Comprehensive Introduction and Patho-Epidemiology
The human wrist represents an evolutionary marvel of biomechanical engineering, transitioning from a primary weight-bearing structure in our quadrupedal ancestors to an incredibly sophisticated, highly mobile universal joint designed for precise spatial positioning of the hand. This transition has necessitated a complex, multi-articulated system that relies overwhelmingly on a delicate equilibrium of ligamentous tethers and precise articular congruity rather than inherent bony stability. Consequently, the wrist is extraordinarily susceptible to both acute traumatic disruption and chronic degenerative conditions, making a profound understanding of its surgical anatomy and vascularity an absolute prerequisite for any orthopedic surgeon, hand specialist, or traumatologist.
Epidemiologically, wrist trauma constitutes a massive proportion of orthopedic emergency room presentations and elective clinical practices. Distal radius fractures alone account for approximately one-sixth of all fractures evaluated in emergency departments, with a bimodal distribution affecting young males in high-energy trauma and elderly females in low-energy fragility falls. Carpal fractures, while less frequent overall, present unique diagnostic and therapeutic challenges due to their subtle radiographic appearances and tenuous vascularity. The scaphoid is the most frequently fractured carpal bone, representing 60% to 70% of all carpal fractures and predominantly affecting young, active individuals. The consequences of missed or mismanaged scaphoid fractures—namely, nonunion, avascular necrosis (AVN), and the inevitable progression to Scaphoid Nonunion Advanced Collapse (SNAC)—are functionally devastating.
Furthermore, ligamentous injuries of the carpus, particularly disruptions of the scapholunate (SL) interosseous ligament, are frequently underdiagnosed. SL tears are the most common cause of carpal instability, initiating a predictable cascade of altered kinematics that culminates in Scapholunate Advanced Collapse (SLAC). The triangular fibrocartilage complex (TFCC), the primary stabilizer of the distal radioulnar joint (DRUJ), is another frequent site of pathology, with degenerative tears ubiquitous in the aging population and traumatic tears frequently complicating distal radius fractures.
Understanding the patho-epidemiology of these conditions requires an intimate knowledge of the underlying vascular anatomy. The carpus is notoriously unforgiving of vascular insult. The retrograde intraosseous perfusion of the scaphoid and the highly variable vascularity of the lunate (predisposing to Kienböck’s disease) dictate specific surgical approaches and fixation strategies. This chapter provides an exhaustive, highly technical exploration of the osteoarticular, ligamentous, and vascular anatomy of the wrist, bridging the gap between foundational anatomical science and advanced surgical application.
Detailed Surgical Anatomy and Biomechanics
The wrist is not a single joint but a highly integrated biomechanical complex comprising the radiocarpal, midcarpal, and distal radioulnar joints. Its function is dictated by the intricate interplay of unique osseous morphology, complex capsuloligamentous networks, and a highly specific, often precarious, vascular supply.
Osteoarticular Architecture
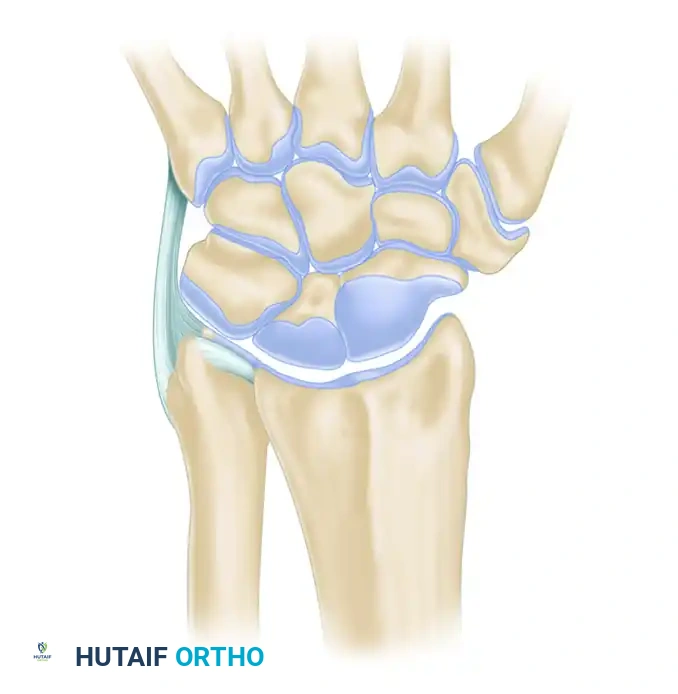
The radiocarpal joint is formed by the articulation of the biconcave distal radius (the scaphoid and lunate fossae) with the convex proximal carpal row. The proximal row—consisting of the scaphoid, lunate, and triquetrum—functions as an intercalated segment, possessing no direct tendinous insertions. Its movement is entirely passive, dictated by the mechanical forces exerted by the surrounding articulations and constrained by intrinsic and extrinsic ligaments. The triquetrum does not articulate directly with the distal ulna; rather, it articulates with the TFCC, allowing for a smooth transition of forces during ulnar deviation and forearm rotation.
