Comprehensive Introduction and Patho-Epidemiology
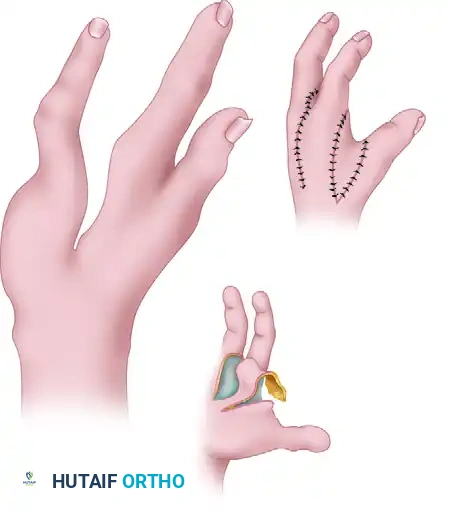
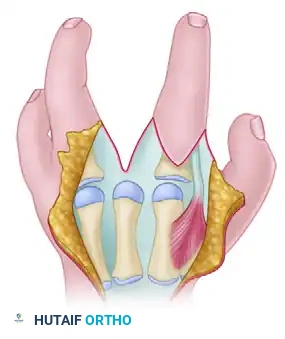
Congenital cleft hand, historically and somewhat pejoratively termed ectrodactyly or "split hand," represents a profound longitudinal deficiency of the central rays of the hand. This complex malformation is fundamentally characterized by a deep, V-shaped central defect that physically and functionally divides the hand into radial and ulnar borders. The pathoanatomy is not merely a cosmetic absence of digits; it is a profound structural collapse. A frequent, functionally debilitating, and nearly ubiquitous component of the typical cleft hand anomaly is the severe thumb adduction contracture. The absence of the central metacarpals (most commonly the third ray) critically compromises the transverse metacarpal arch. Without this keystone structural support, the hand undergoes a biomechanical collapse. Over time, the adductor pollicis and the first dorsal interosseous muscles undergo severe, progressive contracture, relentlessly tethering the thumb to the index ray and effectively obliterating the first web space.
The embryological basis of the typical cleft hand is rooted in a central failure of the apical ectodermal ridge (AER) during the critical window of upper limb development, which occurs between the fourth and eighth weeks of gestation. The AER is the primary signaling center responsible for the proximodistal outgrowth and patterning of the limb bud. A wedge-shaped defect in the AER leads to the failure of mesenchymal condensation and subsequent chondrogenesis of the central rays. Genetically, this defect is frequently inherited in an autosomal dominant pattern with highly variable penetrance and expressivity. Mutations in the DLX5 and DLX6 genes, as well as aberrations in the WNT and SHH (Sonic Hedgehog) signaling pathways, have been heavily implicated in the pathogenesis of this central failure. Furthermore, the typical cleft hand is frequently bilateral and is often associated with syndromic presentations, the most notable being EEC syndrome (Ectrodactyly, Ectodermal dysplasia, and Cleft lip/palate) and SHFM (Split Hand/Foot Malformation) loci.
Epidemiologically, the true congenital cleft hand is a rare anomaly, with an estimated incidence ranging from 1 in 10,000 to 1 in 90,000 live births, depending on the specific demographic and genetic isolate being studied. It is crucial to clinically differentiate the "typical" cleft hand from the "atypical" cleft hand (symbrachydactyly). The typical cleft hand presents with a central V-shaped defect, frequently involves the feet, has a strong genetic component, and features the hallmark thumb adduction contracture. In stark contrast, the atypical cleft hand (symbrachydactyly) presents as a U-shaped defect, is almost always unilateral, lacks a clear genetic inheritance pattern, rarely involves the feet, and frequently presents with rudimentary nubbins rather than fully formed border digits. Recognizing this distinction is paramount, as the surgical algorithms, particularly the indications for central ray closure and thumb adduction release, differ drastically between the two entities.
