Introduction & Epidemiology
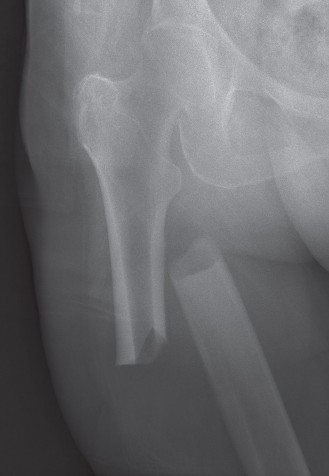
Subtrochanteric femur fractures, often referred to as the "silent threat" due to their challenging nature and potential for significant morbidity and mortality, represent a distinct and complex subset of proximal femoral injuries. Defined anatomically as fractures occurring within the region extending from the lesser trochanter distally approximately 5 cm along the femoral shaft, these injuries are characterized by their location in a highly stressed segment of bone, surrounded by powerful musculature. This unique anatomical and biomechanical environment predisposes them to high rates of comminution, displacement, and persistent deforming forces, making their management a formidable task for the orthopedic surgeon.
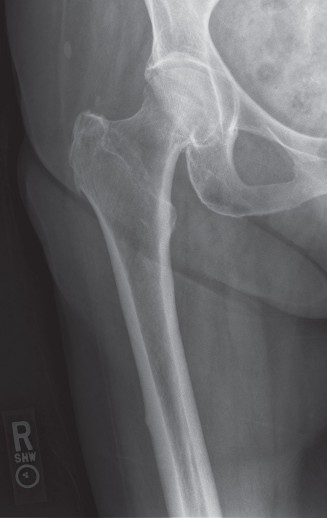
Epidemiologically, subtrochanteric fractures exhibit a bimodal distribution. In younger, active individuals, they typically result from high-energy trauma, such as motor vehicle collisions or falls from significant heights. These fractures are often severe, comminuted, and may be associated with polytrauma, requiring meticulous assessment for concomitant injuries. In contrast, the majority of subtrochanteric fractures are observed in the elderly population, frequently as a result of low-energy falls in patients with underlying osteoporosis or other metabolic bone diseases. This demographic often presents with multiple medical comorbidities, complicating both surgical and anesthetic management. A notable and increasingly recognized subset in this older population comprises atypical femoral fractures (AFFs), often associated with prolonged bisphosphonate use, which present with characteristic radiographic features and unique healing challenges.
The management of subtrochanteric femur fractures is primarily surgical, driven by the inherent instability and the significant deforming muscular forces that lead to high rates of nonunion and malunion if treated non-operatively. The proximity to the hip joint, the high mechanical loads experienced by the proximal femur, and the complex three-dimensional displacement patterns necessitate robust internal fixation to facilitate early mobilization and minimize the systemic complications associated with prolonged recumbency in an often frail patient cohort. Understanding the specific biomechanical challenges and nuances of surgical technique is paramount for achieving optimal patient outcomes and mitigating the high-impact consequences of these injuries.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the subtrochanteric region is fundamental to the successful management of these challenging fractures. The subtrochanteric region is a critical transition zone between the cancellous bone of the proximal femur and the cortical bone of the diaphysis, characterized by a complex interplay of muscular attachments and a highly stressed load-bearing environment.
Anatomical Considerations
The subtrochanteric zone is classically defined as the segment of the femur extending from the inferior border of the lesser trochanter distally for approximately 5 cm. This area is distinguished by its dense cortical bone, particularly along the linea aspera, providing significant structural integrity. However, it is also a region of high stress concentration, making it vulnerable to fracture under both traumatic and cyclic loading.
- Cortical Thickness and Medullary Canal: The cortex in the subtrochanteric region is among the thickest in the entire femur, contributing to its strength but also presenting challenges for reaming and nail insertion. The medullary canal begins to narrow significantly in this zone, transitioning from the broad metaphyseal canal to the narrower diaphyseal canal. This funnel-like geometry can create stress risers and complicate nail passage.
- Vascular Supply: The proximal femur receives its blood supply from several sources, primarily the medial and lateral circumflex femoral arteries, which form an extracapsular ring. Branches from this ring supply the trochanteric region and the femoral neck. The nutrient artery, typically a branch of the profunda femoris artery, enters the femur distally to the lesser trochanter. While the subtrochanteric region itself has a robust blood supply, extensive soft tissue stripping during open reduction can compromise periosteal circulation, potentially impairing fracture healing.