The midcarpal joint represents the articulation between the proximal and distal carpal rows. The distal row (trapezium, trapezoid, capitate, and hamate) is tightly bound together by robust interosseous ligaments, functioning essentially as a single, rigid biomechanical unit that moves synchronously with the metacarpals. The capitate serves as the keystone of the carpal arch, its proximal convexity articulating deeply within the concavity formed by the scaphoid and lunate.

At the carpometacarpal (CMC) level, the distal carpal row dictates the mobility of the hand rays. The first CMC joint (trapeziometacarpal) is a highly mobile, biconcave saddle joint essential for thumb opposition. The second and third CMC joints are rigidly stable, forming the central fixed pillar of the hand, which is crucial for power pinch and grip. In contrast, the fourth and fifth CMC joints possess 15 to 30 degrees of AP mobility, permitting the hand to cup around objects and enhancing grip strength.
Distal Radioulnar Joint (DRUJ) and TFCC
The DRUJ is a diarthrodial trochoid (pivot) joint that, in conjunction with the proximal radioulnar joint (PRUJ), permits pronation and supination of the forearm. The distal ulnar convexity (ulnar head) articulates with the shallow lesser sigmoid notch of the distal radius. The radius rotates around the fixed ulna, with the sigmoid notch accommodating the ulnar head through approximately two-thirds of its rotational arc. The inherent bony stability of the DRUJ is minimal; thus, stability is overwhelmingly dependent on soft tissue constraints, primarily the TFCC.
The TFCC is a complex, multifaceted structure that serves as the primary stabilizer of the DRUJ, a load-bearing cushion for the ulnocarpal axis, and a flexible connection between the radius and ulna. It separates the hyaline cartilage-covered ulnar head from the ulnar styloid and the proximal carpal row.
The TFCC comprises several distinct components: the central articular disc (avascular and load-bearing), the dorsal and volar radioulnar ligaments (the primary stabilizers of the DRUJ), the ulnocarpal ligaments (ulnolunate and ulnotriquetral, which prevent volar subluxation of the ulnar carpus), the meniscal homologue, the ulnar collateral ligament (UCL), and the extensor carpi ulnaris (ECU) subsheath. During pronation, the dorsal radioulnar ligament tightens; during supination, the volar radioulnar ligament tightens. The central portion of the TFCC is avascular, meaning traumatic tears in this zone (Palmer Class 1A) have no healing potential and require arthroscopic debridement. Conversely, the peripheral 10-20% (the "red zone") is well-vascularized by branches of the ulnar artery and is highly amenable to primary surgical repair (Palmer Class 1B).
