Comprehensive Introduction and Patho-Epidemiology
Radial longitudinal deficiency (RLD), historically and colloquially referred to as radial clubhand, represents a profoundly complex and highly variable spectrum of congenital upper extremity anomalies. It is characterized by the hypoplasia or complete aplasia of the radius, the radial-sided carpal bones (predominantly the scaphoid and trapezium), and the associated musculotendinous and neurovascular structures. Occurring with an estimated incidence of 1 in 30,000 to 1 in 100,000 live births, RLD is bilateral in approximately 50% to 60% of cases. The condition stems from a disruption of the apical ectodermal ridge (AER) and the zone of polarizing activity (ZPA) during the critical fourth to fifth weeks of embryonic development. Specifically, aberrations in the Sonic hedgehog (Shh) signaling pathway and fibroblast growth factor (FGF) expression have been heavily implicated in the failure of radial-sided limb bud differentiation.
The clinical presentation of RLD is striking and immediately recognizable at birth. The affected extremity exhibits a shortened forearm with a severe radial and volar deviation of the hand, often resting at a rigid 90-degree angle to the forearm. This structural deficit eliminates the critical skeletal support for the radial aspect of the carpus, leading to a severe biomechanical imbalance that worsens as the child grows. The ulna, which serves as the sole remaining skeletal pillar of the forearm, is typically thickened, shortened (reaching only 60% of its normal anticipated length at maturity), and frequently develops a compensatory ulnar-convex bow. The surrounding soft tissues—particularly the radial collateral ligament, radiocarpal capsule, and radial-sided neurovascular structures—become severely contracted, acting as an unyielding tether that exacerbates the deformity.
Crucially, RLD is rarely an isolated orthopedic anomaly; it is a sentinel clinical sign that mandates an exhaustive systemic evaluation. Up to 70% of patients with RLD present with associated syndromic conditions or systemic anomalies that can be life-threatening if unrecognized. The most critical associations include VACTERL association (Vertebral, Anal, Cardiac, Tracheoesophageal, Renal, and Limb anomalies), Holt-Oram syndrome (cardiac septal defects), TAR syndrome (Thrombocytopenia-Absent Radius, notably where the thumb is characteristically present), and Fanconi anemia (a catastrophic aplastic anemia and chromosomal instability syndrome). Consequently, the orthopedic surgeon must defer any surgical intervention until a comprehensive pediatric, genetic, hematologic, and cardiologic workup has been completed and the patient is deemed medically optimized.
The primary objective of orthopedic intervention in RLD is to reconstruct a functional and cosmetically acceptable upper extremity that allows the child to perform activities of daily living independently. Bora et al. established that successful management of this deformity requires a comprehensive, staged approach. Treatment must begin immediately after birth with serial corrective casting and passive stretching to elongate the contracted radial soft tissues. Once the patient reaches 6 to 12 months of age, surgical centralization of the carpus over the distal ulna is indicated. To maintain this correction and counteract the persistent radial deforming forces, a second-stage tendon transfer is performed 6 to 12 months later. This two-stage paradigm remains a cornerstone of pediatric hand surgery.
Detailed Surgical Anatomy and Biomechanics
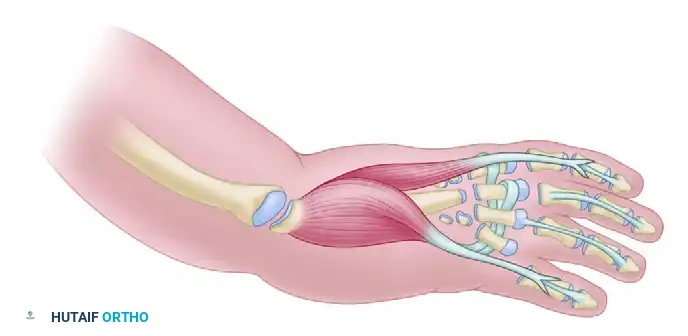
A profound understanding of the aberrant anatomy in RLD is the absolute prerequisite for safe and effective surgical intervention. The pathoanatomy of RLD extends far beyond the mere absence of the radius; it involves a global hypoplasia and disorganization of the entire radial-sided neurovascular and musculotendinous architecture. Skeletally, the deformity is classified by the Bayne and Klug system: Type I (deficient distal radial epiphysis), Type II (hypoplastic radius), Type III (partial aplasia, typically absent distal radius), and Type IV (complete aplasia of the radius). Type IV is the most common and presents the greatest surgical challenge. In these severe cases, the scaphoid and trapezium are universally absent, and the thumb is typically aplastic or severely hypoplastic.
