Disorders of the Posterior Tibial Tendon: Comprehensive Surgical Management
Key Takeaway
Posterior tibial tendon dysfunction (PTTD) is the primary cause of adult-acquired flatfoot deformity. Progressive failure of the posterior tibial tendon leads to medial longitudinal arch collapse, hindfoot valgus, and forefoot abduction. Management ranges from conservative bracing to complex surgical reconstruction, including tendon transfers, osteotomies, and arthrodesis, dictated by the flexibility of the deformity and the integrity of the articular surfaces.
Introduction to Posterior Tibial Tendon Disorders
Disorders of the posterior tibial tendon (PTT) represent a spectrum of pathology ranging from acute tenosynovitis to chronic, rigid adult-acquired flatfoot deformity (AAFD). As the primary dynamic stabilizer of the medial longitudinal arch, the posterior tibial tendon plays an indispensable role in normal foot biomechanics. Insufficiency of this tendon initiates a predictable, progressive kinematic collapse of the foot and ankle, ultimately leading to profound disability.
For the practicing orthopedic surgeon, mastering the nuances of PTTD requires a deep understanding of hindfoot biomechanics, a meticulous clinical examination, and a comprehensive surgical armamentarium that addresses both soft-tissue attenuation and bony malalignment.
Biomechanics and Pathoanatomy
The posterior tibial muscle originates from the posterior aspect of the tibia, fibula, and interosseous membrane. Its tendon courses posterior to the medial malleolus, acting as a primary plantarflexor and invertor of the foot.
During the normal gait cycle, the stance phase begins with the hindfoot in a neutral to slightly inverted position. Through midstance, the hindfoot everts into valgus to absorb shock. Crucially, at terminal stance (toe-off), the posterior tibial tendon fires to invert the hindfoot. This inversion locks the transverse tarsal joint (Chopart's joint), converting the midfoot into a rigid lever arm essential for efficient forward propulsion.
Clinical Pearl: In posterior tibial tendon insufficiency, the failure to invert the hindfoot at terminal stance prevents the transverse tarsal joint from locking. This subjects the midfoot ligaments to massive, repetitive strain, leading to secondary failure of the static stabilizers.
The Cascade of Failure
The collapse of the medial arch is rarely isolated to the tendon alone. As the PTT attenuates, increasing pressure and strain are transferred to the static medial restraints.
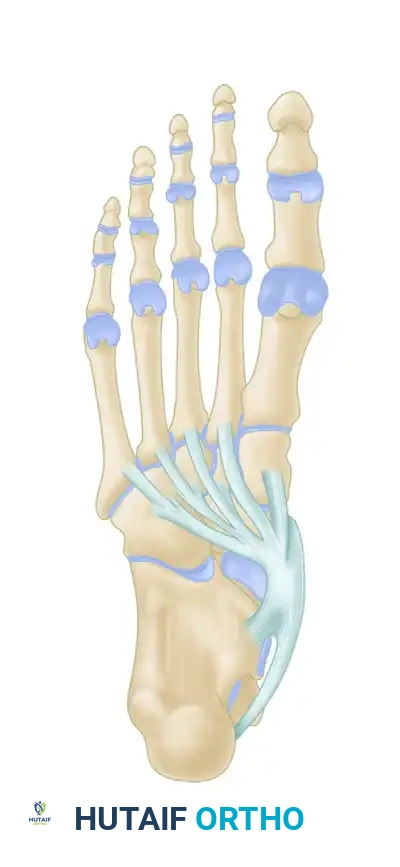
1. Spring Ligament Complex: The plantar calcaneonavicular (spring) ligament is the most commonly involved secondary restraint. Its attenuation allows the talar head to plantarflex and rotate medially.
2. Deltoid Ligament: In severe cases, the superficial deltoid ligament (specifically the tibionavicular portion) elongates, introducing significant medial ankle instability.
3. Plantar Fascia and Midfoot Ligaments: The naviculocuneiform and plantar metatarsal ligaments eventually fail, leading to fixed forefoot abduction and supination.

