Cementless Fixation: Mastering Techniques & Overcoming Pitfalls
Introduction & Epidemiology
Cementless fixation in arthroplasty, relying on the biological process of osseointegration, represents a paradigm shift from traditional cemented constructs. Its evolution stems from the concept that direct bone apposition onto a porous-coated implant surface provides a durable, long-term bond, particularly advantageous in patients with good bone quality and anticipated longer implant survival. The initial mechanical stability, achieved through a "press-fit" or "scratch-fit" design, is paramount to prevent micromotion exceeding 150 µm, which can inhibit bone ingrowth and lead to fibrous tissue formation at the implant-bone interface.
The prevalence of cementless components, particularly in total hip arthroplasty (THA) and total knee arthroplasty (TKA), has steadily increased. In THA, cementless fixation is now the dominant choice in many regions, especially for younger and more active patients. Its adoption in TKA has been more gradual but is gaining traction, driven by advancements in implant design, coating technologies, and surgical techniques that ensure robust primary stability. This approach aims to reduce potential complications associated with cement (e.g., thermal necrosis, cement mantle fracturing, monomer systemic effects) and facilitate easier revision by minimizing bone loss compared to removing a well-fixed cemented component. Understanding the intricate balance between biomechanical principles, meticulous surgical execution, and patient-specific factors is crucial for maximizing the success of cementless arthroplasty.
Surgical Anatomy & Biomechanics
Successful cementless fixation is predicated on achieving immediate rigid mechanical interlock between the implant and host bone, followed by biological osseointegration. This requires an in-depth understanding of regional skeletal anatomy and the biomechanical principles governing the bone-implant interface.
Bone Stock and Quality
The quality and quantity of host bone are critical. Cortical bone offers immediate rigid support, while cancellous bone provides a scaffold for subsequent osseointegration. Bone mineral density (BMD) is a key determinant, with robust bone allowing for adequate press-fit. Low BMD, as seen in osteoporosis, is a significant challenge.
Osseointegration
This biological process involves direct structural and functional connection between ordered, living bone and the surface of a load-carrying implant. It is influenced by:
*
Implant Surface Characteristics:
Porosity, pore size (typically 50-400 µm for optimal ingrowth), surface roughness, and bioactive coatings (e.g., hydroxyapatite) enhance bone apposition.
*
Mechanical Stability:
Micromotion must be below the critical threshold (typically <50-150 µm) to promote bone ingrowth over fibrous tissue formation. Initial press-fit and geometric stability (e.g., fluted stems, metaphyseal filling designs) are essential.
*
Biological Factors:
Patient's healing capacity, systemic health, and absence of infection.
Stress Shielding
A biomechanical phenomenon where the stiffer implant carries a disproportionate amount of load, leading to reduced stress on the surrounding bone and subsequent bone resorption (Wolff's Law). Modern designs aim for more load sharing, particularly in the metaphysis, to minimize this effect.
Regional Anatomy Considerations (with focus on the knee per seed content)
Lower Extremity Alignment
Accurate restoration of mechanical axis and joint line is critical for balanced loading and longevity of cementless components. Standing hip-to-ankle alignment radiographs are essential for pre-operative assessment.
Knee Joint Specifics (as highlighted in seed content)
-
Ligamentous Structures:
- Medial and Lateral Collateral Ligaments (MCL, LCL): These provide varus/valgus stability. They must be protected at all times during bone cuts with retractors to prevent iatrogenic injury. Overtensioning or laxity can compromise implant stability and knee kinematics.
- Patellar Tendon: Essential for extensor mechanism function. Careful retraction and protection are needed during distal femoral and proximal tibial cuts.
- Posterior Cruciate Ligament (PCL): Its management (sacrifice or preservation) influences implant choice and surgical technique. If preserved, a ¼-inch osteotome is driven into the tibial plateau just anterior to the PCL to protect it during the tibial cut, ensuring its integrity and proper tensioning post-implantation.
-
Neurovascular Structures:
The posterior neurovascular structures (popliteal artery and vein, tibial nerve, common peroneal nerve) are at risk, especially during posterior capsule release or posterior osteophyte removal. Meticulous technique and careful use of retractors (e.g., bent Hohmann, broad bladed posterior retractors) are paramount to prevent injury.