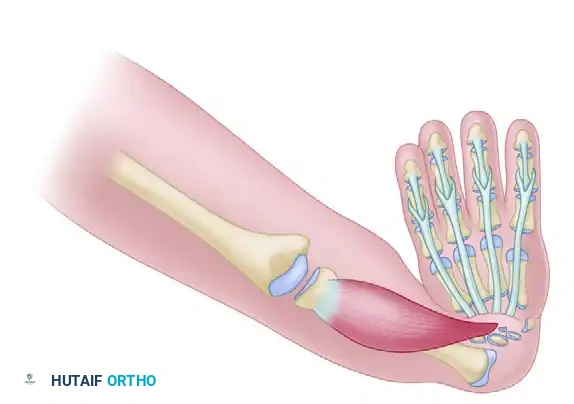
The musculotendinous anatomy in RLD is highly anomalous and unpredictable. The extrinsic flexor and extensor tendons, lacking their normal osseous fulcrum, exert an unopposed radial and volar deforming force. The brachioradialis, extensor carpi radialis longus (ECRL), and extensor carpi radialis brevis (ECRB) are frequently fused into a single fibrotic mass or blend aberrantly with the flexor carpi radialis (FCR). The flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons to the radial digits are often hypoplastic or absent. Conversely, the ulnar-sided musculature, including the extensor carpi ulnaris (ECU) and flexor carpi ulnaris (FCU), is typically present but mechanically disadvantaged due to the severe radial deviation of the carpus. Over time, this results in a progressive, rigid perpendicular relationship between the hand and the forearm.
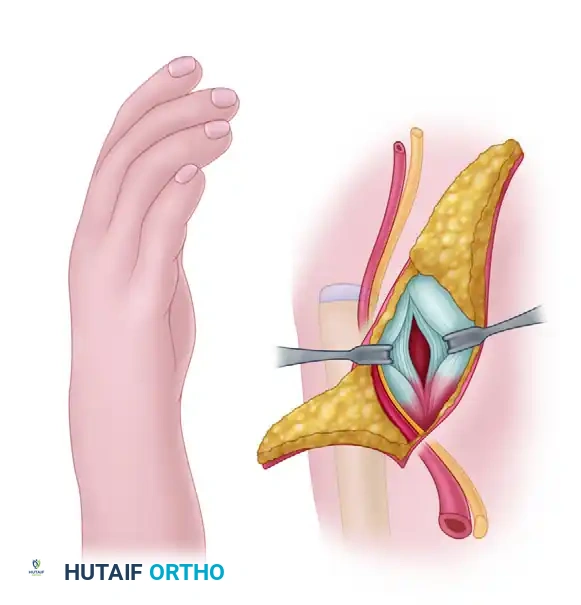
The neurovascular aberrations in RLD pose the most significant intraoperative risk. The radial artery is almost universally absent; arterial perfusion to the hand is entirely dependent on the ulnar artery and a dominant anterior interosseous artery. Therefore, any surgical maneuver that compromises the ulnar or interosseous blood supply can result in catastrophic ischemia of the hand. The radial nerve typically terminates at the level of the elbow, failing to provide sensory innervation to the dorsal-radial aspect of the hand.
Clinical Pearl: In severe RLD, the median nerve is profoundly anomalous. To compensate for the absent radial nerve, the median nerve frequently bifurcates proximally and lies superficially along the radial border of the forearm, directly beneath the fascia, acting as a tethering cord in the concavity of the deformity. Extreme caution must be exercised during the radial approach to avoid iatrogenic transection of this superficially displaced nerve, which provides critical motor and sensory function to the hand.
Biomechanically, the absence of the radius destroys the fundamental radiocarpal fulcrum. In a normal wrist, the radius supports 80% of the axial load transmitted from the carpus. In RLD, the carpus slides radially and volarly off the distal ulna, effectively eliminating the mechanical advantage of the extrinsic digital flexors and extensors. The hand becomes a flail appendage, severely limiting grip strength and digital dexterity. Centralization aims to restore this fulcrum by surgically seating the carpus directly over the distal ulna, thereby converting the ulna into a definitive, central load-bearing pillar. This realignment restores resting tension to the digital tendons, significantly improving the biomechanical efficiency of the fingers.