The primary goals of surgical intervention in the typical cleft hand are intrinsically linked to functional restoration and aesthetic normalization. Functionally, the surgeon must deepen the first web space to restore thumb opposition, palmar abduction, and functional pinch kinematics. A hand with a tethered thumb is relegated to rudimentary side-to-side pinch, severely limiting fine motor dexterity. Aesthetically, closing the central cleft normalizes the appearance of the hand, which carries immense psychosocial importance for the developing child. Achieving these dual goals requires a complex, multi-planar reconstruction involving the ulnar transposition of the index ray to the base of the third metacarpal, combined with a radical, meticulous soft-tissue release of the first web space.
Detailed Surgical Anatomy and Biomechanics
Osteology and the Transverse Metacarpal Arch
The osteological architecture of the cleft hand is highly variable, demanding a thorough understanding of normal and aberrant anatomy. In a normal hand, the bases of the second and third metacarpals are rigidly fixed to the trapezoid and capitate, forming the stable central pillar of the hand. The transverse metacarpal arch is the structural keystone that allows the mobile radial (thumb) and ulnar (ring and small fingers) borders to oppose each other. In the cleft hand, the absence of the third metacarpal destroys this arch. The second metacarpal often drifts ulnarly, or conversely, the thumb and index ray collapse toward each other due to the unopposed pull of the adductor musculature. When transposing the index ray to the third metacarpal position, the surgeon must evaluate the presence of the third metacarpal base. If a hypoplastic base is present, it serves as an excellent foundation for a peg-in-hole osteosynthesis. If absent, the index metacarpal must be transposed and articulated directly with the capitate, requiring meticulous capsular reconstruction to ensure stability.
Muscular and Fascial Pathoanatomy
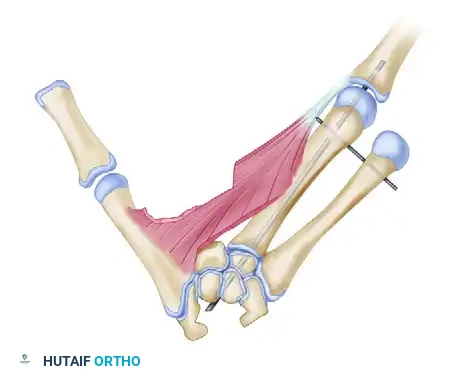
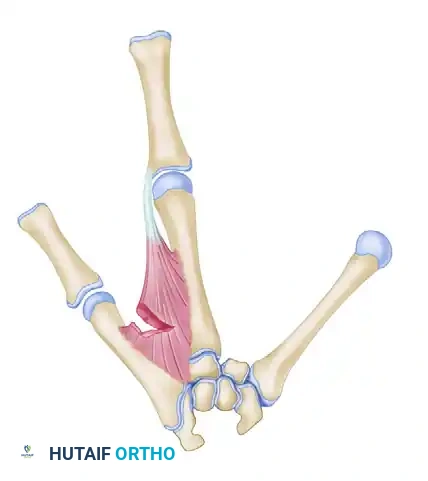
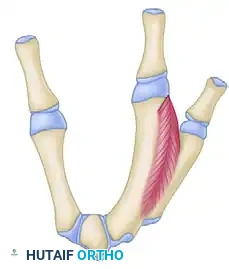
The muscular anatomy in the cleft hand is characterized by severe contracture and frequent anomalous insertions. The adductor pollicis, comprising both its transverse and oblique heads, is the primary deforming force driving the thumb adduction contracture. In the cleft hand, these muscle bellies are structurally shortened and often fibrotic. Similarly, the first dorsal interosseous muscle, which normally originates from the adjacent shafts of the first and second metacarpals, is severely contracted, acting as a secondary tether. The fascial envelopes surrounding these muscles, particularly the interosseous fascia and the deep palmar fascia, are thickened and unforgiving. Surgical release requires not just a superficial fasciotomy, but a profound, sequential release. This often necessitates detaching the origins of the first dorsal interosseous from the metacarpals and elevating the adductor pollicis and the radial belly of the flexor pollicis brevis from their origins to achieve adequate palmar abduction.
