve injuries and six peroneal nerve injuries were reported in 3,034 meniscal repairs. The peroneal nerve is particularly vulnerable during inside-out lateral meniscal repairs if the posterior retractor is not positioned correctly anterior to the lateral head of the gastrocnemius.
Increased surgical experience with meniscal repairs, combined with improved anatomical techniques (especially the use of formal posteromedial or posterolateral safety incisions and exposures), has dramatically lowered the incidence of nerve injury. In Small’s second series, the incidence dropped to a single saphenous nerve injury in 310 meniscal repairs, highlighting the importance of evolving surgical techniques.
Nerve Injuries in Shoulder Arthroscopy
Shoulder arthroscopy presents its own unique set of neurological hazards, primarily involving the axillary nerve and the brachial plexus.
The Axillary Nerve:
During shoulder arthroscopy, the branches of the axillary nerve that course along the deep surface of the deltoid muscle (approximately 5 cm distal to the lateral acromial edge) may be injured if either the anterior or posterior portal sites are placed too far inferiorly. The standard posterior portal should be placed 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion to stay well within the "safe zone."
Brachial Plexus Traction Neurapraxia:
Traction neurapraxia of the brachial plexus is a significant risk when strong traction and distraction of the shoulder are employed, particularly in the lateral decubitus position. The biomechanical position that appears to result in the greatest traction tension on the brachial plexus is 30 degrees of forward elevation combined with 70 degrees of abduction. Surgeons must carefully monitor the amount of weight used for traction (typically not exceeding 10-15 lbs) and ensure the head and neck are maintained in a neutral position to avoid stretching the contralateral plexus.
In 1986, Small reported one axillary nerve injury and three brachial plexus injuries in 14,329 shoulder arthroscopies. By 1988, reflecting improved positioning protocols and heightened awareness, there were zero nerve injuries reported in 1,184 shoulder procedures.
VASCULAR COMPLICATIONS
While major vascular injuries are exceedingly rare, they represent limb-threatening emergencies.
In shoulder arthroscopy, the cephalic vein, which lies in the deltopectoral groove, may be penetrated or lacerated by poor anterior portal site selection. The anterior portal should be established using an outside-in technique with a spinal needle, or an inside-out technique originating from the posterior portal, ensuring the trajectory remains lateral to the coracoid process to avoid the cephalic vein and the deeper neurovascular bundle.
In knee arthroscopy, the popliteal artery is at risk during posterior horn meniscectomies, posterior capsular releases, or when establishing posteromedial/posterolateral portals. The use of motorized shavers without direct visualization in the posterior compartment is strictly contraindicated. Arthroscopic obstruction of view by hypertrophic synovium or fat pad must be cleared meticulously; blind instrumentation may result in catastrophic hemorrhage, or subsequent hypertrophy and fibrosis of the injured structures.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The prevention of complications extends into the postoperative period. Immediate Post-Anesthesia Care Unit (PACU) monitoring must include a thorough neurovascular assessment of the operative extremity.
- Vascular Assessment: Capillary refill, distal pulses, and compartment compressibility must be documented.
- Neurological Assessment: Motor function and sensory distribution of the major peripheral nerves must be verified before discharge.
- Pain Management: Disproportionate postoperative pain that is unresponsive to standard analgesia is a red flag. It may indicate impending compartment syndrome or the early onset of Complex Regional Pain Syndrome (CRPS).
Early mobilization, aggressive edema control (using cryotherapy and compression), and structured physical therapy are essential to prevent arthrofibrosis and deep vein thrombosis (DVT). By adhering to these rigorous, evidence-based protocols, the orthopedic surgeon can ensure that arthroscopy remains a safe, highly effective intervention with minimal morbidity.