The talus slides distally, medially, and plantarward with the loss of the posterior tibial tendon and subsequent insufficiency of the plantar calcaneonavicular (spring) ligament.
Classification of Posterior Tibial Tendon Insufficiency
The classification system originally developed by Johnson and Strom (1989), and later modified by Myerson, remains the gold standard for guiding treatment and predicting outcomes.
Stage I
Characterized by tenosynovitis without deformity. Patients present with swelling, pain, and inflammation within the PTT sheath.
* Clinical Findings: Mild weakness may be present due to pain inhibition, but the patient can perform a single-leg toe raise. The hindfoot remains in normal alignment.
* Pathology: Synovial proliferation and peritendinous effusion; the tendon length is preserved.
Stage II
Characterized by tendon elongation and a flexible flatfoot deformity. The patient is unable to perform a single-leg toe raise.
* Stage IIa: Hindfoot valgus and medial arch collapse, but minimal forefoot abduction.
* Stage IIb: Significant forefoot abduction (uncovering of the talonavicular joint) is present in addition to hindfoot valgus.
* Clinical Findings: Attempted compensation by the anterior tibial muscle is common. The deformity is fully correctable passively.
Stage III
Characterized by a rigid, fixed flatfoot deformity.
* Clinical Findings: The hindfoot is fixed in valgus, and the forefoot is fixed in abduction. Degenerative arthritic changes are often apparent in the subtalar and talonavicular joints.
* Symptoms: Pain shifts from the medial aspect to the lateral aspect (sinus tarsi) due to subfibular impingement.
Stage IV
Described by Myerson et al., this stage involves the ankle joint.
* Clinical Findings: Valgus positioning and incongruency of the ankle joint secondary to deltoid ligament failure. Talar tilt is evident on weight-bearing AP ankle radiographs.
Clinical Evaluation
Patient History
Patients typically report an insidious onset of medial ankle pain, swelling, and a gradual flattening of the arch. They may describe their foot "rolling out" or rapid fatigue during ambulation. In advanced stages (Stage III/IV), the primary complaint often shifts to lateral hindfoot pain due to the lateral process of the talus impinging against the floor of the sinus tarsi or the fibula.
Physical Examination
A systematic examination is paramount. Observe the patient standing barefoot.

Patient with bilateral pes planus demonstrating the classic loss of the medial longitudinal arch.
Weight-bearing posterior view showing the three components of deformity: hindfoot valgus, forefoot abduction, and arch collapse. The Achilles tendon tightens in long-standing deformity, exacerbating heel valgus.
1. The "Too Many Toes" Sign: Viewed from behind, forefoot abduction allows the examiner to see more toes on the lateral side of the affected foot compared to the normal side.
2. Single-Leg Heel Rise Test: Ask the patient to stand on the affected leg and rise onto the toes. A normal foot will invert the calcaneus. A patient with Stage II or greater PTTD cannot perform this maneuver, or if they do, the calcaneus remains in valgus.
Surgical Warning: Some patients with supple deformities may "throw" the hindfoot into a locked position using the gastrocsoleus complex and external support. Careful observation is required to ensure true active inversion by the PTT.

In the sitting position, when asked to hold the foot in plantarflexion-inversion, the patient unconsciously recruits the anterior tibial tendon to substitute for the deficient posterior tibial tendon.
3. Assessment of Deformity Flexibility: Invert the heel to neutral. If the forefoot remains supinated (varus), a fixed forefoot supinatus is present, which must be addressed surgically.
4. The Silfverskiöld Test: Contracture of the gastrocsoleus complex frequently accompanies PTTD.


The Silfverskiöld test determines selective gastrocnemius tightness. Passive dorsiflexion is measured with the knee flexed (left) and extended (right). A significant reduction in dorsiflexion with the knee extended indicates an isolated gastrocnemius contracture, necessitating a gastrocnemius recession.