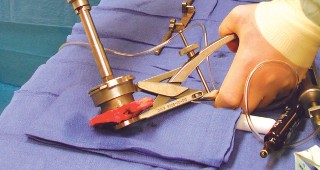
-

- Caption: Careful protection of neurovascular structures posteriorly is essential during tibial preparation and posterior capsule release in TKA.
-
Indications & Contraindications
The decision to utilize cementless fixation is multifactorial, weighing patient characteristics, bone quality, implant design, and surgeon experience.
Indications
Cementless fixation is generally preferred in situations where long-term biological fixation is desired and the host bone can provide adequate initial stability.
- Age: Younger patients (generally <65 years) are often candidates, as the potential for cement fatigue and aseptic loosening over a longer lifespan is a concern. However, excellent results have been obtained in patients older than 65 as well, challenging the traditional age-based cutoffs. The emphasis is shifting towards physiological age and bone quality rather than chronological age alone.
- Bone Quality: Good bone quality, implying sufficient cortical and cancellous bone stock, is paramount to achieve the necessary press-fit and subsequent osseointegration. This is often assessed pre-operatively via radiographs and sometimes CT scans.
- Patient Activity Level: Active patients who may place higher demands on their implants often benefit from the potentially more durable bone-implant interface of cementless components.
-
Specific Arthroplasties:
- Total Hip Arthroplasty (THA): Cementless acetabular components are the standard. Cementless femoral components are favored in younger, active patients with good bone stock (Dorr Type A or B femur).
- Total Knee Arthroplasty (TKA): Increasingly used for femoral, tibial, and patellar components. Indicated for tricompartmental arthritis of the knee that has failed nonoperative measures.
- Shoulder Arthroplasty: Cementless humeral stems and glenoid components (hybrid or all-cementless) are utilized, particularly in younger patients.
- Spine Surgery: Porous cages and interbody devices for fusion.
- Trauma: Certain fracture fixation devices (e.g., long gamma nails, some plate designs) incorporate cementless principles for improved biological integration.
- Revision Surgery: Cementless components can be advantageous in revision settings, especially when dealing with good bone stock or bone defects that require press-fit augments or porous metaphyseal sleeves.
Controversies & Nuances
- Weight and Inflammatory Arthritis: These are generally not absolute contraindications to cementless fixation. Modern implant designs and coating technologies have improved outcomes in these patient populations. However, careful consideration of bone quality, potential for systemic disease progression, and patient compliance is still necessary. In inflammatory arthritis, bone quality can be compromised by disease activity or long-term steroid use, requiring thorough pre-operative assessment.
- Age: While historically favored in younger patients, robust clinical data demonstrate excellent results for cementless THA and TKA in patients well over 65, provided bone quality is sufficient. The choice increasingly depends on individual bone characteristics.
Contraindications
-
Poor Bone Quality / Severe Osteoporosis:
This is a major contraindication (as identified in the seed content). Inadequate bone density may preclude achieving sufficient primary stability or subsequent osseointegration, leading to early loosening, subsidence, or periprosthetic fracture.
-

- Caption: Example of advanced osteoporosis where cementless fixation may be compromised due to inadequate bone stock for primary stability.
-
- Active Infection: Any active or recent periprosthetic infection is an absolute contraindication, as the porous surface can harbor bacteria, making eradication difficult.
- Significant Bone Deformity / Defects: While some defects can be managed with specialized cementless components or augments, severe deformities or large cavitary defects may make achieving stable primary fixation challenging.
- Severe Metabolic Bone Disease: Conditions like osteomalacia or advanced Paget's disease can impair bone healing and osseointegration.
- Compromised Healing Potential: Patients with severe immunosuppression, chronic renal failure, or those on certain medications (e.g., high-dose corticosteroids, bisphosphonates without drug holidays) may have impaired bone ingrowth potential.
- Allergy to Implant Materials: Rare, but a contraindication if documented.