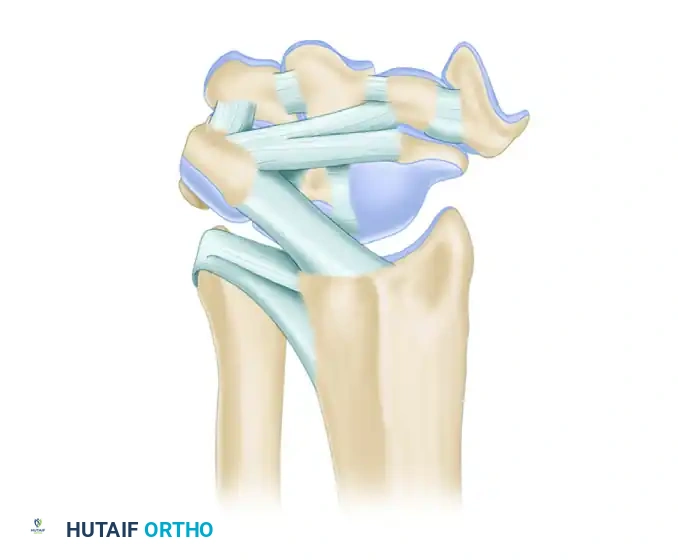
Volar (Palmar) Ligamentous Anatomy
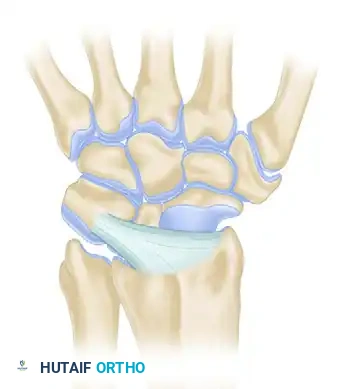
Carpal stability relies entirely on its complex ligamentous network. The palmar ligaments are substantially thicker, stiffer, and mechanically stronger than their dorsal counterparts. They are organized into a double-V configuration that guides carpal kinematics. The apex of the proximal "V" is the lunate, and the apex of the distal "V" is the capitate. The relative weakness between these ligamentous arcades creates the Space of Poirier, a potential zone of vulnerability through which the lunate can dislocate volarly during high-energy hyperextension injuries (Mayfield Stage IV).
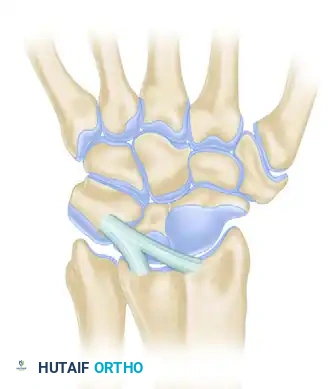
The extrinsic palmar ligaments include the radioscaphocapitate (RSC), the long radioscapholunate (LRSL), and the short radiolunate (SRL). The RSC is a critical structure that acts as a sling supporting the scaphoid waist, serving as a fulcrum for scaphoid flexion. The LRSL, historically considered a mechanical stabilizer, is now understood to be primarily a neurovascular conduit supplying the SL interosseous ligament. The SRL is a stout, unyielding ligament that acts as the primary tether preventing lunate dislocation. Intrinsic ligaments, particularly the SL and lunotriquetral (LT) interosseous ligaments, are critical for proximal row stability. The volar band of the LT ligament is its thickest and most biomechanically significant component, whereas the dorsal band of the SL ligament is its primary stabilizer.
Dorsal Ligamentous Anatomy
While thinner than the volar ligaments, the dorsal carpal ligaments are indispensable for preventing dorsal carpal subluxation and guiding the complex synchronous movements of the carpus. They are broadly categorized into the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments.
The morphological variations of these ligaments are vast, but their functional importance remains consistent. The DRC ligament originates from the dorsal rim of the distal radius and inserts primarily on the triquetrum, with variable slips to the lunate and scaphoid. It acts as a critical restraint against ulnar translation of the carpus.


The DIC ligament originates from the triquetrum and courses radially to insert on the scaphoid, trapezium, and trapezoid. Together, the DRC and DIC ligaments form a horizontal, V-shaped configuration across the dorsal carpus. This "dorsal V" stabilizes the proximal row, particularly during wrist flexion, preventing dorsal intercalated segment instability (DISI) posturing when the intrinsic SL ligament is compromised.



Understanding the comprehensive dorsal perspective is vital for performing ligament-sparing capsulotomies (e.g., the Berger flap), which utilize the intervals between the DRC and DIC ligaments to expose the radiocarpal and midcarpal joints without compromising postoperative stability or proprioception.
