Patient Presentation & History
A 38-year-old male, previously fit and healthy, presented to the emergency department following a 10-foot fall from a ladder onto both feet. He immediately experienced severe bilateral heel pain, rendering him unable to bear weight. The mechanism of injury was a direct axial load through the lower extremities.
His medical history was unremarkable, with no known comorbidities such as diabetes, peripheral vascular disease, or osteopenia, which are crucial considerations in fracture healing and surgical planning. He is an active smoker, consuming approximately 15 pack-years. Social history includes employment as a construction worker, highlighting the significant functional implications of lower extremity injury. There were no reported allergies and he was not on any regular medications.
Upon initial assessment, specific inquiry was made regarding other potential injuries, especially those associated with high-energy axial loading. This included symptoms referable to the lumbar spine, which is crucial given the incidence of concomitant spinal fractures (up to 10-15% in calcaneal fractures), as well as injuries to the talus, pilon, or contralateral foot. The patient denied any back pain, loss of sensation, or motor weakness.
Clinical Examination
Initial examination revealed significant swelling and ecchymosis extending from the hindfoot into the midfoot bilaterally, more pronounced on the left. The skin over both heels, particularly the lateral aspects, appeared tense and shiny, raising concerns for impending fracture blisters and soft tissue compromise. Mondor's sign (hematoma extending to the sole of the foot) was present on the left. No open wounds were observed, and there were no signs of gross deformity, though the normal calcaneal contour was lost due to swelling.
Palpation elicited exquisite tenderness over the calcaneal tuberosity and along the lateral aspect of both calcanei. Crepitus was present on gentle manipulation of the left hindfoot. The Achilles tendon was intact bilaterally, and the integrity of the fibula, tibia, and talus was assessed by careful palpation to rule out associated fractures.
Gross range of motion of the ankle and subtalar joint was severely limited due to pain and swelling, preventing a precise assessment. Both feet were held in a position of slight dorsiflexion due to muscle spasm.
Neurological assessment revealed intact sensation in the distribution of the sural, superficial peroneal, deep peroneal, tibial, and saphenous nerves bilaterally. Motor function of the ankle dorsiflexors, plantarflexors, invertors, and evertors was limited by pain but appeared grossly intact when resisted. Distal pulses (dorsalis pedis and posterior tibial) were strong and symmetric bilaterally, and capillary refill was prompt. Compartment pressures were not overtly elevated, but the presence of significant swelling mandated close monitoring for potential compartment syndrome, particularly in the midfoot. Close attention was paid to the skin integrity, noting areas of blanching with pressure, indicative of potential flap compromise if an immediate surgical approach were contemplated.
Imaging & Diagnostics
Initial imaging commenced with plain radiographs of both feet and ankles, and a focused lumbar spine series to exclude associated injuries.
