Patient Presentation & History
A 32-year-old male, otherwise fit and healthy, presented to the Emergency Department following a high-energy motor vehicle accident as a restrained passenger. He reported significant immediate pain and deformity in his left ankle and foot, rendering him unable to bear weight. The mechanism described was an axial load through a dorsiflexed foot with a pronation-eversion component, consistent with the foot being trapped under the dashboard. He denied any significant past medical history, particularly no prior foot or ankle injuries, no diabetes, peripheral vascular disease, or neuropathic conditions. His only regular medication was a multivitamin. He is a non-smoker and consumes alcohol socially. His tetanus immunization status was up to date.
Clinical Examination
Upon initial assessment in the trauma bay, the patient was alert and oriented.
His vital signs were stable.
Inspection
The left hindfoot and midfoot displayed a marked and obvious deformity. Specifically, there was significant valgus angulation of the hindfoot with prominent lateral displacement of the calcaneus relative to the talus. The talar head was palpable medially, beneath the navicular. The skin overlying the talar head appeared stretched and was under significant tension, displaying pallor and early signs of impending necrosis. There was no gross skin breach, but the integrity was compromised due to the underlying bony prominence. Swelling was rapidly increasing around the ankle and midfoot. No obvious signs of open injury were noted, though careful scrutiny was performed due to the high-energy mechanism.
Palpation
Marked tenderness was elicited diffusely over the ankle joint and subtalar joint complex, extending into the midfoot. The talar head was distinctly palpable medially. The calcaneus was displaced laterally and anteriorly. Bony crepitus was not appreciated. Crucially, the dorsalis pedis and posterior tibial pulses were strong and bilaterally symmetrical. Capillary refill in all toes was brisk (<2 seconds).
Range of Motion
Active and passive range of motion of the ankle and foot was severely restricted due to pain and mechanical blockade from the dislocation. Attempted movements exacerbated the patient's discomfort significantly.
Neurological & Vascular Assessment
A thorough neurological examination of the left lower extremity revealed no deficits. Sensation was intact to light touch and pinprick in all dermatomes (L4, L5, S1, S2). Motor function was intact in all major muscle groups (ankle dorsiflexion, plantarflexion, inversion, eversion, toe flexion/extension). As noted, vascular status was excellent with palpable pulses and brisk capillary refill, indicating no acute compromise, despite the skin tension. Given the evolving soft tissue envelope and high-energy mechanism, close monitoring of neurovascular status and skin integrity was paramount.
Imaging & Diagnostics
Following clinical assessment, initial plain radiographs of the left foot and ankle were obtained in the Emergency Department.
X-ray Findings
Standard orthogonal views (AP, lateral, and oblique views of the foot, and AP/lateral views of the ankle) were reviewed.
- Lateral View: Demonstrated complete loss of articulation between the talus and calcaneus, and between the talus and navicular. The talus remained congruent with the distal tibia, indicating a true subtalar dislocation. The calcaneus was displaced laterally and anteriorly relative to the talus. The talar head was seen to be dislocated medially from the navicular. This pattern is consistent with a medial subtalar dislocation .
- AP View: Confirmed the medial displacement of the talar head from the navicular. The calcaneus appeared in valgus relative to the talus.
- Oblique View: Provided additional perspective on the talonavicular disarticulation.
- Ankle Views: Demonstrated no concomitant tibiotalar dislocation or significant ankle fracture.
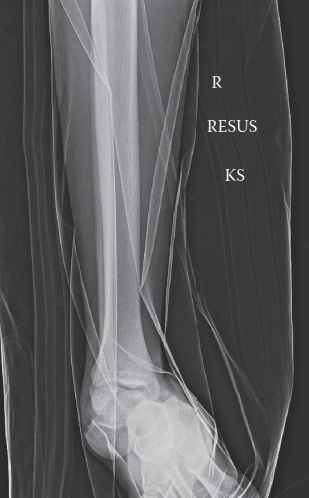
Representative lateral radiograph demonstrating a medial subtalar dislocation. Note the intact tibiotalar articulation and complete loss of alignment between the talus, calcaneus, and navicular.
CT/MRI Indications & Templating
-
Computed Tomography (CT) Scan:
-
Immediately following the preliminary assessment and initial radiographs, a CT scan of the left foot and ankle was requested. This was crucial for:
- Confirmation of Dislocation Pattern: To precisely characterize the direction and extent of the subtalar dislocation (medial in this case).