Table: Operative vs. Non-Operative Indications for Arthroplasty (where Cementless is an Option)
| Category | Operative Indications (Arthroplasty) | Non-Operative Measures (Failure Precedes Arthroplasty) |
|---|---|---|
| Pain | Severe, debilitating joint pain unresponsive to non-operative management, significantly impacting quality of life, sleep, and daily activities. | Oral analgesics (NSAIDs, acetaminophen), physical therapy, corticosteroid injections, viscosupplementation, activity modification, weight loss, assistive devices (cane, walker). |
| Functional Impairment | Significant limitations in activities of daily living (ADLs) such as walking, stair climbing, rising from a chair, or self-care, due to joint stiffness, weakness, or instability. | Physical therapy for strengthening and range of motion, occupational therapy for ADL adaptation, assistive devices, lifestyle modification. |
| Radiographic Evidence | Advanced degenerative joint disease (e.g., Kellgren-Lawrence Grade 3 or 4 for knee, severe joint space narrowing, subchondral sclerosis, osteophytes, subchondral cysts), significant post-traumatic arthritis, avascular necrosis (late stages), inflammatory arthritis (with joint destruction) not controlled by medical management. | Mild to moderate radiographic changes without significant clinical correlation. |
| Failed Conservative Care | Documented failure of a comprehensive course of non-operative treatment (typically 3-6 months) to provide satisfactory symptom relief or functional improvement. This includes tricomp. arthritis of the knee not responding to non-operative measures. | Initial trial of all appropriate non-operative modalities. |
| Progressive Deformity | Progressive angular deformity (e.g., varus/valgus knee deformity), fixed flexion contracture, or leg length discrepancy contributing to symptoms and functional decline. | Orthotics, bracing, shoe lifts (for minor discrepancies), physical therapy to prevent contracture progression (though often ineffective for fixed deformity). |
| Quality of Life | Deterioration of mental health, social engagement, and overall well-being due to chronic pain and disability. | Psychological counseling, support groups, stress management. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful cementless arthroplasty, anticipating potential challenges and optimizing implant selection and surgical execution.
Patient Optimization
- Medical Evaluation: Comprehensive assessment of comorbidities (cardiac, pulmonary, renal, metabolic) to minimize perioperative risks. Optimization of chronic conditions (e.g., diabetes control, hypertension management).
- Nutritional Status: Address malnutrition or obesity; both can negatively impact wound healing and osseointegration.
- Smoking Cessation: Crucial at least 4-6 weeks pre-operatively to improve microcirculation and bone healing.
- Medication Review: Manage anticoagulants, antiplatelets, bisphosphonates. Discontinue NSAIDs pre-operatively due to potential impact on bone healing.
Imaging
-
Plain Radiographs:
-
Knee:
Weight-bearing anteroposterior (AP), lateral, and "sunrise" (patellofemoral) views are standard. Standing hip-to-ankle alignment radiographs are critical to assess the mechanical axis, degree of arthritis, and overall bone quality. These provide essential templating information.
-

- Caption: Standard weight-bearing AP radiograph of the knee, critical for assessing joint space narrowing, osteophytes, and overall alignment.
-

- Caption: Standing hip-to-ankle alignment radiograph, essential for determining the mechanical axis and planning corrective osteotomy or arthroplasty to restore neutral alignment.
-
- Hip: AP pelvis, AP hip, and cross-table lateral views. These allow assessment of acetabular and femoral bone stock, anatomy (e.g., Dorr classification for femur), and templating.
-
Knee:
Weight-bearing anteroposterior (AP), lateral, and "sunrise" (patellofemoral) views are standard. Standing hip-to-ankle alignment radiographs are critical to assess the mechanical axis, degree of arthritis, and overall bone quality. These provide essential templating information.
- Computed Tomography (CT) Scan: Indicated for complex cases, severe deformity, significant bone loss, or abnormal anatomy (e.g., severe dysplasia) to create 3D reconstructions and plan bone resections or defect management more precisely. This can also aid in assessing bone density if DEXA is not available or insufficient.
- Magnetic Resonance Imaging (MRI): Less frequently used for routine cementless arthroplasty planning but can be useful for assessing soft tissue pathologies, differentiating inflammatory conditions, or evaluating bone marrow edema pre-operatively.
Templating
Accurate templating using digital or physical templates over calibrated radiographs is vital for:
* Determining implant size and position.
* Anticipating leg length discrepancies.
* Estimating bone cuts and reaming depths.
* Identifying potential challenges (e.g., narrow canals, osteophytes).