Neurovascular Aberrations
The neurovascular anatomy of the congenital cleft hand is notoriously unpredictable, making dissection perilous. The superficial palmar arch is frequently incomplete or entirely absent, with the digits relying heavily on a dominant dorsal arterial supply or anomalous branches from the deep palmar arch. The radial artery, as it dives between the two heads of the first dorsal interosseous muscle to form the deep palmar arch, is at extreme risk during the adductor release. The digital nerves also exhibit anomalous branching patterns. The common digital nerve to the cleft often bifurcates proximally or presents with cross-connections (ramus communicans) that span the cleft. Meticulous loupe magnification and a bloodless field via pneumatic tourniquet are absolute prerequisites. The viability of the local transposition flaps, particularly the palmar-based flap in the Snow and Littler technique, relies entirely on preserving the delicate subdermal venous plexus, as formal venous outflow tracts are often disrupted during the cleft closure.
Kinematics and Index Ray Supination
The biomechanics of the transposed index ray dictate the functional success of the procedure. When the index metacarpal is osteotomized and shifted ulnarly to the third metacarpal position, it cannot simply be translated in a two-dimensional plane. The normal flexion axis of the digits points toward the scaphoid tubercle. If the index ray is merely translated ulnarly without rotational correction, its flexion axis will intersect with the ring finger, leading to debilitating digital overlap (scissoring) during grip. Therefore, the transposed digit must be supinated—often up to 45 degrees—to realign its flexion axis. This supination ensures that the transposed index finger flexes symmetrically into the palm alongside the ring finger, restoring a functional, non-interfering kinematic chain.
Exhaustive Indications and Contraindications
The decision to proceed with a combined cleft closure and thumb adduction contracture release requires a nuanced assessment of the patient's functional deficits, the anatomical severity of the cleft, and the psychosocial needs of the family. The Manske and Halikis classification of cleft hands, which categorizes the anomaly based on the severity of the first web space narrowing (Types I through V), is the standard framework guiding these surgical indications.
Surgical intervention is definitively indicated for patients with Manske Types II (narrowed first web space), III (syndactylized first web space), and IV (merged first web space) cleft hands. In these patients, the thumb adduction contracture precludes functional opposition and large object grasp. The primary indication is the restoration of the kinematic pinch mechanism. A secondary, yet highly significant indication is the prevention of progressive deformity. As the child grows, the unopposed adductor forces will exacerbate the structural collapse of the metacarpal arch, leading to fixed secondary joint contractures at the carpometacarpal (CMC) and metacarpophalangeal (MCP) joints. Furthermore, the psychosocial impact of a severe cleft hand cannot be understated; early aesthetic reconstruction (typically between 12 and 18 months of age) allows the child to integrate into social and educational environments with normalized hand morphology before body image awareness fully develops.
Contraindications must be rigorously respected to avoid catastrophic functional loss. Absolute contraindications include severe medical comorbidities that preclude safe general anesthesia, and critically, an inadequate local vascular supply. If preoperative vascular mapping indicates that the border digits rely on a single, tenuous collateral vessel that crosses the planned osteotomy or cleft closure site, the procedure is absolutely contraindicated, as transposition will inevitably lead to digital ischemia and necrosis. Relative contraindications include Manske Type I hands (normal first web space), where the functional deficit is minimal and the risks of surgery may outweigh the cosmetic benefits. Additionally, severe Manske Type V hands (absent thumb) require complete pollicization rather than a simple adduction release.