- Detection of Associated Fractures: High-energy mechanisms frequently result in concomitant osseous injuries. The CT allows for detailed assessment of the talus, calcaneus, navicular, cuboid, and distal tibia for subtle or occult fractures that may not be apparent on plain radiographs. These can include talar dome osteochondral lesions, talar neck/body fractures, calcaneal sustentacular fractures, or cuboid compression fractures. In this patient, the CT revealed a small, non-displaced fracture of the posterior process of the talus, not engaging the subtalar joint, and a minor avulsion of the calcaneal tuberosity, which did not preclude closed reduction.
- Identification of Intra-Articular Fragments: Crucial for planning potential open reduction, as incarcerated fragments can block closed reduction.
- Assessment of Articular Surface Integrity: While immediate reduction is the priority, CT provides baseline information regarding the subtalar and talonavicular joint surfaces.
- A CT scan is almost universally indicated in subtalar dislocations post-reduction to ensure concentric reduction and rule out incarcerated fragments or unstable associated fractures that mandate operative intervention.
-
Immediately following the preliminary assessment and initial radiographs, a CT scan of the left foot and ankle was requested. This was crucial for:
-
Magnetic Resonance Imaging (MRI):
- MRI is generally not indicated acutely for subtalar dislocations unless there is suspicion of significant ligamentous injury contributing to persistent instability after reduction, or for assessment of potential osteochondral lesions or avascular necrosis (AVN) of the talus in the subacute or chronic phase, particularly if complications arise or if prolonged symptoms persist despite adequate bony reduction. In the acute setting, the primary focus is rapid reduction and bony assessment.
-
Templating:
- Templating in the acute setting of subtalar dislocation primarily revolves around pre-planning for potential operative intervention if closed reduction fails or if significant associated fractures require fixation. This includes selecting appropriate hardware (screws, plates, K-wires) and considering surgical approaches. For straightforward closed reductions, traditional templating is less relevant, but detailed CT analysis guides the decision-making process for subsequent management.
Differential Diagnosis
Subtalar dislocation must be differentiated from other common and uncommon midfoot and hindfoot injuries, particularly given similar mechanisms of injury and presentation of pain and deformity.
| Feature | Subtalar Dislocation (Our Case) | Ankle (Tibiotalar) Dislocation | Talonavicular Dislocation (Isolated) | Midfoot (Chopart/Lisfranc) Dislocation |
|---|---|---|---|---|
| Definition | Dislocation of the talocalcaneal and talonavicular joints, with tibiotalar joint remaining intact. | Complete loss of articulation between the distal tibia/fibula and the talus. | Isolated disruption of the talonavicular joint. | Disruption of tarsometatarsal (Lisfranc) or talonavicular & calcaneocuboid (Chopart) joints. |
| Mechanism of Injury | High-energy axial load with pronation-eversion (medial) or supination-inversion (lateral). Often sports or MVA. | High-energy, often MVA or fall. Severe dorsiflexion, plantarflexion, or rotational forces. Often associated with fractures. | Forced abduction/adduction or rotation of the forefoot/midfoot on a fixed hindfoot. | High-energy axial load onto plantarflexed foot (Lisfranc) or twisting force (Chopart). |
| Clinical Features | Marked hindfoot deformity, often in valgus (medial) or varus (lateral). Talus remains aligned with tibia. Talar head palpable medially (medial type). | Gross ankle deformity, severe swelling. Foot often appears externally/internally rotated relative to leg. | Less obvious global foot deformity than subtalar/ankle dislocation. Pain focused over medial midfoot. Palpable gap or prominence. | Forefoot abduction/pronation (Lisfranc). Midfoot swelling, tenderness, potential plantar ecchymosis (Lisfranc sign). Inability to bear weight. |
| X-ray Findings | Tibiotalar articulation intact . Talus dislocated from calcaneus and navicular. Directional displacement (medial, lateral, etc.) of calcaneus/foot block relative to talus. | Complete loss of tibiotalar congruity. Talus displaced relative to tibia. Often associated malleolar or plafond fractures. | Talus remains aligned with calcaneus (subtalar joint intact). Navicular displaced from talar head. | Lateral displacement of metatarsal bases from cuneiforms (Lisfranc). Disruption of talonavicular and calcaneocuboid joints (Chopart). |
| CT/MRI Role | Essential for identifying associated fractures (talus, calcaneus, navicular), articular damage, incarcerated fragments. Post-reduction verification. | Essential to characterize fracture patterns (pilon, malleolar), assess articular congruity, and identify incarcerated fragments. | Confirm isolated dislocation, rule out associated subtle fractures or soft tissue interposition. | CT is gold standard for Lisfranc to assess articular damage, subtle diastasis, and small avulsion fractures. MRI for ligamentous injury if CT equivocal. |
| Treatment Principles | Urgent closed reduction under adequate anesthesia. Post-reduction CT. Immobilization for 4-6 weeks. ORIF for irreducible cases, open dislocations, or unstable associated fractures. | Urgent closed reduction. Often requires ORIF due to associated fractures or instability. Ex-fix may be used acutely for unstable injuries. | Closed reduction. Immobilization. ORIF if irreducible or unstable. | Urgent closed reduction. ORIF for unstable Lisfranc injuries. Immobilization for Chopart. |
Surgical Decision Making & Classification
The decision-making process for subtalar dislocations hinges on several critical factors, primarily focused on the urgency of reduction and subsequent stability.