*

*
Caption: Digital templating for femoral component sizing, ensuring appropriate fit and fill within the medullary canal for cementless fixation.
Patient Positioning
Proper positioning ensures optimal surgical exposure, prevents iatrogenic injury, and allows for accurate component alignment.
*
Total Knee Arthroplasty (TKA):
Supine on the operating table, often with a bump under the ipsilateral hip to allow for external rotation, and the foot of the table dropped or flexed to facilitate knee flexion. A tourniquet is typically applied high on the thigh.
*

*
Caption: Patient positioning for total knee arthroplasty, demonstrating appropriate preparation and draping for surgical exposure.
*
Total Hip Arthroplasty (THA):
*
Supine:
Often used for anterior approaches.
*
Lateral Decubitus:
Common for posterior and anterolateral approaches, providing good access to both the acetabulum and proximal femur. Careful padding of pressure points is essential.
Detailed Surgical Approach / Technique
The fundamental principle of cementless fixation is to achieve maximal primary mechanical stability, creating an environment conducive to biological ingrowth. This necessitates meticulous bone preparation and precise implant insertion.
General Principles for Cementless Fixation
- Exposure: Adequate surgical exposure, respecting soft tissue planes, is essential.
- Bone Preparation: Meticulous bone resection, reaming, or broaching to create a precise cavity that matches the implant's geometry. Bone surfaces must be free of soft tissue, cartilage, or debris.
- Primary Stability: Achieved through a "press-fit" or "scratch-fit" mechanism, which relies on the implant being slightly larger than the prepared bone cavity (e.g., 0.5-2 mm oversized reaming for acetabular components). This generates hoop stresses in the bone.
- Rotational Stability: Geometric features (e.g., fins, flutes, metaphyseal filling designs) of the implant are crucial to prevent rotation, which is highly detrimental to osseointegration.
- Load Transfer: Designs aim for physiological load transfer to the surrounding bone, minimizing stress shielding.
Example: Cementless Total Knee Arthroplasty (TKA)
1. Surgical Exposure
- Incision: Typically a midline longitudinal incision, often paramedian arthrotomy.
- Capsulotomy: Medial parapatellar approach is common. Patella eversion is performed.
- Soft Tissue Release: Careful release of medial structures (medial retinaculum, pes anserinus) as needed for exposure and alignment, while protecting the MCL.
2. Bone Resections (with emphasis on the knee, per seed content)
-
Distal Femoral Resection:
- Use an intramedullary (IM) guide for rotational alignment.
- Resect the appropriate amount of distal femur to restore joint line and create the desired valgus angle (typically 5-7 degrees).
- Careful protection of the medial and lateral collateral ligaments with retractors during all bone cuts is imperative.
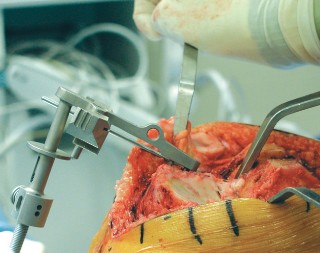
-

- Caption: Distal femoral resection using an intramedullary guide for accurate alignment in TKA.
-
Proximal Tibial Resection:
- Use an extramedullary (EM) guide for varus/valgus and posterior slope.
- Resect perpendicular to the mechanical axis, ensuring adequate bone stock for cementless component fixation.
- PCL Management: If preserving the PCL, a ¼-inch osteotome is driven into the tibial plateau just anterior to the PCL to protect it during the tibial cut. If sacrificing, it is released.
-

- Caption: Tibial resection using an extramedullary guide, ensuring correct posterior slope and alignment relative to the mechanical axis.
-
Femoral Sizing and Chamfer Cuts:
After distal cuts, sizing guides are used to determine anterior/posterior dimensions, and chamfer cuts are made to prepare for the femoral component.
-

- Caption: Femoral chamfer cuts being made, sculpting the bone for the posterior condylar component.
-
- Caption: Broaching the femoral canal for component sizing and fit. (This image also applies to hip, but can represent femoral preparation generally).
-
3. Ligament Balancing
- After bone cuts, the knee's flexion and extension gaps are assessed.