Exhaustive Indications and Contraindications
The decision to proceed with surgical centralization and subsequent tendon transfers is highly nuanced and must be individualized to the patient's specific pathoanatomy, functional status, and systemic health. The primary goal of centralization is to reposition the carpus over the distal end of the ulna, thereby creating a stable mechanical fulcrum that improves the functional length of the extremity, enhances digital flexor mechanics, and provides a cosmetically acceptable alignment.
Surgical intervention is generally reserved for patients with Bayne and Klug Type III and Type IV deficiencies, where the lack of radial support leads to a progressive and debilitating deformity. The timing of surgery is critical; it is typically performed between 6 and 12 months of age. At this stage, the anatomical structures are large enough to handle surgically, yet the soft tissues remain pliable enough to allow for correction without placing excessive tension on the delicate neurovascular bundles. Delaying surgery beyond 18 to 24 months significantly increases the risk of irreversible soft tissue contractures and recurrent deformity.
However, centralization is not universally indicated, and in certain clinical scenarios, it can be profoundly detrimental to the patient's function. The most critical prerequisite for centralization is adequate elbow flexion. In patients with severe RLD, the elbow is frequently stiff in extension. If the elbow lacks flexion, the radial deviation of the wrist is often the only mechanism allowing the child to bring the hand to the mouth for feeding and facial hygiene. Straightening the wrist in such patients will severely compromise their independence, converting a functional, albeit deformed, limb into a cosmetically straight but functionally useless appendage.
| Clinical Parameter | Indications for Centralization | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Deformity Severity | Bayne Type III and IV (Severe radial deviation) | Bayne Type I and mild Type II (Adequate radial support) | Moderate Type II with acceptable function |
| Elbow Function | Active and passive elbow flexion > 90 degrees | Severe elbow extension contracture (Stiff elbow) | Mild elbow stiffness requiring extensive therapy |
| Conservative Care | Failure of serial casting to maintain alignment | N/A | Non-compliant family/caregivers |
| Systemic Health | Medically cleared, optimized syndromic conditions | Untreated Fanconi anemia, severe cardiac instability | Poor anesthetic candidate, active infections |
| Patient Age | 6 to 12 months (Optimal soft tissue compliance) | Older adults with rigid, untreated, fixed deformities | Children > 3 years with severe, unyielding contractures |
In older patients presenting with neglected, rigid deformities, the soft tissues are often so severely contracted that acute centralization would cause profound stretching of the ulnar artery and median nerve, leading to ischemia and neuropathy. In these salvage scenarios, preliminary distraction osteogenesis (using an external fixator such as an Ilizarov or Taylor Spatial Frame) is mandated to gradually elongate the soft tissues prior to any open skeletal realignment.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of a successful centralization procedure. The planning phase begins months before the actual surgery, focusing heavily on non-operative soft tissue conditioning. Immediately following birth and medical clearance, the infant must undergo a rigorous protocol of serial corrective casting and passive stretching. The goal is to elongate the contracted radial-sided structures (the radial anlage, radial collateral ligament, and skin) and passively stretch the hand over the distal ulna. A well-executed casting protocol significantly reduces the soft tissue tension encountered during the open surgical release, thereby minimizing the risk of neurovascular compromise and reducing the complexity of the operation.
Radiographic templating is essential, though challenging in the infant due to the largely cartilaginous nature of the carpus. Standard anteroposterior and lateral radiographs of the forearm and hand are obtained to assess the severity of the ulnar bow, the presence of any rudimentary radial segments, and the relationship of the carpus to the distal ulna. If the ulnar bow exceeds 30 degrees, it may mechanically impede the centralization process or exacerbate postoperative recurrence. In such cases, a concurrent closing-wedge ulnar osteotomy may need to be templated and planned. Advanced imaging, such as MRI or ultrasound, is occasionally utilized in complex syndromic cases to map the anomalous musculotendinous anatomy and precisely locate the superficially displaced median nerve prior to incision.

On the day of surgery, the patient is placed supine on the operating table with the affected upper extremity extended onto a radiolucent hand table. General anesthesia is induced, and prophylactic intravenous antibiotics are administered. A pediatric pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is critical for identifying the delicate, anomalous neurovascular structures. The surgeon must utilize loupe magnification (typically 2.5x to 3.5x) to safely navigate the distorted anatomy.