Why Operative vs. Non-Operative?
Non-Operative (Closed Reduction):
This is the
primary treatment modality
for the vast majority (over 80%) of subtalar dislocations.
*
Indication:
Closed subtalar dislocations without significant neurovascular compromise or severe skin compromise, and without unstable associated fractures or incarcerated fragments that prevent concentric reduction.
*
Rationale:
Prompt reduction minimizes soft tissue tension, reduces the risk of skin necrosis, preserves neurovascular integrity, and improves long-term functional outcomes by restoring joint alignment. The inherent stability of the subtalar joint once reduced, due to its complex ligamentous attachments (e.g., interosseous talocalcaneal ligament, cervical ligament), often precludes the need for internal fixation in isolated injuries.
Operative (Open Reduction Internal Fixation - ORIF):
This approach is reserved for specific indications.
*
Indications:
1.
Open Subtalar Dislocation:
Mandates debridement and open reduction to address contamination and allow for thorough assessment of soft tissue and bony structures.
2.
Irreducible Closed Dislocation:
If closed reduction attempts fail despite adequate anesthesia and muscle relaxation. This typically suggests soft tissue interposition (e.g., extensor digitorum brevis, tibialis posterior tendon, flexor hallucis longus, joint capsule, or neurovascular bundle) or incarcerated osteochondral fragments.
3.
Associated Unstable Fractures:
Such as displaced talar neck fractures, significant calcaneal fractures, or large osteochondral fragments that require fixation to restore joint congruity and stability.
4.
Significant Neurovascular Compromise:
Although rare, if pulses or neurological function are compromised following reduction attempts, an open approach may be necessary to decompress or repair structures.
5.
Severe Skin Compromise:
While prompt closed reduction is usually the first step, in cases of severe skin tenting, a delay in reduction can lead to skin necrosis, which might necessitate surgical debridement and formal open reduction.
In our patient's case, the presence of a closed dislocation with rapidly worsening skin tension indicated an urgent need for closed reduction. The associated minor avulsion fractures were not considered unstable or significant enough to impede reduction or necessitate primary ORIF.
Classification
Subtalar dislocations are typically classified based on the direction of displacement of the foot (and calcaneus) relative to the talus, which remains congruently articulated with the tibia. The most widely accepted classifications include:
-
Close and Inman Classification (most common):
- Medial Dislocation (Inward): The most frequent type (80-85%). The foot and calcaneus are displaced medially, with the talar head dislocating medially from the navicular. The talar head is often palpable on the medial aspect of the ankle. This type results from a violent supination and plantarflexion force or an axial load with pronation-eversion. Our patient presented with a medial subtalar dislocation.
- Lateral Dislocation (Outward): Less common (15-20%). The foot and calcaneus are displaced laterally, and the talar head dislocates laterally from the navicular. The talar head may be palpable laterally, or the lateral malleolus may be prominent due to medial displacement of the talus relative to the calcaneus. This typically occurs from a severe pronation-dorsiflexion or an axial load with supination-inversion mechanism.
- Anterior Dislocation: Very rare. The foot and calcaneus are displaced anteriorly relative to the talus.
- Posterior Dislocation: Extremely rare. The foot and calcaneus are displaced posteriorly relative to the talus.