Patients with posterior tibial tendon insufficiency as a result of attritional loss of continuity. Note the marked midfoot abduction, hindfoot valgus, and the convexity of the medial side with concavity of the lateral side.
Radiographic and Imaging Evaluation
Weight-Bearing Radiographs
Standard evaluation requires standing AP, lateral, and mortise views of the foot and ankle.
- AP View: Assess the talonavicular coverage angle. Uncovering of the talar head indicates forefoot abduction. The talus-first metatarsal angle (normally 0 degrees) will be elevated.
- Lateral View: Assess the medial longitudinal arch.
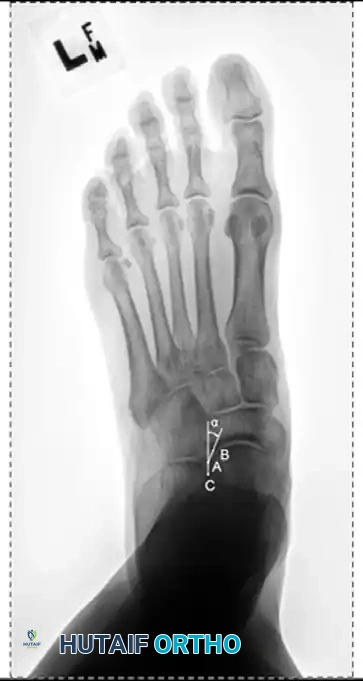
- Meary's Angle: The intersection of the longitudinal axis of the talus and the first metatarsal. An angle >4 degrees indicates arch collapse.
- Calcaneal Pitch: Decreased in flatfoot deformity.
- Lateral Tibial-Calcaneal Angle: Arangio et al. demonstrated this angle is a sensitive method for quantifying Achilles tendon contracture in adult-acquired flatfoot.
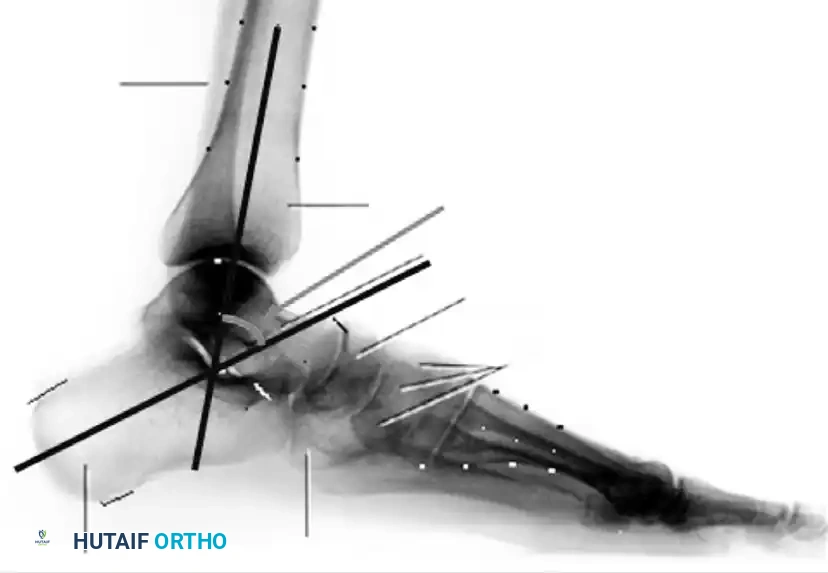
Measurement of the standing lateral tibial-calcaneal angle, utilized to quantify Achilles contracture.


Preoperative and postoperative radiographic comparisons demonstrating correction of Meary's angle and talonavicular coverage following structural reconstruction.
Magnetic Resonance Imaging (MRI)
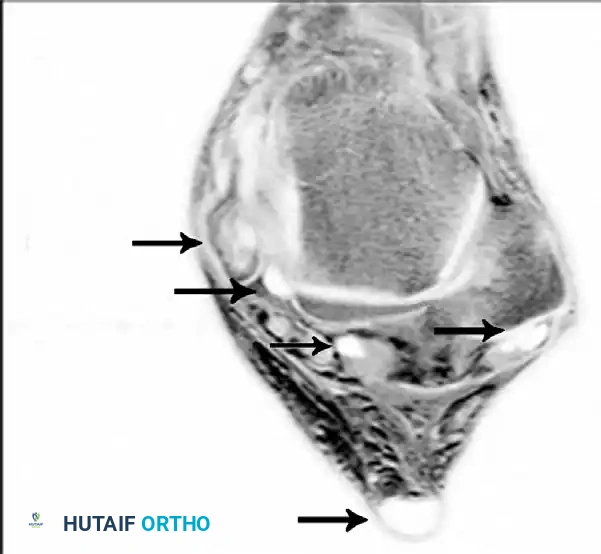
MRI is highly sensitive for evaluating the integrity of the PTT, spring ligament, and deltoid ligament. T2-weighted and fat-suppressed images excel at demonstrating peritendinous effusions, tendinosis, and interstitial tearing. DeOrio et al. described the "posterior tibial edema sign," where subcutaneous pitting edema along the tendon correlates with MRI evidence of disease in 88% of patients.


Axial MRI slices demonstrating severe tendinosis, fluid within the tendon sheath, and attenuation of the spring ligament complex.
Surgical Management: Step-by-Step
Surgical intervention is dictated strictly by the stage of the disease, the flexibility of the deformity, and the presence of arthritic changes.
Stage I: Tenosynovectomy and Debridement
When conservative measures (immobilization, NSAIDs, orthotics) fail after 3 to 6 months, surgical debridement is indicated.