Vascular Anatomy and Circulation
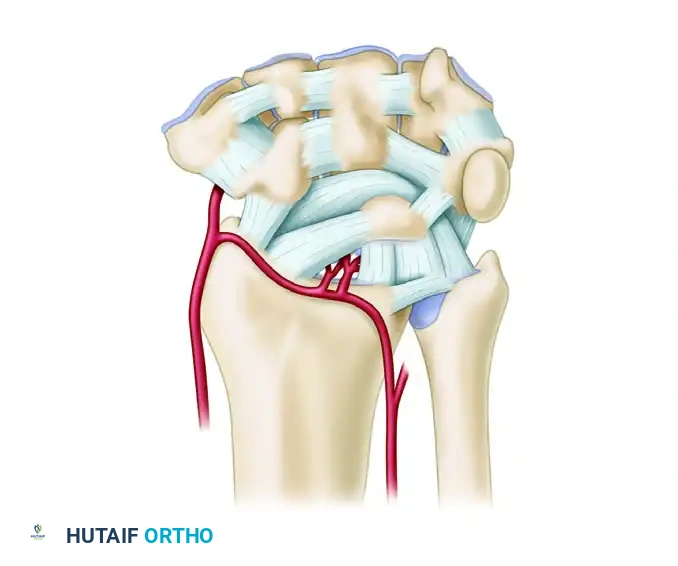
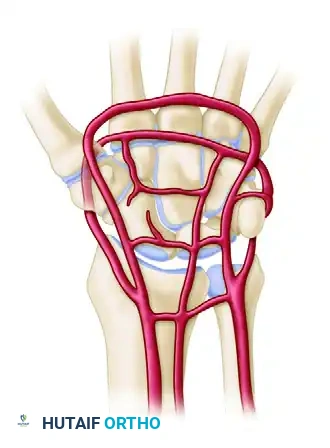
The extraosseous blood supply to the carpus is derived from the terminal branches of the radial, ulnar, and anterior interosseous arteries. These vessels form a highly redundant, anastomotic network comprising three dorsal and three palmar transverse arterial arches.
The dorsal arterial arches include the dorsal radiocarpal arch, the dorsal intercarpal arch, and the basal metacarpal arch. The dorsal intercarpal arch is the largest and most consistent, located between the proximal and distal carpal rows. It provides the dominant blood supply to the distal row and sends critical retrograde branches to the proximal poles of the scaphoid and lunate.
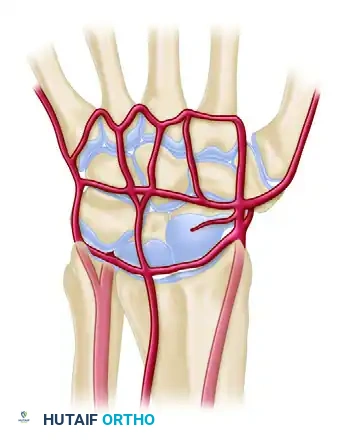
The palmar arterial arches consist of the palmar radiocarpal arch, the palmar intercarpal arch, and the deep palmar arch. While the deep palmar arch is robust and communicates directly with the dorsal basal metacarpal arch, the palmar intercarpal arch is highly variable and rarely contributes significant nutrient vessels to the intraosseous carpus. The palmar radiocarpal arch is vital for supplying the palmar surfaces of the lunate and triquetrum.
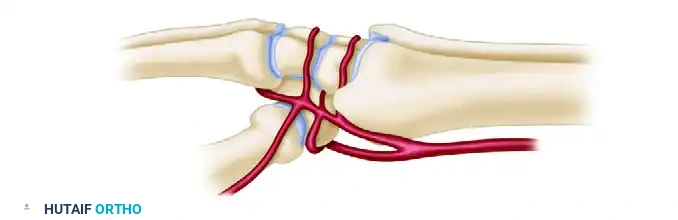
From a lateral perspective, the radial artery provides critical branches that supply the scaphoid tubercle and the trapezium. The vascularity of the scaphoid is particularly precarious. Gelberman’s landmark anatomical studies demonstrated that 70% to 80% of the scaphoid’s intraosseous blood supply enters via the dorsal ridge (from the dorsal carpal branch of the radial artery) and flows in a retrograde fashion to supply the proximal pole. The remaining 20% to 30% enters via the volar tubercle. Consequently, fractures occurring at the scaphoid waist or proximal pole disrupt this retrograde flow, placing the proximal fragment at an exceptionally high risk for avascular necrosis (AVN) and nonunion.