| Category | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Functional | Inability to perform opposition or wide grasp; severe thumb adduction contracture (Manske Types II-IV); progressive collapse of the transverse metacarpal arch. | Manske Type I (normal web space, excellent function); Manske Type V (requires formal pollicization); isolated atypical clefts with stable pinch. |
| Anatomical | Presence of a functional index ray capable of transposition; adequate bone stock at the 2nd/3rd metacarpal bases; syndactyly of the border digits requiring release. | Absent or critically hypoplastic index ray; severe joint stiffness precluding functional ROM post-transposition; anomalous neurovascular bundle crossing the cleft that cannot be safely mobilized. |
| Vascular | Intact, redundant arterial supply to the thumb and index fingers; robust dorsal venous drainage capable of supporting local transposition flaps. | Absolute: Single-vessel dominant supply to the radial digits that would be stretched or kinked during transposition; severe venous insufficiency. |
| Psychosocial & Timing | Age 12-18 months (optimal for cortical integration of new motor patterns); strong family support for rigorous postoperative rehabilitation. | Medically unstable infant; non-compliant family structure incapable of managing complex postoperative casting and splinting protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Assessment and Vascular Mapping
A meticulous, exhaustive preoperative clinical evaluation is the foundation of a successful cleft hand reconstruction. The surgeon must assess the passive and active range of motion of the thumb, specifically quantifying the degree of palmar abduction and opposition. The severity of the adduction contracture dictates the extent of the necessary muscular release. Any concomitant syndactyly between the remaining digits must be documented, as its release may need to be staged to prevent vascular compromise. Crucially, the vascular status of the hand must be evaluated. Because congenital anomalies frequently present with aberrant arterial arches, a modified Allen test (if feasible in the pediatric patient) or a hand-held Doppler ultrasound examination is mandatory to map the arterial supply to the thumb and index finger. The surgeon must confirm that the index ray can be mobilized ulnarly without tethering or kinking its dominant arterial inflow.
Radiographic Planning and Templating
Standard posteroanterior (PA), lateral, and oblique radiographs of the hand are required. Advanced imaging, such as an MRI or CT scan, is rarely indicated unless there is a suspicion of a complex carpal coalition or a hidden cartilaginous anlage. The surgeon must meticulously evaluate the presence, size, and morphology of the third metacarpal base. This structure will serve as the foundation for the transposed index ray. Radiographic templating is performed to determine the exact level and angle of the index metacarpal osteotomy. The surgeon must calculate the required length of the index metacarpal to ensure that, once transposed, the metacarpal heads align in a smooth, cascading transverse arch. Failure to template accurately can result in a transposed index finger that is either excessively long or short, disrupting the flexor cascade and compromising grip strength.
Timing of Surgical Intervention
The timing of the combined cleft closure and thumb adduction release is a critical variable. The consensus among pediatric hand surgeons is to perform this reconstruction between 12 and 18 months of age. Intervening during this window leverages the immense neuroplasticity of the infant brain, allowing the child to incorporate the newly reconstructed thumb and transposed index finger into their developing fine motor patterns and cortical homunculus. Delaying surgery beyond 2 to 3 years of age allows abnormal compensatory pinch patterns (such as a side-to-side key pinch between the thumb and ring finger) to become deeply ingrained, making postoperative functional rehabilitation significantly more challenging. Furthermore, early intervention prevents the progressive, secondary capsular contractures of the CMC joint that occur due to prolonged adductor tethering.
Patient Positioning and Anesthesia
The procedure is performed under general anesthesia, supplemented with a regional brachial plexus block (usually supraclavicular or axillary) to provide profound intraoperative vasodilation and preemptive postoperative analgesia. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pediatric pneumatic tourniquet is applied to the proximal arm. Exsanguination is achieved via elevation or a sterile Esmarch bandage, and the tourniquet is inflated to age- and weight-appropriate pressures (typically 150-200 mmHg). The surgeon sits in the axilla, utilizing loupe magnification (minimum 3.5x to 4.5x) and a sterile micro-instrumentation set. A mini-C-arm fluoroscopy unit must be positioned perpendicular to the hand table, readily available for intraoperative imaging during the osteotomy and K-wire fixation phases.