Patient with mild unilateral pes planus and recalcitrant tenosynovitis. Inflamed synovium is obvious along the tendon, causing loss of excursion. Radiographs are typically normal in this stage.
Surgical Technique:
1. Incision: A longitudinal incision is made along the course of the PTT, from the retromalleolar groove extending distally to the navicular tuberosity.
2. Sheath Release: The flexor retinaculum is incised. Care is taken to preserve a small distal pulley to prevent tendon subluxation.
3. Debridement: Hypertrophic synovium is meticulously excised. The tendon is inspected for longitudinal splits. If tears involve less than 50% of the tendon substance, they are tubularized with running non-absorbable suture.
4. Postoperative Care: Weight-bearing in a CAM boot for 3-4 weeks, followed by aggressive physical therapy.
Stage II: Joint-Sparing Reconstruction
Stage II disease requires a combination of soft-tissue reconstruction and bony osteotomies to restore the biomechanical axis. An isolated tendon transfer will universally fail due to the uncorrected mechanical disadvantage.
1. Flexor Digitorum Longus (FDL) Transfer
The FDL is the ideal transfer due to its proximity, in-phase firing, and expendable nature.
* Harvest: The FDL is identified at the Master Knot of Henry (where it crosses dorsal to the FHL). It is transected as distally as possible.
* Routing: A drill hole is created dorsal-to-plantar through the navicular. The FDL is passed through the tunnel and tensioned with the foot in maximal plantarflexion and inversion. Fixation is achieved with a biotenodesis screw or button.
2. Medial Displacement Calcaneal Osteotomy (MDCO)
Addresses the hindfoot valgus by shifting the Achilles tendon insertion medially, converting it from an evertor to an invertor.
* Approach: An oblique lateral incision is made posterior to the sural nerve and peroneal tendons.
* Osteotomy: An oscillating saw is used to create a transverse osteotomy in line with the incision.
* Displacement: The posterior tuberosity is translated medially by 10 mm.
* Fixation: Secured with one or two large-fragment (6.5mm or 7.3mm) cannulated screws placed from the posterior heel into the anterior calcaneus.


Intraoperative views and fluoroscopy demonstrating the medial displacement calcaneal osteotomy (MDCO) and subsequent screw fixation.
3. Lateral Column Lengthening (Evans Osteotomy)
Indicated specifically for Stage IIb disease to correct severe forefoot abduction.
* Osteotomy: A vertical osteotomy is made in the anterior calcaneus, 1.5 cm proximal to the calcaneocuboid joint.
* Grafting: The osteotomy is distracted, and a tricortical iliac crest autograft or allograft wedge (typically 8-10 mm) is inserted to lengthen the lateral column, swinging the forefoot out of abduction.
* Fixation: A cervical plate or staple is used to secure the graft.
4. Spring Ligament Repair
The attenuated spring ligament is imbricated and repaired using suture anchors placed into the sustentaculum tali and navicular, reinforcing the medial arch.
5. Gastrocnemius Recession
If the Silfverskiöld test is positive, a Strayer or Baumann procedure is performed to release the gastrocnemius aponeurosis, resolving the equinus contracture that drives midfoot collapse.



Clinical progression of a Stage II reconstruction: Preoperative deformity, intraoperative correction via osteotomies and tendon transfer, and final postoperative alignment.
Stage III: Joint-Sacrificing Arthrodesis
When the deformity becomes rigid or arthritic changes are present in the hindfoot, joint-sparing procedures are contraindicated. The goal is to create a plantigrade, stable, and pain-free foot through arthrodesis.
Triple Arthrodesis
Involves fusion of the subtalar, talonavicular, and calcaneocuboid joints.
* Preparation: Cartilage is meticulously denuded down to bleeding subchondral bone using curettes and osteotomes.
* Positioning (CRITICAL): The hindfoot must be fused in 5 degrees of valgus. Fusing the hindfoot in varus locks the transverse tarsal joint, leading to rigid lateral border overload and severe pain. The forefoot is rotated to neutral.
* Fixation:
* Subtalar: Large cannulated screws (7.3mm) from the calcaneal tuberosity into the talar dome.
* Talonavicular: Two 4.5mm screws or a specialized compression plate.
* Calcaneocuboid: Staples or 4.5mm screws.


*Radiographic examples of a solid triple arthrodesis, demonstrating restoration of Meary's angle and solid trabecular bridging across the subt
Associated Surgical & Radiographic Imaging


You Might Also Like