Biomechanics and Kinematics
The biomechanics of the wrist are governed by load transmission and complex kinematic theories. In a wrist with neutral ulnar variance, the radius absorbs approximately 80% of axial loads, while the ulna absorbs the remaining 20% via the TFCC. Alterations in ulnar variance drastically shift this load distribution. A positive ulnar variance of just +2.5mm increases ulnar load transmission to 42%, frequently resulting in ulnocarpal impaction syndrome and degenerative TFCC tearing. Conversely, negative ulnar variance increases radial loading and is strongly associated with Kienböck's disease (AVN of the lunate) due to increased shear forces on the lunate from the radius.
Carpal kinematics are best understood through the "Row Theory." During radioulnar deviation, the proximal row acts as a flexible intercalated segment. In radial deviation, the scaphoid must flex to avoid bony impingement on the radial styloid. Because the scaphoid is tightly bound to the lunate via the stout dorsal SL ligament, it forces the lunate and triquetrum into flexion as well. During ulnar deviation, the entire proximal row extends. If the SL ligament is ruptured, this synchronous movement is uncoupled. The scaphoid flexes independently, while the lunate and triquetrum (bound by the intact LT ligament) extend, resulting in the classic DISI (Dorsal Intercalated Segment Instability) deformity.
Exhaustive Indications and Contraindications
Surgical intervention in the wrist demands precise decision-making based on fracture morphology, ligamentous integrity, patient demands, and the presence of degenerative changes. The following table outlines the absolute and relative indications, as well as contraindications, for common wrist pathologies.
| Pathology / Procedure | Absolute Indications | Relative Indications | Absolute Contraindications |
|---|---|---|---|
| Scaphoid Proximal Pole Fracture | Displaced fracture >1mm; Any proximal pole fracture (due to high AVN risk). | Undisplaced waist fracture in a high-demand athlete seeking early return to play. | Active localized infection; Medically unstable patient. |
| Scaphoid Nonunion | Symptomatic nonunion with cystic changes; SNAC Stage I or II. | Asymptomatic nonunion in a young patient (to prevent future arthritis). | Advanced SNAC Stage III (requires salvage procedure, not fixation/grafting). |
| Acute SL Ligament Tear | Complete tear with static radiographic gap (Terry Thomas sign >3mm) and DISI deformity. | Dynamic instability (pain with normal static x-rays but positive arthroscopy). | Fixed, irreducible carpal deformity; Pre-existing SLAC arthritis. |
| Distal Radius Fracture (ORIF) | Volar tilt >20° dorsal; Intra-articular step-off >2mm; Radial shortening >3mm. | Osteoporotic bone precluding cast maintenance; Bilateral upper extremity injuries. | Non-ambulatory, low-demand elderly patient with minimal pain (relative/absolute depending on comorbidities). |
| TFCC Tear (Palmer 1B) | Acute peripheral tear with gross DRUJ instability. | Chronic ulnar-sided wrist pain failing >3 months of conservative management. | Central avascular tear (Palmer 1A) - requires debridement, not repair. |
| SLAC/SNAC Advanced Arthritis | Intractable pain with Stage III arthritis (capitolunate involvement). | Stage II arthritis failing conservative management (PRC or 4-corner fusion indicated). | Proximal Row Carpectomy (PRC) is contraindicated if the capitate head is arthritic. |
Surgical decision-making must also account for patient-specific factors such as smoking status, which significantly impairs microvascular perfusion and drastically increases the risk of nonunion in carpal procedures. In cases of advanced SLAC/SNAC where the radiolunate joint is spared (which is typical, as the spherical lunate fossa maintains congruity), a Proximal Row Carpectomy (PRC) or Scaphoid Excision with Four-Corner Fusion (4CF) are the primary salvage options. PRC requires a pristine capitate head, whereas 4CF can be performed even if midcarpal arthritis is present, provided the radiolunate joint is intact.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful wrist surgery. The complex three-dimensional anatomy of the carpus necessitates high-quality, multi-planar imaging. Standard zero-PA and true lateral radiographs are mandatory. A true lateral is confirmed when the palmar cortex of the pisiform lies precisely midway between the palmar cortices of the distal scaphoid pole and the capitate head. Gilula’s three carpal arcs must be assessed on the PA view to rule out subtle carpal disruptions.