Step-by-Step Surgical Approach and Fixation Technique
The two most prominent, evidence-based techniques for this complex reconstruction are the Snow and Littler technique and the Miura and Komada technique. The choice between these methods depends on the specific geometry of the cleft, the pliability of the palmar skin, and the surgeon's preference for flap design.
Surgical Technique 1: The Snow and Littler Method
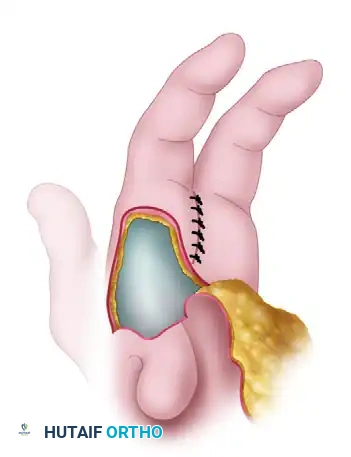
The Snow and Littler technique is a masterclass in local tissue rearrangement. It utilizes a broad, robust palmar-based flap to reconstruct the first web space while simultaneously transposing the index ray to close the central cleft. This technique is particularly advantageous when there is a deep, wide cleft and severe thumb adduction contracture requiring massive tissue interposition.
1. Incision and Flap Design
The procedure begins with precise geometric planning of the skin incisions to ensure adequate coverage of the newly created web space without tension. The dorsal cleft incision outlines the sides of the cleft on the dorsal surfaces of the index and ring fingers. These incisions are joined proximally so that the V-shaped apex extends just proximal to the level of the metacarpal heads. A small, straight incision is made on the ulnar side of the index finger to accommodate a small commissure flap raised on the radial side of the ring finger, recreating a natural-appearing web.
As the incisions pass the metacarpal heads, they are curved proximally onto the palm. These palmar incisions must run almost parallel to each other, lying slightly toward the cleft side of the midline of the two fingers. The crucial limit of this design is that the palmar incisions must not extend any farther proximally than a point directly opposite the V-shaped apex of the dorsal incision. This specific geometry creates the robust palmar flap destined to form the new thumb web.
2. Thumb Adduction Release
Releasing the tethered thumb requires meticulous deep dissection, balancing aggressive muscle release with absolute neurovascular preservation. Another incision is made on the dorsum of the thumb web at the same level as the V-shaped cleft incision, extending distally parallel with the index split incision. This creates a vital strip of dorsal skin that remains connected to the index finger and the dorsum of the hand. The viability of this split flap is entirely dependent on robust venous drainage; therefore, small dorsal veins must be preserved and never dissected off the flap.
The dissection is deepened to release the dense fibrous bands tethering the metacarpals. The origins of the first dorsal interosseous muscle are detached from the metacarpals. The adductor pollicis muscle and the radial belly of the flexor pollicis brevis are elevated from their origins. During this stage, the branches of the median nerve and the radial artery are highly vulnerable. The radial artery must be definitively identified and protected as it dives between the two heads of the first dorsal interosseous muscle. If full thumb abduction is still restricted after muscular release, a dorsal capsulotomy of the CMC joint is performed.
3. Index Ray Transposition and Osteotomy
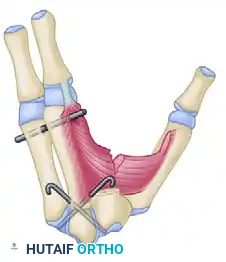
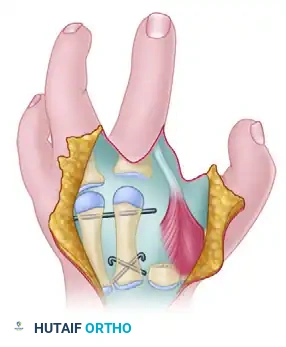
With the soft tissues completely released and the thumb fully abducted, the structural reconstruction begins. A transverse or slightly oblique osteotomy is performed at the base of the index metacarpal using an oscillating microsaw. The entire index ray is mobilized and transferred ulnarly to align with the base of the third metacarpal.