-
Broca Classification: Historically categorized based on integrity of soft tissues (pure dislocation vs. dislocation with fracture). Less used in acute trauma.
-
Mears and Shocher Classification: Incorporates associated fractures.
- Type I: Pure dislocation.
- Type II: Dislocation with associated minor fractures (e.g., avulsions).
- Type III: Dislocation with major associated fractures (e.g., talar neck fracture).
For our patient, the classification was a Close and Inman Type I Medial Subtalar Dislocation with minor associated fractures (Mears and Shocher Type II). This classification guided the urgent decision for closed reduction.
Surgical Technique / Intervention
The primary intervention for a closed subtalar dislocation is prompt closed reduction under adequate anesthesia.
Pre-operative Preparation
- Analgesia: Intravenous opioids were administered immediately upon presentation.
- Anesthesia: Given the significant muscle spasm and pain, a procedural sedation (e.g., ketamine, propofol) or a regional block (e.g., ankle block or popliteal block) combined with conscious sedation was utilized. In cases of severe muscular guarding or failed initial attempts, general anesthesia may be required for optimal muscle relaxation. Our patient underwent closed reduction in the Emergency Department under propofol sedation administered by an anesthetist.
- Consent: Informed consent was obtained, detailing the procedure, risks (e.g., failed reduction, skin necrosis, neurovascular injury, post-traumatic arthritis, avascular necrosis, stiffness, chronic instability), and potential need for open reduction.
- Antibiotics: Prophylactic antibiotics (e.g., Cefazolin) were administered due to the high-energy nature of the injury and potential for occult soft tissue damage, even in a closed injury.
- Positioning: The patient was positioned supine on the gurney. The leg was flexed at the knee to relax the gastrocnemius-soleus complex, which can hinder reduction.
Reduction Techniques (for Medial Subtalar Dislocation)
The key to successful reduction lies in reversing the mechanism of injury and overcoming the deforming forces exerted by the strong ligaments and muscle groups.
- Traction: Strong, sustained longitudinal traction is applied to the forefoot and hindfoot by an assistant, while counter-traction is applied to the proximal tibia by another assistant or via a thigh-holding device. This helps to disengage the talar head from its abnormal position and relax the surrounding soft tissues.
- Dorsiflexion & Plantarflexion: While maintaining traction, the foot is gently brought into slight plantarflexion, and then gradually dorsiflexed to disengage the talar head.
-
Maneuver to Address Displacement:
-
For Medial Subtalar Dislocation (like our patient):
- The primary surgeon applies direct pressure over the displaced talar head (medially) to push it laterally, while simultaneously inverting and then everting the calcaneus.
- The foot (calcaneus and midfoot) needs to be brought from its displaced medial position laterally. This usually involves exaggerating the deformity (supination/inversion) to clear any bony impingement, followed by a reversal of the deformity (pronation/eversion) while applying firm thumb pressure on the medial aspect of the talar head and longitudinal traction.
- The maneuver can be summarized as: Exaggerate the deforming force (supination/inversion if medial dislocation), then distract the foot, and finally pronate/evert the foot into anatomical alignment while simultaneously pushing the talar head laterally into its socket.
-
For Lateral Subtalar Dislocation:
- The foot (calcaneus and midfoot) needs to be brought from its displaced lateral position medially. This involves exaggerating the deformity (pronation/eversion), then distracting, and finally supinating/inverting the foot into anatomical alignment while pushing the talar head medially.
-
For Medial Subtalar Dislocation (like our patient):
Successful reduction is often marked by a palpable and audible "clunk" or "pop." Immediate relief of soft tissue tension and improved appearance of the foot are observed.
Post-Reduction Assessment
- Clinical: Reassess neurovascular status immediately. Palpate for pulses, check capillary refill and sensation. Inspect skin for blanching or new tenting.
- Stability: Gently assess the stability of the subtalar joint. Excessive laxity might suggest significant ligamentous disruption requiring further consideration (though rare).
- Radiographs: Post-reduction plain radiographs (AP, lateral, oblique) are mandatory to confirm concentric reduction of the talonavicular and talocalcaneal joints and to rule out any gross residual displacement.
-
Post-Reduction CT Scan:
This is
crucial
to:
- Confirm precise anatomical reduction.