X-ray Findings (Left Calcaneus):
*
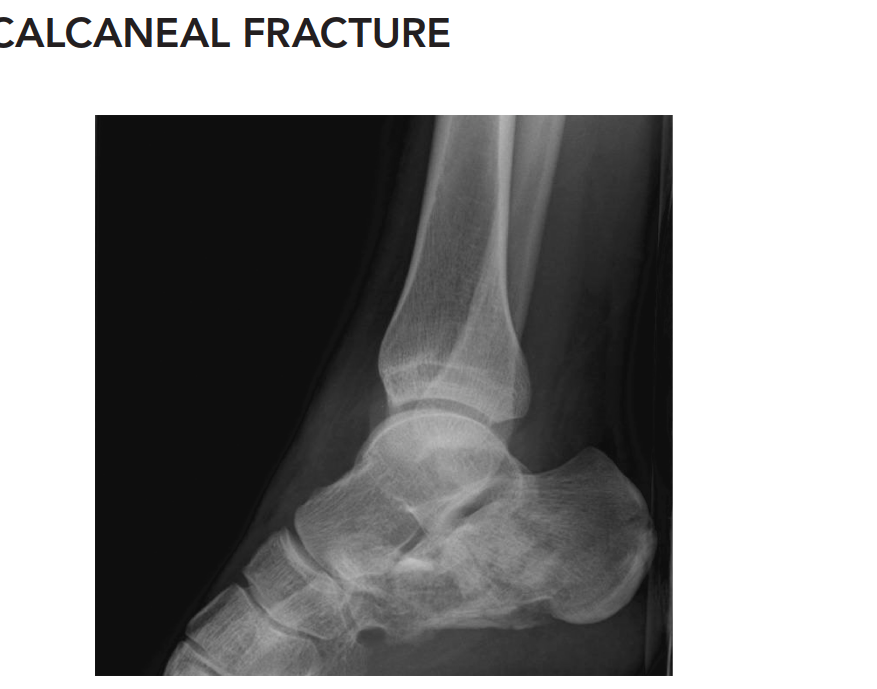
Lateral View:
Demonstrated a significant decrease in Bohler's angle (measured at 5 degrees, normal 20-40 degrees), indicative of substantial collapse of the posterior facet and loss of calcaneal height. Gissane's angle (Crucial angle) was increased to 140 degrees (normal 100-120 degrees), reflecting the disruption of the lateral process of the talus and the primary fracture line. There was clear evidence of a tongue-type fracture pattern with extension into the subtalar joint. Loss of calcaneal length and significant posterior facet depression were also evident.
*
Axial (Harris) View:
Revealed marked broadening of the calcaneus and a varus malalignment of the tuberosity. Significant comminution of the lateral wall was observed. Disruption of the sustentaculum tali was also suspected.
*
AP Ankle View:
Showed no evidence of ankle mortise injury, pilon fracture, or fibular fracture.
X-ray Findings (Right Calcaneus):
* Less severe, non-displaced extra-articular fracture of the calcaneal tuberosity. Bohler's angle was preserved at 30 degrees. This was initially planned for non-operative management.
CT Scan Indications & Findings:
Given the significant displacement and intra-articular involvement seen on plain radiographs, a Computed Tomography (CT) scan of both feet was deemed essential for definitive classification, detailed characterization of the fracture pattern, and meticulous pre-operative planning.

CT Scan (Left Calcaneus) Findings:
*
Coronal Views:
Demonstrated severe comminution of the posterior facet of the subtalar joint. The most prominent fracture line passed through the posterior facet, creating multiple articular fragments. Sustentacular involvement was confirmed, with a medial fragment displaced. The lateral wall was blown out, causing significant calcaneal broadening.
*
Sagittal Views:
Confirmed the substantial depression of the posterior facet and the severe loss of Bohler's angle. The tongue-type fracture pattern was clearly delineated, with the posterior superior fragment articulating with the Achilles tendon insertion.
*
Axial Views:
Provided precise measurements of the calcaneal broadening (increased by 25mm compared to the contralateral side) and corroborated the lateral wall comminution. The posterior facet involvement was extensively mapped.
Based on the CT findings, the left calcaneal fracture was classified as a Sanders Type IIIBC fracture (severe comminution involving the posterior facet with three articular fragments, one involving the sustentaculum, and lateral wall comminution), indicating a complex, highly unstable intra-articular injury requiring surgical intervention. The right calcaneal fracture was confirmed as a minimally displaced extra-articular tuberosity fracture, amenable to conservative management.
MRI Indications:
Magnetic Resonance Imaging (MRI) was not indicated in the acute setting for primary diagnosis of the calcaneal fracture, as CT provided sufficient detail for bony injury and surgical planning. MRI might be considered in cases of suspected associated ligamentous injury (e.g., spring ligament, deltoid ligament), occult talar or navicular fractures not visualized on CT, or to evaluate soft tissue injuries such as peroneal tendon pathology in a delayed presentation. In this case, with clear bony pathology on CT, MRI was deferred.