- Releases (e.g., posteromedial capsule, popliteus tendon, IT band) or rarely, restricted resection, are performed to balance the gaps symmetrically in flexion and extension.
- This is critical for optimal kinematics and long-term implant survival.
4. Component Preparation and Insertion
-
Femoral Component:
Impacted onto the prepared distal femur. Fins or pegs provide rotational stability.
-

- Caption: Insertion of the trial femoral component in TKA, verifying fit and stability prior to definitive implantation.
-
-
Tibial Component:
- The tibial plateau is prepared for the keel or peg(s) of the cementless tibial baseplate.
- Achieving a robust press-fit and rotational stability is paramount. Often, cancellous bone screws are used in conjunction with the press-fit to augment initial stability.
-

- Caption: Preparing the tibial plateau for the cementless tibial baseplate, including drilling for pegs or keel.
-

- Caption: Impaction of the cementless tibial component onto the prepared proximal tibia, ensuring stable press-fit.
-
Patellar Component:
Cementless patellar components are also available. Careful sizing and fixation are important.
-
- Caption: Drilling for patellar component pegs, preparing the patella for cementless resurfacing.
-
5. Trial Reduction and Final Implantation
- Trial components are inserted, and knee stability, range of motion, and patellar tracking are assessed.
- Once satisfactory, definitive cementless components are inserted, typically with firm impaction.
- Screws may be used in certain designs (e.g., tibial baseplates, acetabular shells) to further enhance initial mechanical fixation.
Example: Cementless Total Hip Arthroplasty (THA)
1. Acetabular Preparation
-
Reaming is performed sequentially, typically starting with an undersized reamer and progressing to an equal or 1-2 mm oversized reamer relative to the chosen cementless shell diameter. This creates the necessary press-fit.
-
- Caption: Example of acetabular reaming. (Can be interpreted as preparing the acetabulum broadly).
-
- The cementless acetabular shell is then impacted into place. Screw holes are often present for additional fixation, especially in cases of compromised bone quality or to improve stability in specific quadrants.
2. Femoral Preparation
-
The femoral canal is progressively broached using sequential broaches that create a shape matching the chosen femoral stem. The goal is to achieve metaphyseal fill and diaphyseal cortical contact for robust primary stability.
-
- Caption: Broaching the femoral canal for femoral component sizing and fit.
-
- The cementless femoral stem is impacted into place. Ensure correct anteversion/retroversion and leg length.
Complications & Management
While offering significant advantages, cementless fixation is not without its specific set of complications, which require careful recognition and management.
Common Complications and Salvage Strategies
| Complication | Incidence | Description & Etiology | Salvage Strategies |
|---|---|---|---|
| Early Aseptic Loosening / Subsidence | 1-3% (can be higher with poor technique/bone) | Failure to achieve adequate primary stability leading to excessive micromotion (>150 µm) and subsequent fibrous tissue formation instead of osseointegration. May present with persistent post-operative pain. Etiology: Inadequate press-fit, poor bone quality (e.g., osteoporosis). | Early revision to a cemented component or a larger cementless component with supplementary fixation (e.g., screws, augments) if bone stock allows. Bone grafting may be necessary. For subsidence without severe symptoms, watchful waiting may be an option, but often indicates impending failure. Revision to a long-stem cemented component for severe cases. |
| Stress Shielding | Variable, up to 50% radiographically | Bone resorption in areas unloaded by the stiffer implant, particularly distal femur with stiff femoral stems. Can lead to diaphyseal cortical thinning. Often asymptomatic, but can cause thigh pain. | For asymptomatic cases, no intervention needed. For symptomatic cases, conservative management (activity modification, analgesics). Revision to a more flexible, load-sharing stem design (e.g., short stem, metaphyseal-filling) if severe and debilitating. |
| Periprosthetic Fracture | 0.5-5% (higher in revisions, osteoporosis) | Fracture of the bone surrounding the implant. Can occur intraoperatively (during impaction) or postoperatively (due to stress risers, trauma, or loosening). Common sites: femoral shaft, proximal tibia. | Depends on fracture location, stability of implant, and bone quality (Vancouver, Modified Vancouver, Paprosky classifications). ORIF with plates/wires, stem revision (longer stem, cemented stem), cables, allograft struts. If implant is loose, revision is usually mandatory. |