If the third metacarpal base is hypoplastic, the proximal end of the transposed index metacarpal is shaped into a peg and impaled directly into the medullary canal of the third metacarpal base. If adequate bone stock is present, the osteotomy is reduced and fixed using crossed or parallel 0.045-inch or 0.062-inch Kirschner wires (K-wires).
Rotational alignment is the most critical aspect of the osteotomy. The transposed digit must be supinated—often up to 45 degrees—to ensure its flexion axis is directed toward the scaphoid tubercle, preventing scissoring over the ring finger.
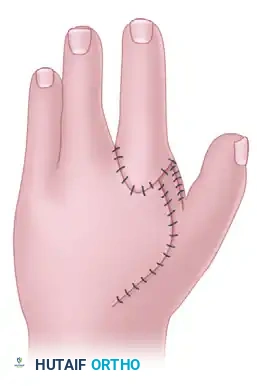
4. Wound Closure and Web Space Inset
The skin between the ring and index fingers is sutured, closing the central cleft. The small, longitudinal flap is inset into the ulnar side of the index finger to recreate a smooth, U-shaped commissure. The large palmar-based cleft flap is then transposed into the newly opened space between the index finger and the abducted thumb.

These flaps must never be placed under tension. Ischemia will lead to catastrophic flap necrosis and severe secondary contracture. If the palmar flap does not completely cover the dorsal defect, a full-thickness skin graft (often harvested from the groin) must be utilized to achieve complete, tension-free coverage.
Surgical Technique 2: The Miura and Komada Method
The Miura and Komada technique offers an alternative geometric approach to cleft hand reconstruction. It utilizes a distinct dorsal and palmar flap design that is particularly useful when the dorsal skin is highly pliable or when the surgeon desires a different vector of web space deepening.
1. Incision and Exposure
The Miura and Komada procedure begins with a precisely planned skin incision mapped on the dorsum of the hand, outlining the cleft and the planned web space.

Additional incisions (often marked as broken lines during preoperative planning) are utilized to fully expose the metacarpals dorsally and the palmar surface of the digits.

The index finger skin flaps are carefully elevated. The surgeon must ensure the subdermal vascular plexus is preserved within these flaps to maintain viability during the extensive transposition.

2. Bone Transposition and Soft Tissue Release
The core principle remains identical: the ulnar shift of the index ray to obliterate the central cleft and reconstruct the transverse arch.
To allow the index ray to shift and the thumb to abduct, the fasciae of the first dorsal interosseous and the adductor pollicis must be radically released. In severe cases, fractional lengthening or complete release of the muscle bellies from their metacarpal origins is required.
Once the osteotomy is performed and the profound muscular releases are complete, the index ray is secured to the third metacarpal base, and the thumb is brought into full palmar abduction.
3. Closure
The skin flaps are meticulously inset. The Miura and Komada design often allows for a primary closure that naturally deepens the first web space while seamlessly closing the central defect, minimizing the need for supplemental skin grafting if executed perfectly.
Complications, Incidence Rates, and Salvage Management
Orthopaedic surgeons must be hyper-vigilant regarding several high-risk complications associated with this complex, multi-tissue reconstruction. The most devastating soft-tissue complication is flap necrosis. This is almost universally iatrogenic, caused by excessive tension during closure, failure to preserve the delicate dorsal venous drainage during flap elevation, or direct arterial injury to the radial artery or dominant digital vessels during the adductor release. If flap ischemia is noted intraoperatively (evidenced by a lack of capillary refill or venous congestion after tourniquet deflation), the surgeon must immediately release all tension-bearing sutures. The defect must be allowed to open, and a full-thickness skin graft must be applied. Attempting to "wait and see" on a dusky flap in a pediatric cleft hand will result in full-thickness necrosis, profound scarring, and a recurrent contracture that is exponentially more difficult to treat.