Templating:
Pre-operative templating was performed meticulously using the CT scans. This involved assessing the contralateral uninjured calcaneus for reference to restore calcaneal height, length, and width. The anticipated placement of a contoured locking calcaneal plate and appropriate screw lengths for articular fragment fixation and sustentacular screw placement were planned. Consideration for potential bone graft volume to fill any metaphyseal defects after reduction was also made.
Differential Diagnosis
The primary diagnosis in this case is a calcaneal fracture. However, in the setting of a high-energy axial load injury to the foot and ankle, several other injuries must be considered and systematically ruled out.
| Feature | Calcaneal Fracture (Case Presentation) | Talus Fracture (e.g., Neck/Body) | Pilon Fracture (Distal Tibia) | Midfoot Fracture/Dislocation (e.g., Lisfranc) |
|---|---|---|---|---|
| Mechanism | High-energy axial load (fall from height onto heels). | High-energy axial load, dorsiflexion injury. | High-energy axial load, rotational forces. | High-energy axial load with rotational component. |
| Primary Pain Site | Heel, hindfoot. | Ankle, hindfoot, midfoot. | Ankle, distal tibia. | Midfoot, often medial side. |
| Clinical Signs | Significant heel swelling, ecchymosis (Mondor's sign), tenderness over calcaneus, loss of calcaneal contour. Compartment syndrome risk. | Ankle swelling, tenderness over talus, often severe deformity with displacement. | Significant ankle swelling, tenderness over distal tibia/fibula, crepitus, potential open injury. | Midfoot swelling, tenderness over tarsometatarsal joints, often plantar ecchymosis. "Gap" on palpation. |
| X-ray Findings | Lateral: ↓ Bohler's angle, ↑ Gissane's angle, loss of height/length, tongue-type or joint depression patterns. Axial: Broadening, varus. | AP/Lateral/Mortise: Fracture lines through talar neck, body, dome; displacement, often avascular necrosis risk. | AP/Lateral/Mortise: Articular incongruity of plafond, metaphyseal comminution, fibular fracture often present. | AP/Lateral/Oblique: Widening of TMT joint spaces (Lisfranc diastasis), fleck sign (avulsion), displacement. |
| CT Indication | Essential for classification (Sanders), articular involvement, surgical planning. | Essential for understanding fracture pattern, displacement, AVN risk. | Essential for articular involvement, comminution, surgical approach planning. | Essential for subtle dislocations, comminution, extent of ligamentous injury. |
| Associated Injuries | Lumbar spine fractures, contralateral calcaneal fractures, pilon/talus, ankle sprains. | Calcaneal fractures, pilon, ankle ligaments, navicular. | Calcaneal, talar fractures, ankle ligamentous injuries, fibular fractures. | Cuboid, cuneiform, navicular fractures, ankle sprains, compartment syndrome. |
| Treatment | Often ORIF (lateral approach for Sanders IIIBC) for displaced intra-articular, non-operative for non-displaced. | ORIF for displaced fractures (often medial/lateral approaches), non-operative for non-displaced. | ORIF for displaced articular fractures, often requiring staged approach for soft tissue. | ORIF for unstable injuries, non-operative for stable non-displaced. |
Surgical Decision Making & Classification
Surgical Decision Making:
The decision for operative versus non-operative management of calcaneal fractures is multifactorial, considering fracture type, patient factors, and soft tissue status.
Indications for Operative Fixation (Left Calcaneus):
Our patient's left calcaneal fracture presented with clear indications for surgical intervention:
1.
Displaced Intra-articular Fracture:
The Sanders Type IIIBC classification signifies significant displacement and comminution of the posterior facet, directly involving the subtalar joint. Failure to anatomically reduce these fragments leads to poor functional outcomes and early degenerative arthritis.
2.
Significant Loss of Calcaneal Height & Length:
The Bohler's angle of 5 degrees indicated substantial collapse, which contributes to impingement syndromes, altered gait mechanics, and difficulty wearing shoes.