| Thigh Pain | 5-15% (femoral cementless stems) | Persistent pain in the thigh, often attributed to micromotion at the tip of the stem, stiffness mismatch (stress shielding), or incomplete osseointegration. More common with fully porous-coated, stiff stems. | Conservative management (NSAIDs, activity modification) often resolves symptoms over time (up to 1-2 years post-op). If severe and persistent, revision to a more flexible, shorter stem, or cemented stem may be considered after ruling out other causes (infection, loosening). |
| Neurovascular Injury | <1% (rare but devastating) | Damage to nerves (e.g., sciatic, femoral, peroneal, tibial) or vessels (e.g., femoral, popliteal) during exposure, retraction, or component insertion. Specific to the knee, posterior neurovascular structures are vulnerable. | Immediate surgical exploration and repair. Post-operative nerve palsy may require extensive rehabilitation, nerve grafting, or tendon transfers. |
| Infection | <1% (early), up to 2% (late) | Periprosthetic joint infection (PJI) can complicate any arthroplasty. Cementless porous surfaces can be difficult to debride and sterilize. | Two-stage revision arthroplasty (explantation, debridement, antibiotic spacer, then reimplantation) is the gold standard for chronic PJI. Direct exchange in highly selected acute cases. Suppressive antibiotics. |
| Implant Malposition | Variable, dependent on surgeon skill | Incorrect component alignment or rotation, leading to instability, impingement, accelerated wear, or abnormal kinematics. | Revision surgery to correct alignment. For subtle malposition without severe symptoms, conservative management. |
| Heterotopic Ossification | 5-15% (can be higher with specific approaches/patients) | Formation of mature lamellar bone in periarticular soft tissues. Can cause pain and restricted range of motion. | Prophylaxis (NSAIDs, radiation therapy) in high-risk patients. Excision if symptomatic and mature. |
Post-Operative Rehabilitation Protocols
Rehabilitation following cementless arthroplasty aims to facilitate bone ingrowth while safely restoring joint function and strength. Protocols typically emphasize early mobilization but with specific considerations for weight-bearing and activity progression.
General Principles
- Early Mobilization: Essential to prevent complications such as deep vein thrombosis (DVT), pulmonary embolism (PE), and joint stiffness.
- Progressive Weight-Bearing: While many cementless constructs allow for immediate full weight-bearing (FWB) given adequate primary stability, some surgeons prefer protected weight-bearing (e.g., toe-touch, partial weight-bearing) for 4-6 weeks to minimize micromotion during the critical initial osseointegration phase, especially in cases of questionable bone quality or less than ideal press-fit.
- Gradual Increase in Activity: Avoid high-impact activities for several months to allow for robust bone ingrowth and implant maturation.
- Patient Education: Crucial for compliance with activity restrictions and adherence to exercises.
Phase 1: Acute Post-Operative (Day 0 - Week 6)
- Goals: Pain control, wound healing, prevention of DVT/PE, initiation of ROM, protected weight-bearing if indicated.
-
Weight-Bearing:
- THA: Typically FWB as tolerated immediately post-op for cementless stems/acetabular components. Precautions for dislocation based on approach.
- TKA: Often FWB as tolerated immediately post-op. In cases of concern for primary stability (e.g., softer bone, minimal press-fit), PWB or TTWB for 4-6 weeks may be prescribed.
-
Range of Motion (ROM):
- THA: Active and active-assistive ROM exercises within dislocation precautions.
- TKA: Continuous passive motion (CPM) machine often used, active and passive knee flexion/extension exercises (goal: 0-90 degrees by 2 weeks, increasing thereafter).
- Strengthening: Gentle isometric exercises (quadriceps sets, gluteal sets, ankle pumps).
-
Mobility:
Gait training with assistive devices (walker, crutches).
-
- Caption: Post-operative gait training with assistive devices is initiated early to promote mobility and manage weight-bearing. (This image also depicts an X-ray, but can be used metaphorically for gait training).
-
Phase 2: Intermediate Recovery (Week 6 - Month 3)
- Goals: Improve ROM, increase strength, normalize gait pattern, gradually decrease reliance on assistive devices.
- Weight-Bearing: Progress from protected to FWB if not already initiated.