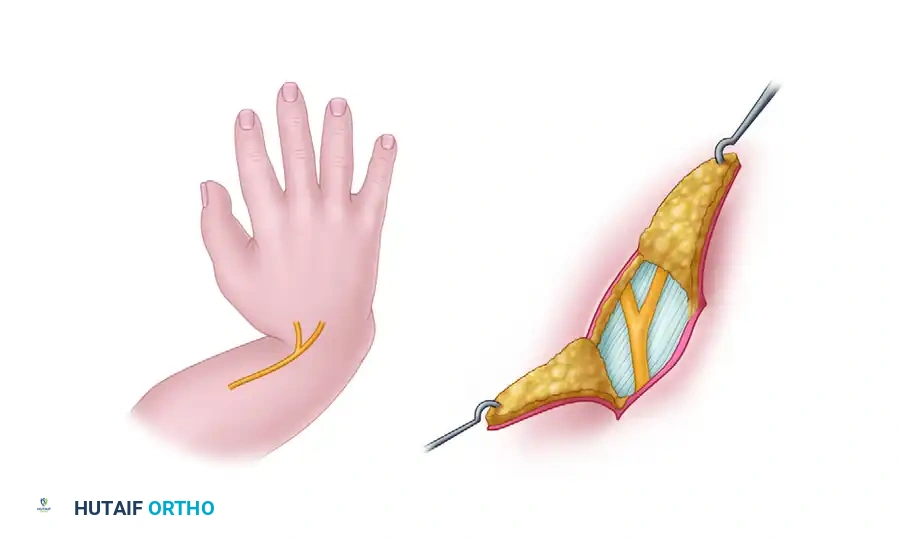
The surgical incision is carefully designed to address the soft tissue discrepancy inherent in RLD. The radial side of the wrist is severely deficient in skin, while the ulnar side often has redundant folds. A radial S-shaped, Z-plasty, or bilobed flap incision is marked over the radial aspect of the wrist. This specialized incision allows for extensive exposure of the contracted radial structures while providing a crucial lengthening effect during closure, accommodating the newly corrected, centralized posture without placing undue tension on the radial skin flaps.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of RLD via the Bora et al. technique is a highly orchestrated, two-stage process. Stage I focuses on skeletal realignment and soft tissue release, while Stage II, performed months later, provides dynamic musculotendinous rebalancing.
STAGE I: Surgical Centralization of the Hand
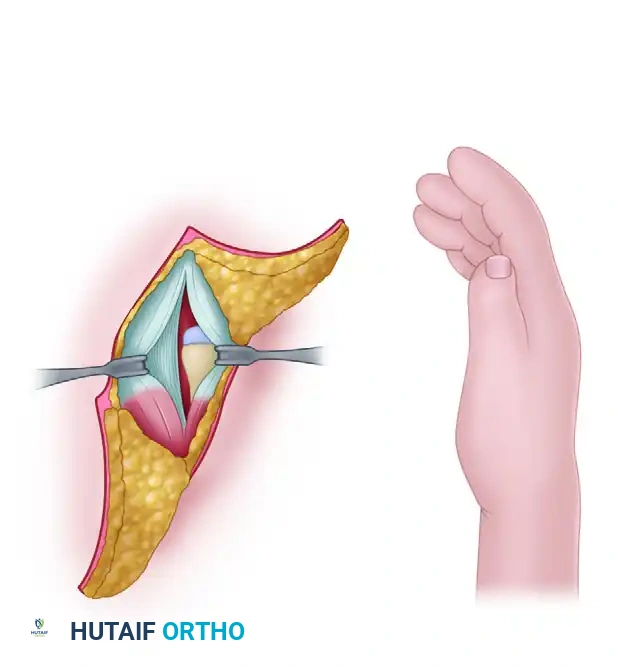
1. Soft Tissue Release and Exposure
Following exsanguination and tourniquet inflation, the meticulously planned radial incision is made. The skin flaps are elevated with extreme care, utilizing blunt dissection to avoid injuring the superficial veins. The immediate priority is the identification and protection of the superficial radial nerve (if present), the dorsal sensory branch of the ulnar nerve, and the superficially displaced median nerve. As previously noted, the median nerve frequently lies directly beneath the radial fascia; it must be isolated, mobilized, and gently retracted with a vessel loop.