-
Muscular Attachments and Deforming Forces:
The powerful musculature surrounding the proximal femur exerts significant deforming forces on fracture fragments, which are a hallmark challenge of subtrochanteric injuries.
- Proximal Fragment: The iliopsoas muscle inserts onto the lesser trochanter, causing flexion of the proximal fragment. The gluteus medius and minimus insert onto the greater trochanter, inducing abduction. The external rotators (piriformis, obturators, gemelli, quadratus femoris) also contribute to external rotation of the proximal segment.
- Distal Fragment: The adductor muscles (adductor longus, brevis, magnus) and vastus lateralis exert an adduction force, while the hamstring muscles and gastrocnemius can cause shortening and posterior displacement of the distal fragment.
- The net effect of these opposing forces is often a characteristic deformity: flexion, abduction, and external rotation of the proximal fragment, with adduction and shortening of the distal fragment. This complex three-dimensional displacement makes closed reduction difficult and often necessitates meticulous surgical maneuvers.
Biomechanical Considerations
The subtrochanteric region is subjected to substantial biomechanical loads, particularly high bending and torsional stresses during weight-bearing and activities of daily living. It acts as a long lever arm, transmitting forces from the hip to the knee.
- Stress Concentration: The change in femoral geometry from the broad proximal metaphysis to the narrower diaphysis creates a stress concentration zone in the subtrochanteric region. This is further exacerbated by the varying cortical thickness and the anatomical curvature of the femur.
- Cantilever Bending: The femur functions largely as a cantilever beam during single-leg stance, with the hip joint acting as the fulcrum. This results in significant bending moments across the subtrochanteric region, placing the lateral cortex under tension and the medial cortex under compression.
- Torsional Forces: Rotational movements of the trunk or limb translate into substantial torsional forces across the femur, which are particularly concentrated at the junction of the wider metaphysis and narrower diaphysis.
- Impact of Comminution: Subtrochanteric fractures are frequently comminuted, especially medially. Loss of medial cortical support significantly increases the load on the implant, contributing to implant fatigue and failure if not adequately supported biomechanically. The restoration of medial cortical contact, either directly or indirectly, is critical for load sharing and long-term implant survival.
Understanding these anatomical and biomechanical principles guides surgical decision-making, emphasizing the need for robust implants capable of neutralizing these powerful forces and achieving stable fixation to promote healing.
Indications & Contraindications
The management of subtrochanteric femur fractures is overwhelmingly operative due to the inherent instability of these injuries and the high risk of nonunion or malunion with non-surgical approaches. The powerful deforming muscle forces invariably lead to unacceptable displacement and functional deficits if not surgically stabilized.
Indications for Operative Management
Nearly all subtrochanteric femur fractures warrant surgical fixation. The primary goals of surgery are to:
* Achieve stable anatomical reduction.
* Allow for early mobilization and rehabilitation.
* Minimize pain and long-term disability.
* Prevent complications such as nonunion, malunion, and systemic morbidity associated with prolonged bed rest.
Specific indications include:
*
All displaced or unstable subtrochanteric fractures:
This encompasses the vast majority of these injuries.
*
Pathological fractures:
Often requiring biopsy and stabilization.
*
Impending pathological fractures:
Identified through imaging (e.g., bone scans, MRI) in patients with known malignancy or other bone pathologies. Prophylactic fixation is indicated when cortical involvement exceeds 50% or pain is significant, preventing fracture.
*
Atypical femoral fractures (AFFs):
Often bilateral, these stress fractures associated with bisphosphonate use are inherently unstable and have a high risk of complete fracture if not surgically stabilized. Prophylactic nailing of the contralateral femur is often considered if radiographic signs of an impending AFF are present.
*
Polytrauma patients:
Early stabilization of femur fractures is crucial for damage control orthopedics, reducing systemic inflammatory response and improving outcomes.
Contraindications for Operative Management
Absolute contraindications to surgical intervention are rare and generally relate to the patient's overall physiological status rather than the fracture pattern itself.
*
Medically unstable patient:
A patient with severe, uncorrectable medical comorbidities (e.g., severe sepsis, decompensated cardiac failure) where the risks of anesthesia and surgery outweigh the benefits of fracture fixation. Such cases require medical stabilization, potentially followed by delayed surgery, or palliation.