3.
Calcaneal Broadening:
The marked increase in calcaneal width due to lateral wall blowout can lead to painful impingement on the lateral malleolus and difficulty fitting into footwear.
4.
Young, Active Patient:
At 38 years old and working in construction, the patient has high functional demands. Surgical reconstruction aims to restore hindfoot anatomy and function, allowing a return to pre-injury activity levels.
5.
Lack of Absolute Contraindications:
While he is a smoker, which increases wound complication risk, this alone was not an absolute contraindication, but rather a factor requiring counseling and strict post-operative monitoring. His otherwise healthy status, without severe comorbidities, favored operative management.
Contraindications for Operative Fixation (Not present in this case, but important considerations):
* Severe open fractures (Gustilo Type IIIB or IIIC) with extensive soft tissue loss or contamination.
* Significant comorbidities precluding anesthesia or prolonged surgery (e.g., severe peripheral vascular disease, uncontrolled diabetes, severe immunocompromise).
* Non-ambulatory patient or extremely elderly patients with low functional demands (often managed non-operatively).
* Extremely poor soft tissue envelope (e.g., severe fracture blisters, necrosis, severe swelling not resolving after adequate delay).
* Severe crush injury with unsalvageable foot.
Non-Operative Management (Right Calcaneus):
The right calcaneal fracture was a minimally displaced extra-articular tuberosity fracture. Given its stable nature and minimal involvement of the subtalar joint, this was managed non-operatively with a short-leg non-weight-bearing cast for 6-8 weeks, followed by progressive weight-bearing and physiotherapy.
Classification Systems for Calcaneal Fractures:
-
Essex-Lopresti Classification (Based on Lateral X-ray):
- Tongue-Type: The primary fracture line extends posteriorly, separating a superior fragment (tongue) containing the posterior facet from the main body. The Achilles tendon inserts onto this fragment. This pattern is associated with skin compromise if displaced superiorly.
- Joint Depression-Type: The primary fracture line involves the posterior facet, which is depressed directly into the body of the calcaneus, without forming a distinct "tongue."
- Our patient's left calcaneus showed features of a tongue-type fracture on lateral X-ray.
-
Sanders Classification (Based on CT Coronal Views through Posterior Facet):
- The gold standard for intra-articular calcaneal fractures. Divides the posterior facet into three columns using two primary fracture lines (A and B). A third fracture line (C) involves the medial wall/sustentaculum.
- Type I: Non-displaced intra-articular (fracture lines without displacement >2mm).
-
Type II:
Two-part fracture of the posterior facet.
- IIA: Fracture line lateral to the A line.
- IIB: Fracture line between A and B lines.
- IIC: Fracture line medial to the B line.
-
Type III:
Three-part fracture of the posterior facet.
- IIIA: Two fracture lines lateral to the C line.
- IIIB: One fracture line between A and B, one medial to B.
- IIIC: One fracture line between A and B, one medial to C.
- Type IV: Highly comminuted, four or more articular fragments (often unsalvageable).
- Our patient's left calcaneus was classified as Sanders Type IIIBC , indicating severe comminution with involvement of the sustentaculum, aligning with the complexity requiring ORIF.
-
Zwipp Classification:
- A more comprehensive classification system that considers the number of fracture fragments, involvement of all three joint facets (posterior, middle, anterior), and extra-articular components. While detailed, it is less commonly used for routine surgical planning compared to Sanders.
Surgical Technique / Intervention (Left Calcaneus)
The surgical intervention for the left calcaneal fracture was delayed by 7 days to allow for resolution of soft tissue swelling and the appearance of the "wrinkle sign," indicating that the soft tissue envelope was amenable to surgery. This minimizes the risk of wound complications such as dehiscence and infection.