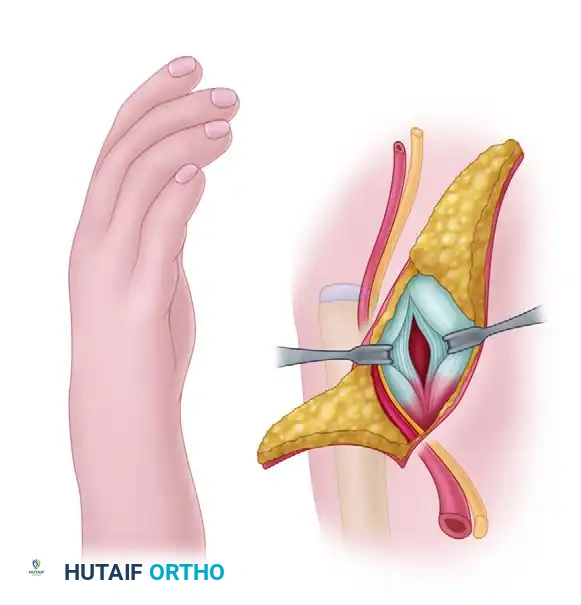
Once the neurovascular structures are secured, the surgeon identifies the thickened, fibrotic bands representing the anlage of the radius. This anlage, along with the contracted radiocarpal ligaments, volar capsule, and the fascial expansions of the brachioradialis and radial wrist extensors, must be aggressively released. A thorough, systematic release of all radial-sided tethering structures is mandatory to mobilize the carpus sufficiently so that it can be passively reduced over the distal ulna without tension.
2. Carpal Preparation and Slot Creation
To prevent the distal ulna from sliding radially or volarly off the carpus postoperatively, a central slot must be created within the carpal mass to securely seat the ulnar epiphysis. The central carpal bones—which are largely cartilaginous in the infant—are isolated.
Using a scalpel (typically a #15 blade), the surgeon carefully excises the lunate and the capitate. This excision creates a deep, rectangular notch or "slot" in the proximal carpal row. The dimensions of this slot must be perfectly tailored to receive the distal ulnar epiphysis. If the slot is too tight, it will crush the ulnar physis; if it is too loose, the centralization will be unstable.
3. Ulnar Preparation and Transposition
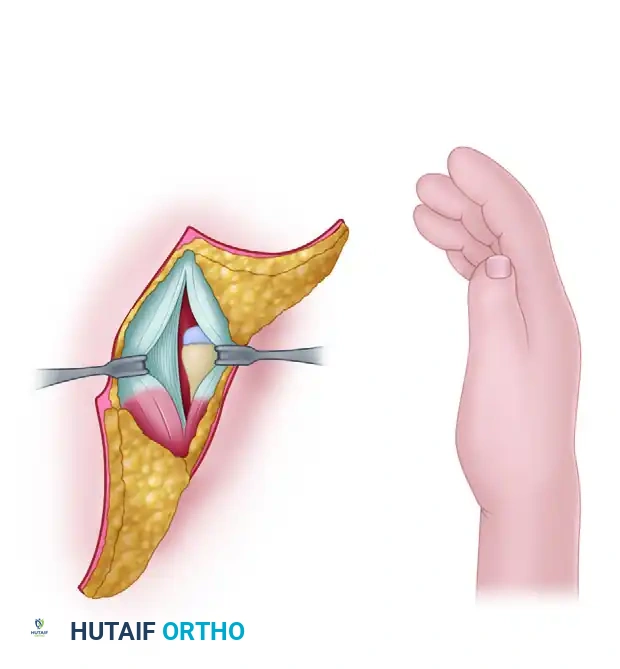
Attention is then turned to the distal ulna. If the primary radial incision does not provide adequate exposure, a separate longitudinal incision is made over the distal ulnar epiphysis. The distal ulna is freed from its surrounding soft tissue attachments. Meticulous care must be taken to preserve the extensor carpi ulnaris (ECU) and extensor digiti minimi (EDM) tendons, as these will be crucial for postoperative ulnar stability and future tendon transfers.
Surgical Warning: Extreme care must be taken not to strip the periosteum or damage the distal ulnar physis during preparation and seating. Physeal arrest of the distal ulna is a devastating complication that will lead to severe forearm shortening, rendering the limb functionally inferior and predisposing the patient to recurrent deformity.
The distal end of the ulna is then transposed radially through the plane between the flexor and extensor tendons, aligning it with the newly created carpal slot.