For scaphoid fractures, specific scaphoid views (PA with the wrist in ulnar deviation and slight extension) elongate the scaphoid profile, projecting it away from the overlapping radius. Computed Tomography (CT) with 1mm fine cuts in the sagittal, coronal, and axial planes parallel to the long axis of the scaphoid is the gold standard for assessing fracture displacement, comminution, humpback deformity, and union status. Magnetic Resonance Imaging (MRI) without contrast is highly sensitive for detecting occult fractures, AVN of the proximal pole, and intrinsic ligament tears, although MR arthrography provides superior resolution for TFCC and SL/LT ligament pathology.
Templating software should be utilized to determine screw length for scaphoid fixation. The goal is to place the longest possible headless compression screw down the central axis of the scaphoid to maximize biomechanical stability and compression, without violating the proximal or distal articular surfaces.
Patient positioning is standardized for most wrist procedures. The patient is placed supine with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. For dorsal approaches, the forearm is fully pronated. For volar approaches, the forearm is supinated. The C-arm fluoroscopy unit should be positioned parallel to the hand table, entering from the distal end or the contralateral side, allowing the surgeon unimpeded access while providing orthogonal intraoperative imaging.
Step-by-Step Surgical Approach and Fixation Technique
The Universal Dorsal Approach to the Wrist
The dorsal approach provides expansive access to the radiocarpal and midcarpal joints, making it the workhorse approach for proximal row carpectomy, four-corner fusion, dorsal perilunate dislocation reduction, and retrograde scaphoid fixation.
- Incision and Superficial Dissection: A longitudinal incision is centered directly over Lister's tubercle, extending 3-4 cm proximal and distal to the radiocarpal joint. The subcutaneous tissue is bluntly dissected to protect the dorsal sensory branches of the radial nerve (radially) and the dorsal cutaneous branch of the ulnar nerve (ulnarly).
- Extensor Retinaculum Management: The extensor retinaculum is exposed. The third extensor compartment is incised longitudinally, and the Extensor Pollicis Longus (EPL) tendon is mobilized and transposed radially.
- Deep Dissection: The floor of the third compartment is incised. Subperiosteal elevation of the second compartment (ECRL/ECRB) radially and the fourth compartment (EDC/EIP) ulnarly exposes the dorsal wrist capsule.
- Capsulotomy: A ligament-sparing capsulotomy is paramount to prevent postoperative instability. The Berger dorsal capsular flap is created by making an incision parallel to the DRC ligament and a second incision parallel to the DIC ligament, creating a distally based, V-shaped flap. This preserves the critical dorsal mechanoreceptors and stabilizing ligaments.
- Procedure Execution: Once the carpus is exposed, the specific procedure (e.g., scaphoid excision, lunate reduction) is performed.
- Closure: The capsular flap is meticulously repaired with non-absorbable sutures. The EPL is left transposed in the subcutaneous tissue to prevent attrition rupture against dorsal hardware or bony irregularities.
The Volar Approach (FCR Bed)
The volar approach, utilizing the bed of the Flexor Carpi Radialis (FCR), is the standard for distal radius fracture fixation (volar locking plates), volar scaphoid fixation, and decompression of the carpal tunnel combined with wrist surgery.
- Incision: A longitudinal incision is made directly over the FCR tendon, incorporating a zig-zag (Bruner) incision across the wrist flexion creases to prevent scar contracture.
- Superficial Dissection: The superficial fascia is incised, and the FCR tendon sheath is opened. The FCR tendon is retracted ulnarly (or radially, depending on surgeon preference, though ulnar retraction protects the median nerve). The palmar cutaneous branch of the median nerve, lying ulnar to the FCR, must be strictly avoided.
- Deep Dissection: The floor of the FCR sheath is incised, exposing the deep space. The Flexor Pollicis Longus (FPL) tendon is identified and retracted ulnarly with the flexor digitorum tendons.
- Pronator Quadratus Elevation: The pronator quadratus (PQ) muscle is identified. An L-shaped incision is made along its radial and distal borders. The PQ is elevated subperiosteally from radial to ulnar, exposing the volar cortex of the distal radius.