Patient Positioning:
The patient was positioned in the
lateral decubitus position
on the operating table, with the injured left foot facing upwards. This provides optimal access for the extensile lateral approach. A bump was placed under the contralateral hip to stabilize the patient. The ipsilateral limb was prepped and draped from above the knee to the toes, allowing for assessment of leg rotation and potential fluoroscopic imaging. A tourniquet was applied to the thigh.
Surgical Approach:
An
extensile lateral approach
(or lateral L-shaped incision) was chosen. This is the workhorse approach for displaced intra-articular calcaneal fractures, providing excellent visualization of the posterior facet, lateral wall, and calcaneal body.
1.
Incision:
A curvilinear incision was made starting approximately 2 cm posterior and superior to the tip of the lateral malleolus, curving distally along the lateral border of the foot, turning at the calcaneocuboid joint, and extending posteriorly along the plantar aspect of the calcaneal tuberosity.
2.
Full-Thickness Flap Elevation:
A full-thickness fasciocutaneous flap was carefully elevated anteriorly and superiorly. This involved dissecting superficial to the peroneal tendons and their sheath. The key is to include the sural nerve and its branches within the flap to protect them from iatrogenic injury. The flap was retracted superiorly and anteriorly, often secured with K-wires inserted into the tibia or fibula.
3.
Exposure:
This exposed the lateral wall of the calcaneus, the peroneal tendons (retracted superiorly), and the subtalar joint. The fracture hematoma was evacuated.
Reduction Techniques:
The goal of reduction was to restore: 1) the articular surface of the posterior facet, 2) calcaneal height, 3) calcaneal length, and 4) calcaneal width, and subsequently, Bohler's and Gissane's angles.
1.
Restoration of Height and Length:
* A Schanz pin or a large Steinmann pin was inserted into the calcaneal tuberosity and used as a "joy-stick" to distract the tuberosity fragment distally and posteriorly. This maneuver helps to unimpact the depressed fragments and restore calcaneal length.
* Another pin was often placed into the talus for counter-traction.
2.
Lateral Wall Reduction:
* The "blown-out" lateral wall was often comminuted and displaced laterally. These fragments were carefully removed to allow access to the underlying depressed articular fragments.
* Once the posterior facet was reduced, the lateral wall fragments were repositioned and reconstructed, often with K-wire fixation or direct screw fixation, effectively reducing the calcaneal broadening.
3.
Posterior Facet Reduction:
* This is the most critical step. Using a lamina spreader or small osteotomes, the posterior facet fragments were disimpacted from the underlying cancellous bone.
* A curved elevator (e.g., periosteal elevator, freer) was then inserted through the lateral window into the subtalar joint. Under direct visualization and fluoroscopic guidance (oblique Broden's view for articular reduction), the depressed posterior facet fragments were meticulously elevated and anatomically reduced to the talus.
* Once reduced, the articular fragments were temporarily secured with multiple small K-wires passed percutaneously or directly through the fragments.
4.
Sustentacular Fragment Reduction:
* The sustentaculum tali fragment, if involved, was reduced under direct visualization and secured. This often serves as a key medial buttress.
Fixation Construct:
1.
Internal Fixation:
After satisfactory anatomical reduction of the posterior facet and restoration of overall calcaneal morphology, definitive fixation was performed.
* An anatomically contoured
lateral locking calcaneal plate
was applied to the lateral aspect of the calcaneus. The plate provides stable buttressing for the lateral wall and holds the reduced fragments.
* Lag screws were placed across the articular fragments to achieve interfragmentary compression, followed by locking screws into the calcaneal body and tuberosity for angular stability.
* Special attention was paid to placing long screws into the sustentaculum tali from the lateral plate, as this medial pillar is crucial for hindfoot stability. These sustentacular screws ideally pass into the medial fragment without transgressing the joint.
2.
Bone Grafting:
After reduction, a metaphyseal void often remains beneath the elevated posterior facet. In this case, due to significant comminution and depression, an allograft cancellous bone chip graft was packed into this void to provide structural support and promote healing.