4. Skeletal Fixation
The distal ulnar epiphysis is seated deeply into the surgically created carpal slot (the space previously occupied by the lunate and capitate). The surgeon must ensure that the longitudinal axis of the ulna is directly aligned with the base of the long finger (third) metacarpal.
A smooth, stout Kirschner wire (typically 0.045 or 0.062 inch, depending on the patient's size and bone density) is selected. The K-wire is driven longitudinally through the carpus and into the intramedullary canal of the third metacarpal.
Once the wire is firmly secured within the metacarpal, the hand is held in a centralized, neutral position, and the K-wire is driven retrograde across the carpal slot and down the intramedullary canal of the ulnar shaft. This transfixes the hand and wrist in a perfectly centralized alignment.
Intraoperative fluoroscopy is utilized in both anteroposterior and lateral planes to confirm that the ulna is aligned with the long axis of the third metacarpal and that the K-wire is centrally placed within both medullary canals. The dorsal radiocarpal ligament and redundant dorsal capsule are then sutured tightly over the neck of the ulna using non-absorbable sutures to reinforce the stabilization. The tourniquet is deflated, meticulous hemostasis is achieved, and the skin is closed.
STAGE II: Tendon Transfers for Dynamic Rebalancing
Despite a successful skeletal centralization, the inherent soft tissue imbalance remains. The powerful radial flexors and extensors will inevitably pull the hand back into radial deviation if a dynamic counterforce is not established. Bora et al. advocated for tendon transfers 6 to 12 months following the initial centralization to provide an active ulnar-tethering force.
Before attempting to transfer the flexor digitorum superficialis (FDS) tendons, their function must be rigorously tested clinically, as they are frequently hypoplastic or absent in RLD. Only functioning FDS tendons (typically from the long and ring fingers) should be selected.

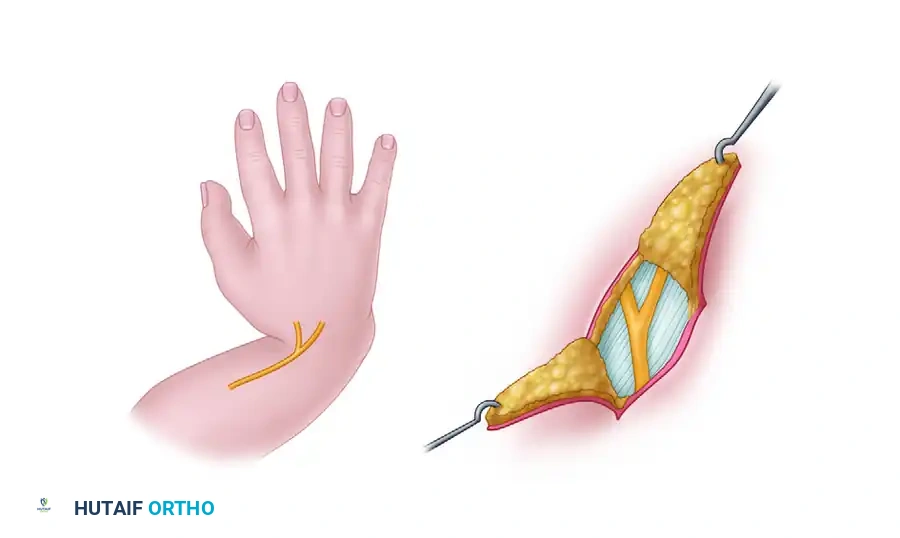
Under general anesthesia, a midlateral incision is made on the ulnar side of the long finger at the level of the PIP joint. The FDS tendon slips are identified, divided at their insertion on the middle phalanx, and withdrawn into the proximal forearm through a separate volar incision. This process is repeated for the ring finger FDS if dual transfers are planned.

The harvested FDS tendons are routed subcutaneously around the ulnar border of the forearm to the dorsal aspect of the wrist. The tendons are typically woven into the extensor carpi ulnaris (ECU) tendon using a Pulvertaft weave or anchored directly to the dorsal ulnar aspect of the carpus. The tension of the transfer is set with the wrist in neutral to slight ulnar deviation, and sutured securely using non-absorbable braided suture (e.g., 3-0 or 4-0 Ethibond). By rerouting a volar-radial force (FDS) to a dorsal-ulnar insertion, the surgeon eliminates a deforming force while simultaneously creating a corrective, stabilizing checkrein.