- Capsulotomy (if required): If access to the radiocarpal joint is necessary (e.g., for volar scaphoid ORIF), a longitudinal or transverse volar capsulotomy is performed. Extreme care must be taken to preserve the stout RSC and SRL ligaments to prevent irogenic volar carpal instability.
- Fixation and Closure: Following fracture reduction and plate fixation, or scaphoid screw placement, the PQ is repaired over the hardware if possible to prevent flexor tendon irritation. The FCR sheath is left open, and the skin is closed in layers.
Complications, Incidence Rates, and Salvage Management
Wrist surgery is fraught with potential complications due to the dense concentration of neurovascular structures, the tenuous blood supply of the carpus, and the unforgiving biomechanical demands placed on the joint. Anticipation and early recognition of these complications are critical.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage & Management Strategy |
|---|---|---|---|
| Scaphoid Avascular Necrosis (AVN) | 15-30% (Proximal pole fractures) | Disruption of retrograde intraosseous blood supply entering the dorsal ridge. | Vascularized bone grafting (e.g., 1,2-ICSRA or medial femoral condyle free flap). |
| Complex Regional Pain Syndrome (CRPS) | 5-10% | Dysfunctional sympathetic nervous system response to trauma/surgery. | Early aggressive hand therapy, gabapentinoids, sympathetic nerve blocks, Vitamin C prophylaxis. |
| Tendon Rupture (EPL or Flexors) | 1-3% | Attrition over prominent dorsal hardware (EPL) or proud volar plates (FPL). | Hardware removal, tendon transfer (e.g., EIP to EPL), or tendon grafting. |
| Hardware Failure / Screw Cut-out | 2-5% | Poor bone quality, premature weight-bearing, eccentric screw placement. | Revision ORIF with larger diameter screw, bone grafting, or salvage arthrodesis. |
| Post-Traumatic Osteoarthritis (SLAC/SNAC) | Highly variable (Depends on initial injury) | Altered carpal kinematics leading to asymmetric joint loading and cartilage wear. | Proximal Row Carpectomy (PRC), Four-Corner Fusion, or Total Wrist Arthrodesis. |
| Iatrogenic Nerve Injury (SRN or PCBMN) | 1-4% | Direct laceration or aggressive retraction of the Superficial Radial Nerve or Palmar Cutaneous Branch of the Median Nerve. | Microsurgical repair, neuroma excision, and targeted muscle reinnervation (TMR). |
Salvage procedures for the wrist are generally motion-preserving (PRC, 4-corner fusion) or motion-eliminating (total wrist arthrodesis). PRC transforms the complex multi-articulated wrist into a simple hinge joint between the radius and the capitate. It requires less immobilization than a 4-corner fusion but relies on pristine articular cartilage on the capitate head and lunate fossa. Four-corner fusion (capitate, hamate, lunate, triquetrum) with scaphoid excision preserves the radiolunate articulation and is preferred in younger, heavier-demand patients or those with capitate arthrosis.
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following wrist surgery is as critical as the surgical execution itself. The balance between protecting the surgical repair and preventing debilitating stiffness requires a highly structured, phased approach, closely coordinated with a certified hand therapist (CHT).
Phase I: Immobilization and Edema Control (Weeks 0-2)
The primary goals of the immediate postoperative phase are to protect the surgical site, minimize edema, and prevent complex regional pain syndrome (CRPS).
* Immobilization: Depending on the procedure, the patient is placed in a bulky Jones dressing reinforced with a volar plaster splint, or a sugar-tong splint if DRUJ rotational control is required (e.g., TFCC repair).
* Edema Management: Strict, continuous elevation of the hand above the level of the heart is mandatory.
* Motion: Immediate, aggressive active range of motion (AROM) of all uninvolved joints is instituted. This includes full composite flexion and extension of the digits, thumb opposition, and elbow/shoulder ROM to prevent tendon adhesions and promote lymphatic drainage.
Phase II: Early Protected Motion (Weeks 2-6)
At the 10-14 day mark, sutures are removed. If rigid internal fixation was achieved (e.g., volar plating of a distal radius, headless screw fixation of a scaphoid), early protected motion can commence.
* Orthosis: The patient is transitioned to a custom-molded thermoplastic splint (e.g., a short arm Munster splint or a standard volar