- Rule out incarceration of soft tissues (e.g., tendons, capsule) or osteochondral fragments within the joint space that were not visible on plain radiographs and could lead to painful range of motion or early arthritis.
- Identify any occult fractures or assess the displacement of previously identified minor fractures.
In our patient's case, closed reduction was successfully achieved on the first attempt under propofol sedation. A clear "clunk" was felt, and the foot immediately regained a more anatomical contour. Post-reduction radiographs confirmed satisfactory alignment. A subsequent CT scan confirmed concentric reduction of the subtalar and talonavicular joints, with no incarcerated fragments. The previously noted minor talar posterior process fracture and calcaneal avulsion remained undisplaced and non-articular.
Fixation Construct
For most isolated, stable subtalar dislocations reduced closed, internal fixation is not required . The robust ligamentous structures of the subtalar joint, particularly the interosseous talocalcaneal ligament and the cervical ligament, provide inherent stability once the joint is reduced.
- Temporary K-wire Fixation: May be considered if the reduction is stable but there is concern for early redislocation during the immediate post-reduction period, or if there is excessive laxity due to severe capsuloligamentous injury. This is rare and typically not necessary.
- ORIF for Associated Fractures: If an open reduction was required or if significant associated fractures (e.g., displaced talar neck fracture) were present, then appropriate internal fixation (screws, plates) would be used to stabilize these fractures.
Our patient did not require internal fixation after successful closed reduction.
Post-Operative Protocol & Rehabilitation
The post-operative (or post-reduction) protocol for subtalar dislocations focuses on protecting the joint, managing pain and swelling, and gradually restoring motion and strength.
Phase 1: Immobilization and Protection (Weeks 0-6)
-
Immobilization:
- Immediately post-reduction, the foot was placed in a well-padded short leg plaster backslab in a neutral position to accommodate swelling.
- Once swelling subsided (typically within 3-5 days), the backslab was converted to a short leg non-weight-bearing cast (either plaster or fiberglass). The cast provides rigid immobilization of the subtalar and talonavicular joints while allowing for some ankle dorsi/plantarflexion.
- The position of the foot in the cast should be neutral or slightly dorsiflexed to prevent equinus contracture. The cast should extend from just below the fibular head to the metatarsal heads.
- Weight-bearing Status: Strictly non-weight-bearing (NWB) for the entire 6-week period. The patient was instructed to use crutches or a knee scooter.
- Edema Management: Elevation of the extremity above heart level, regular ice application (over the cast if possible), and non-steroidal anti-inflammatory drugs (NSAIDs) or other analgesics as needed.
- Neurovascular Monitoring: Regular checks, especially in the first few days, for any signs of neurovascular compromise or pressure sores from the cast.
- Deep Vein Thrombosis (DVT) Prophylaxis: Given the NWB status and immobilization, chemical DVT prophylaxis (e.g., low molecular weight heparin) was initiated, especially for patients with additional risk factors.
- Radiographic Follow-up: At 1-2 weeks and 4-6 weeks to ensure maintenance of reduction.
Phase 2: Controlled Mobilization and Early Strengthening (Weeks 6-12)
- Cast Removal: At approximately 6 weeks, the short leg cast was removed.
- Weight-bearing Status: Transition to a removable ankle-foot orthosis (AFO) or walking boot . Gradual progression to partial weight-bearing (PWB) , advancing to full weight-bearing (FWB) as tolerated over the next 2-4 weeks, depending on pain and radiographic healing (if associated fractures were present). Crutches were used initially for support.
-
Rehabilitation Focus:
- Range of Motion (ROM): Initiation of gentle, active and passive range of motion exercises for the ankle and subtalar joints. Emphasis on restoring dorsiflexion, plantarflexion, inversion, and eversion. Stretching exercises for the Achilles tendon.
- Strengthening: Isometric exercises initially, progressing to resistance band exercises for all ankle and foot muscle groups (dorsiflexors, plantarflexors, invertors, evertors).
- Proprioception: Single-leg standing exercises (initially with support), wobble board exercises, and balance activities to restore neuromuscular control.
- Pain Management: Continued as needed.
Phase 3: Advanced Strengthening and Return to Activity (Weeks 12 onwards)
- Weight-bearing Status: Full weight-bearing without support.
-
Rehabilitation Focus:
- Progressive Strengthening: Increase resistance and intensity of exercises. Incorporate functional exercises relevant to the patient's activities (e.g., walking on uneven surfaces, stair climbing, light jogging).