- ROM: Continue to work on achieving full functional ROM (TKA goal: 0-120 degrees flexion).
- Strengthening: Progressive resistive exercises for all major muscle groups around the operated joint. Closed-chain exercises. Balance and proprioception training.
- Activity: Stair climbing, light cycling, swimming. Avoid deep squats, kneeling, and high-impact activities.
Phase 3: Advanced Recovery & Return to Activity (Month 3 - Month 6/12)
- Goals: Maximize strength and endurance, functional independence, gradual return to recreational activities.
- Strengthening: Continue advanced strengthening, sport-specific training for appropriate activities.
- Activity: Gradual return to low-impact sports (e.g., golf, doubles tennis, hiking on even terrain).
- Restrictions: High-impact activities (running, jumping, contact sports) are generally discouraged long-term for arthroplasty patients due to increased risk of wear and loosening, though patient-specific decisions are made.
Long-Term Considerations
-
Regular Follow-up:
Annual or biennial clinical and radiographic follow-up to monitor implant integrity, bone remodeling, and identify any signs of loosening or stress shielding.
-
- Caption: Post-operative X-ray for long-term follow-up, assessing implant position and integration. (This image also shows a trial femoral component, but can be used to imply follow-up X-ray).
-
- Infection Prophylaxis: Patient education on the importance of antibiotic prophylaxis for invasive procedures (dental work, urological procedures) to prevent hematogenous spread to the implant.
Summary of Key Literature / Guidelines
The body of literature supporting cementless fixation has grown exponentially, demonstrating comparable or superior long-term outcomes to cemented constructs in appropriate patient populations.
-
Total Hip Arthroplasty (THA):
- Acetabular Components: Cementless acetabular cups have become the standard of care due to excellent long-term survival rates (often >95% at 10-15 years) and lower rates of aseptic loosening compared to cemented cups. Studies by Engh and Glassman et al. established early benchmarks for successful osseointegration.
- Femoral Components: Meta-analyses and large registry studies (e.g., National Joint Registry for England, Wales, Northern Ireland and the Isle of Man) consistently show that cementless femoral stems perform very well, especially in younger, active patients with good bone quality. Long-term follow-up studies (e.g., 20+ years) have confirmed the durability of well-designed cementless stems, with rates of aseptic loosening often less than 5%. Concerns about thigh pain and periprosthetic fracture rates have been mitigated by design advancements (e.g., shorter stems, metaphyseal-filling designs, improved material properties).
-
Total Knee Arthroplasty (TKA):
- Historically, cemented TKA was considered the "gold standard," particularly in older patients. However, the performance gap between cementless and cemented TKA is narrowing.
- Recent randomized controlled trials and systematic reviews suggest that cementless TKA can achieve comparable clinical outcomes and survivorship to cemented TKA, particularly in patients aged <65-70 years with good bone quality.
- Advantages cited include reduced operative time (no cement drying time), potential for easier revision, and elimination of cement-related complications.
- The American Academy of Orthopaedic Surgeons (AAOS) and the American Association of Hip and Knee Surgeons (AAHKS) regularly update guidelines regarding arthroplasty. While these often focus on overall arthroplasty indications, the choice between cemented and cementless is increasingly patient- and surgeon-specific, informed by the growing evidence base.
- Concerns regarding fixation of the tibial component in cementless TKA have led to innovations in surface technology (e.g., highly porous metals) and screw augmentation to enhance primary stability. Some designs are now demonstrating excellent long-term results.
-
Emerging Technologies: The field continues to evolve with advanced porous coatings (e.g., trabecular metal, highly porous titanium), bioactive surfaces, and additive manufacturing (3D printing) allowing for customized implant geometries and enhanced biological fixation. Robotics and navigation also play a role in optimizing component positioning for cementless implants, aiming for greater precision and reduced malalignment, which is critical for long-term osseointegration.
In conclusion, cementless fixation has matured into a reliable and often preferred method for arthroplasty across various joints. Mastery of the techniques demands a deep understanding of surgical anatomy, meticulous execution to achieve primary stability, careful patient selection, and comprehensive post-operative management. Continuous engagement with evolving literature and adherence to best practices are essential for overcoming pitfalls and optimizing patient outcomes.
Clinical & Radiographic Imaging