Complications, Incidence Rates, and Salvage Management
The surgical reconstruction of radial clubhand is fraught with potential complications, largely due to the severe inherent tissue deficiencies and the relentless biomechanical forces acting on the wrist. Surgeons undertaking these procedures must be intimately familiar with the long-term sequelae and possess the technical armamentarium to manage them.
Recurrent radial deviation is by far the most ubiquitous long-term complication, with incidence rates reported between 50% and 70% in long-term follow-up studies. This recurrence is driven by the relentless, unopposed pull of the radial musculature, inadequate initial soft tissue release, failure or stretching of the tendon transfer, and the natural growth of the child. Continuous, disciplined night splinting until skeletal maturity is mandatory to mitigate this risk. When recurrence is severe and functionally limiting, revision surgery is required.
Physeal arrest of the distal ulna is a catastrophic complication. The distal ulnar physis is responsible for 80% of the longitudinal growth of the ulna. Damage to this delicate structure during slot creation, aggressive periosteal stripping, or repeated K-wire passes will halt longitudinal growth. Given that the ulna is already the sole bone of the forearm in these patients and is inherently shortened, any further iatrogenic loss of length is functionally devastating.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Recurrent Radial Deviation | 50% - 70% | Aggressive initial release, Stage II tendon transfers, strict night splinting to maturity. | Revision centralization, Radialization (Buck-Gramcko), or Wrist Arthrodesis in adults. |
| Distal Ulnar Physeal Arrest | 10% - 20% | Avoid crushing the physis in the carpal slot; use smooth, centrally placed K-wires; limit K-wire passes. | Ulnar lengthening via distraction osteogenesis (Ilizarov) if severe shortening occurs. |
| Digital Stiffness | 30% - 40% | Early mobilization of the MCP and IP joints while the wrist remains pinned. | Aggressive occupational therapy, tenolysis in severe, refractory cases. |
| Neurovascular Injury | < 5% | Meticulous dissection, loupe magnification, awareness of superficial median nerve anomaly. | Immediate microsurgical repair if transected; observation if neuropraxia. |
| Pin Track Infection | 10% - 15% | Meticulous pin care, burying K-wires beneath the skin when possible. | Oral antibiotics; early pin removal if deep infection or osteomyelitis is suspected. |
Salvage procedures for failed centralizations are complex. The Buck-Gramcko "Radialization" procedure is a notable alternative or salvage option, wherein the carpus is transposed completely to the ulnar side of the ulna (rather than centralizing it), altering the mechanical lever arms to favor ulnar deviation. In older patients nearing skeletal maturity with painful, rigid recurrences, a definitive wrist arthrodesis is often the most reliable method to provide a stable, functional extremity.
Phased Post-Operative Rehabilitation Protocols
The success of the centralization and tendon transfer procedures is inextricably linked to a rigorous, prolonged, and family-compliant postoperative rehabilitation protocol. The rehabilitation is divided into distinct phases, requiring close collaboration between the orthopedic surgeon, specialized pediatric hand therapists, and the patient's caregivers.
Phase I: Acute Immobilization (Weeks 0 to 6-8)
Immediately following Stage I centralization, the patient is placed in a well-padded, long-arm cast. For unilateral deformities, the elbow is positioned at 90 degrees of flexion with the wrist and hand held in a neutral, centralized position. In bilateral cases, positioning is nuanced to facilitate feeding and interaction: both elbows are at 90 degrees, but one forearm is placed in 45 degrees of pronation and the other in 45 degrees of supination. The transfixing intramedullary K-wire and the cast are typically maintained for 6 to 8 weeks to allow for robust capsular healing and fibrous stabilization of the carpus over the ulna. During this phase, caregivers are instructed to encourage active movement of the fingers to prevent extensor and flexor tendon adhesions.
Phase II: Splinting and Mobilization (Weeks 8 to Pre-Stage II)
At the 6-to-8-week mark, the cast is bi-valved, and the K-wire is removed in the clinic. A custom-molded thermoplastic resting splint is immediately fabricated by the occupational therapist. This splint holds the wrist in neutral to slight ulnar deviation. Initially, the splint is worn full-time, removed only for hygiene and structured therapy sessions. Therapy focuses on active and passive range of motion of the digits, wrist, and elbow. As dynamic stability improves, daytime splint wear is gradually weaned, allowing the child to incorporate the centralized hand into bimanual