Digital overlap, or "scissoring," is a severe biomechanical complication resulting from a failure to properly align the index ray during transposition. As previously emphasized, the index metacarpal must be supinated up to 45 degrees to align its flexion axis with the scaphoid tubercle. If the digit is merely translated ulnarly without this rotational correction, it will cross over the ring finger during active flexion, severely compromising grip strength and hand function. If scissoring is identified postoperatively, the only salvage is a secondary derotational osteotomy of the index metacarpal once the initial osteotomy has fully healed.
Recurrence of the thumb adduction contracture is a frustratingly common complication, particularly in severe Manske Type IV hands. This recurrence is often multifactorial, resulting from an initially inadequate release of the carpometacarpal joint capsule, incomplete release of the adductor origins, or failure to maintain the thumb in rigorous palmar abduction during the critical 6-week postoperative casting phase. Prevention requires aggressive intraoperative release and uncompromising postoperative splinting. Night splinting with a rigid web spacer is critical for up to 6 months postoperatively. If a severe contracture recurs, a revision release utilizing a dorsal rotational flap or a first dorsal metacarpal artery (kite) flap may be required to import healthy, vascularized tissue into the web space.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Flap Necrosis | 5% - 10% | Preserve dorsal veins; absolutely no tension on closure; use skin grafts liberally. | Immediate suture removal; debridement of necrotic tissue; full-thickness skin grafting or local rotational flaps. |
| Digital Scissoring | 10% - 15% | Supinate index ray 30-45 degrees during osteotomy fixation; assess flexion cascade intraoperatively. | Secondary derotational osteotomy of the index metacarpal at 6-12 months post-op. |
| Recurrent Contracture | 15% - 25% | Radical release of adductor and 1st dorsal interosseous; CMC capsulotomy; strict prolonged splinting. | Revision soft-tissue release; Z-plasty or regional flap (e.g., Kite flap) to deepen web space. |
| Nonunion / Delayed Union | < 2% | Precise osteotomy cuts; robust K-wire fixation (crossed or peg-in-hole); adequate immobilization. | Prolonged immobilization; if symptomatic nonunion persists, revision open reduction and internal fixation with bone grafting. |
Phased Post-Operative Rehabilitation Protocols
The technical success of a cleft hand reconstruction in the operating room is rapidly negated without strict adherence to a rigorous, phased postoperative immobilization and rehabilitation protocol. The pediatric patient presents unique challenges, as compliance cannot be reasoned with; therefore, the immobilization constructs must be inherently robust and foolproof.
Phase 1: Immobilization and Protection (Weeks 0 to 6)
Immediately postoperatively, while the patient is still under anesthesia, a bulky, well-padded long-arm cast is applied. The cast must be meticulously molded to maintain the newly reconstructed transverse and longitudinal arches of the hand. Crucially, the thumb must be immobilized in a position of maximum palmar abduction and opposition to prevent the immediate recurrence of the adduction contracture. The transposed index finger must be supported to prevent stress on the K-wires. The surgeon must ensure the distal tips of the fingers and thumb have enough freedom to allow for capillary refill checks and slight micro-motion, which aids in preventing profound flexor and extensor tendon adhesions. Sutures are typically removed at the 2-week mark. This is optimally performed under mild sedation in the clinic or via a carefully cut cast window, after which a new, equally rigid long-arm cast is applied for the remainder of the 6-week period.
Phase 2: Pin Removal and Transition (Week 6)
At approximately 6 weeks postoperatively, the patient returns to the clinic for cast removal and radiographic evaluation. Follow-up PA and lateral radiographs are obtained to confirm clinical and radiographic bone healing at the index-to-third metac