3.
Final Checks:
Fluoroscopic images (lateral, axial, Broden's views) were taken to confirm hardware placement, articular reduction, restoration of Bohler's and Gissane's angles, and overall calcaneal morphology.
Wound Closure:
The flap was carefully irrigated and returned to its anatomical position. A drain was placed beneath the flap to manage hematoma and seroma formation. The deep fascia was loosely closed, and the skin was closed with non-absorbable sutures, ensuring no tension on the skin edges. A sterile dressing and a well-padded posterior splint were applied.
Post-Operative Protocol & Rehabilitation
The post-operative protocol for a complex calcaneal fracture aims to protect the surgical repair, manage pain and swelling, prevent complications, and gradually restore function.
Immediate Post-Operative (Day 0-14):
*
Immobilization:
The limb was immediately placed in a well-padded posterior splint or short-leg cast, holding the foot in a neutral position.
*
Weight-Bearing:
Strictly
non-weight-bearing (NWB)
on the operated left foot. The patient was instructed to use crutches or a knee scooter. The right foot, having a non-displaced fracture, was also NWB initially in a walking boot.
*
Elevation:
Strict elevation of the operative limb above heart level to minimize swelling.
*
Pain Management:
Multimodal analgesia including opioids, NSAIDs (if not contraindicated), and acetaminophen.
*
Wound Care:
Daily wound checks for signs of infection, dehiscence, or hematoma. Drain care (removed when output <30ml/24hr, typically within 2-3 days).
*
Thromboprophylaxis:
Chemical (e.g., LMWH) and mechanical (e.g., compression stockings, pneumatic pumps) prophylaxis for deep vein thrombosis (DVT) and pulmonary embolism (PE).
*
Smoking Cessation:
Aggressive counseling and support for smoking cessation were initiated immediately, given its profound negative impact on wound healing and bone union.
Early Rehabilitation (Weeks 2-8):
*
Suture Removal:
At 2-3 weeks post-op.
*
Immobilization:
Transition from splint to a removable short-leg cast or controlled ankle motion (CAM) boot.
*
Weight-Bearing:
Continued
NWB
. Patient instructed on gentle ankle active range of motion (ROM) exercises (dorsiflexion, plantarflexion, circumduction)
out of the boot
to prevent stiffness, but strictly avoiding subtalar motion (inversion/eversion) as this puts stress on the healing posterior facet.
*
Soft Tissue Management:
Scar massage and desensitization once the wound is healed. Edema control with compression stockings.
*
Physical Therapy (PT) Focus:
Gentle, non-stressful exercises for the ankle, strengthening of intrinsic foot muscles, hip, and knee strength training to maintain overall fitness and aid in crutch ambulation.
Progressive Rehabilitation (Weeks 8-12):
*
Imaging:
Follow-up radiographs (AP, lateral, axial) at 8-10 weeks post-op to assess fracture healing.
*
Weight-Bearing:
If radiographic signs of union are progressing and clinical tenderness is resolving, gradual
partial weight-bearing (PWB)
can begin, typically starting with 25% body weight in a CAM boot, progressing to 50% over 2-4 weeks.
*
Physical Therapy Focus:
* Continued ankle ROM exercises, now incorporating gentle subtalar ROM (inversion/eversion).
* Gradual strengthening exercises for ankle dorsiflexors, plantarflexors, invertors, and evertors.
* Proprioceptive training (e.g., balance board, single-leg stance) as tolerated.
* Gait training with crutches, focusing on proper heel-toe progression.
Advanced Rehabilitation (Weeks 12-6 Months):
*
Weight-Bearing:
Transition from CAM boot to supportive shoes with custom orthotics as tolerance allows. Full weight-bearing (FWB) is typically achieved by 12-16 weeks if union is confirmed.
*
Physical Therapy Focus:
* Progression to advanced strengthening, balance, and agility drills.