- Plyometrics and Agility: For active individuals, specific drills to improve power, agility, and dynamic stability, if appropriate.
- Sport-Specific Training: Gradual return to sports-specific activities, ensuring adequate strength, stability, and pain-free motion.
- Long-Term Follow-up: Continued monitoring for complications such as post-traumatic arthritis, chronic pain, stiffness, or instability. Orthotics or ankle braces may be considered for patients with persistent instability or for return to high-impact activities.
Our patient followed this protocol diligently. At 6 weeks, radiographs showed stable reduction and he transitioned to a walking boot with a gradual return to weight-bearing. By 12 weeks, he had excellent range of motion, minimal pain, and was progressing well with strengthening and balance exercises. He was cleared to gradually return to light work activities by 4 months post-injury.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Urgency of Reduction: Subtalar dislocations, especially with skin tenting, are orthopaedic emergencies. Prompt reduction (within hours) is paramount to prevent skin necrosis, minimize soft tissue swelling, and reduce the risk of neurovascular compromise and avascular necrosis of the talus.
- Adequate Anesthesia: Never attempt reduction without sufficient analgesia and muscle relaxation . Inadequate anesthesia leads to failed attempts, increased patient distress, and further soft tissue damage. Procedural sedation or regional blocks are often sufficient; general anesthesia may be required.
- Comprehensive Neurovascular Assessment: Always document the neurovascular status pre- and post-reduction . This is a non-negotiable step.
- Post-Reduction Imaging: While radiographs confirm gross reduction, a post-reduction CT scan is essential . It is the gold standard for confirming concentric reduction, ruling out incarcerated fragments (e.g., osteochondral pieces, tibialis posterior tendon, extensor digitorum brevis) that can block reduction or lead to chronic pain and arthritis, and identifying subtle associated fractures.
- Exaggerate Deformity then Reverse: The key reduction maneuver often involves exaggerating the primary deformity (e.g., supination/inversion for medial dislocation) to unlock the talus, followed by firm traction and a reversal of the deforming forces.
- Associated Injuries: Always be vigilant for associated injuries. While the tibiotalar joint is typically intact, concomitant ankle or midfoot fractures (especially talar neck/body, calcaneus, navicular) are common. A high-energy mechanism warrants a thorough trauma survey.
- Soft Tissue Envelope: Pay close attention to the soft tissue envelope. Severe tension, skin dimpling, or an open injury drastically changes management. Open injuries require formal surgical debridement and reduction.
Pitfalls
- Delayed Reduction: Prolonged delay in reduction can lead to irreversible skin necrosis, compartment syndrome (though rare in subtalar dislocations), and increased difficulty of reduction due to edema and muscle spasm. This significantly worsens prognosis.
- Inadequate Reduction: Failure to achieve or confirm true anatomical reduction. A seemingly reduced joint on plain films might still have subtle subluxation or incarcerated fragments, leading to chronic pain, stiffness, and early post-traumatic arthritis. This is why post-reduction CT is critical.
- Missed Associated Fractures: Overlooking subtle fractures (e.g., talar dome, sustentaculum tali, navicular avulsion) on plain radiographs. These can be better identified with CT and, if unstable, may require specific management.
- Avascular Necrosis (AVN) of the Talus: Although subtalar dislocations involve the talocalcaneal and talonavicular joints, the high-energy mechanism can disrupt the vascular supply to the talus, particularly the talar neck and body. While less common than with talar neck fractures, AVN remains a significant long-term complication, leading to collapse and arthritis.
- Post-Traumatic Arthritis: This is the most common long-term complication, particularly if there was significant articular cartilage damage at the time of injury or if anatomical reduction was not achieved or maintained. Patients should be counseled about this risk.
- Chronic Stiffness and Instability: Inadequate rehabilitation, prolonged immobilization, or extensive capsuloligamentous injury can lead to chronic stiffness (especially reduced subtalar motion) and/or persistent instability, requiring further intervention.
- Ignoring the Talus-Navicular Joint: Ensure both the talocalcaneal and talonavicular joints are reduced and congruent. Failure to address both components of the subtalar complex leads to persistent deformity and pain.
This case highlights the principles of emergent orthopedic trauma management, emphasizing the critical interplay of rapid diagnosis, effective reduction techniques, and vigilant post-reduction assessment to optimize patient outcomes.