* Cardiovascular conditioning (e.g., stationary cycling, swimming).
* Return to work/sport-specific training, gradually increasing impact activities.
* Addressing any remaining gait abnormalities.
*
Hardware Removal:
Considered 12-18 months post-op, usually only if symptomatic (e.g., hardware prominence, peroneal tendon irritation).
Long-Term Follow-up:
* Continued monitoring for complications such as subtalar arthritis (common even with good reduction), chronic pain, malunion, nonunion, or peroneal tendinopathy.
* Custom orthotics are often beneficial long-term to accommodate any residual foot shape changes or provide support.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Soft Tissue Envelope is King: Always prioritize soft tissue healing. Delay surgery until the "wrinkle sign" appears (typically 7-14 days post-injury) to minimize wound complications, especially with the extensile lateral approach.
- Rule out Associated Injuries: In high-energy calcaneal fractures, systematically evaluate for lumbar spine fractures (10-15%), contralateral calcaneal fractures (10%), and other lower extremity injuries (pilon, talus, hip).
- CT is Essential: Plain radiographs are only screening tools. A fine-cut CT scan is mandatory for classification (Sanders), understanding the fracture morphology, and pre-operative templating.
-
Sequential Reduction Principles:
- First, restore the posterior facet: This is the most critical step for long-term functional outcome and preventing post-traumatic arthritis. Use direct visualization and fluoroscopic guidance (Broden's views).
- Second, restore calcaneal height and length: Use a "joy-stick" maneuver to pull the tuberosity fragment distally and posteriorly to disimpact depressed fragments.
- Third, reconstruct the lateral wall and restore width: This prevents impingement and improves shoe wear.
- Sural Nerve Protection: During the extensile lateral approach, ensure the sural nerve (and its branches) are protected within the full-thickness fasciocutaneous flap. Iatrogenic injury can lead to chronic neuropathic pain.
- Sustentacular Screw: A strong screw or screws directed from the lateral plate into the sustentaculum tali is crucial for medial column stability and prevention of varus collapse.
- Bone Grafting: Consider using allograft or autograft (e.g., from iliac crest or distal tibia) to fill metaphyseal voids created after elevating the posterior facet, providing structural support and promoting union.
- Smoking Cessation: Aggressively counsel patients on smoking cessation, as it significantly increases the risk of wound dehiscence, infection, and nonunion.
Pitfalls:
- Operating Too Early: Performing surgery on a swollen, tense foot with fracture blisters leads to unacceptably high rates of wound breakdown, infection, and potentially flap necrosis. Impatience is a significant risk factor.
- Inadequate Reduction of the Posterior Facet: Failure to achieve anatomical or near-anatomical reduction of the subtalar joint's posterior facet is the primary cause of chronic pain and early subtalar arthrosis, often necessitating future subtalar fusion.
- Ignoring Calcaneal Width: Not reducing the lateral wall blowout leads to impingement of the lateral malleolus, peroneal tendinopathy, and difficulty wearing shoes.
- Poor Flap Handling: Excessive traction, inadequate protection of the flap, or aggressive dissection can compromise its vascularity, leading to skin necrosis.
- Over-Reduction or Under-Reduction: Both can lead to problems. Over-reduction can cause impingement; under-reduction leads to residual deformity and poor function.
- Ignoring the Medial Column: Failure to address sustentacular involvement or medial comminution can lead to varus malunion or continued instability.
- Early Weight-Bearing: Premature weight-bearing can lead to loss of reduction, hardware failure, nonunion, or malunion. Strict NWB for at least 8-12 weeks is critical.
- Missing Compartment Syndrome: Calcaneal fractures, especially those with significant crush injury, carry a risk of foot compartment syndrome, requiring a high index of suspicion and timely fasciotomy if suspected.
- Insufficient Pre-operative Planning: Lack of detailed CT analysis and templating can lead to surprises in the operating room, prolonging surgery and increasing complications.