*
Active infection at the surgical site:
Requires control of the infection prior to definitive fixation.
*
Severe uncontrolled coagulopathy:
Should be corrected prior to surgery.
Relative contraindications may include:
* Non-ambulatory patient with minimal pain and a stable, undisplaced fracture where the risk of surgery is deemed higher than the benefit of functional restoration. This is an exceedingly rare scenario for subtrochanteric fractures.
Summary Table: Operative vs. Non-Operative Indications
| Feature | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | All displaced fractures | Extremely rare, possibly select non-ambulatory patients with undisplaced fractures |
| Fracture Stability | All unstable fractures (high comminution, deforming forces) | Extremely rare, only truly stable and undisplaced fractures |
| Patient Status | Medically optimized for surgery, polytrauma requiring early stabilization, pathological/impending pathological | Medically unstable, severe comorbidities precluding safe anesthesia/surgery |
| Associated Conditions | Atypical femoral fractures (AFFs), concomitant injuries requiring early mobilization | None specific, typically reserved for palliative care in select scenarios |
| Expected Outcome | Early mobilization, anatomical reduction, reduced risk of nonunion/malunion, improved functional recovery | High risk of nonunion/malunion, significant shortening, angular deformity, prolonged bed rest, systemic complications |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing surgical outcomes and minimizing complications in subtrochanteric femur fracture fixation.
Pre-Operative Planning
-
Patient Assessment and Medical Optimization:
- A comprehensive medical evaluation is paramount, especially in elderly patients with comorbidities. This includes cardiovascular, pulmonary, renal, and neurological assessments.
- Correction of anemia, electrolyte imbalances, and coagulopathies.
- Nutritional assessment and optimization.
- Review of medications, particularly anticoagulants and antiplatelet agents.
- Pain management strategy.
-
Imaging Review and Fracture Classification:
- Radiographs: Anteroposterior (AP) and lateral views of the entire femur, including the hip and knee joints, are essential. Contralateral hip imaging can be useful for templating.
- Computed Tomography (CT) Scan: Highly recommended, especially for comminuted fractures, to fully delineate fracture patterns, assess medial comminution, and identify potential issues with nail entry or length. 3D reconstructions can be invaluable.
-
Classification:
- Seinsheimer Classification: Based on the number and location of fracture fragments at the lesser trochanter. Useful for understanding proximal fragment stability.
- Russell-Taylor Classification: Differentiates between fractures extending into the piriformis fossa (Type I) or not (Type II), with further subdivisions based on greater trochanteric involvement. Influences nail entry point.
- AO/OTA Classification: Comprehensive, universally accepted system (32-A/B/C) providing detailed information on fracture morphology.
- Atypical Femoral Fractures (AFFs): Recognize characteristic features (lateral cortical thickening, transverse or short oblique pattern, minimal comminution, often bilateral).
-
Implant Selection and Templating:
-
Intramedullary Nailing (IMN):
Considered the gold standard for most subtrochanteric fractures.
- Nail Type: Reamed vs. unreamed (reamed provides better cortical contact, stronger construct). Standard vs. trochanteric entry (trochanteric entry is preferred to avoid piriformis fossa osteonecrosis and ease of entry). Long vs. short nail (long nails spanning the entire femoral shaft are generally preferred for distal fractures or comminution to protect the entire diaphysis).
- Nail Diameter and Length: Templating with contralateral hip films helps estimate nail length and diameter. The nail should ideally extend to within 1-2 cm of the epiphyseal plate of the distal femur.
- Locking Options: Number and orientation of proximal and distal locking screws. Multi-planar locking is desirable.
- Plating: Less common for primary fixation but may be indicated for certain fracture patterns (e.g., extremely wide medullary canals unsuitable for nailing, fractures extending too far proximally into the femoral neck where an IMN would compromise reduction, reverse obliquity patterns that can be unstable with IMN). Examples include Less Invasive Stabilization System (LISS) or Locking Compression Plates (LCP).
- Ancillary Fixation: Blocking screws, cerclage wires (used judiciously to prevent soft tissue stripping), or external fixators for temporary stabilization/reduction aids.
-
Intramedullary Nailing (IMN):
Considered the gold standard for most subtrochanteric fractures.
-
Surgical Team and Equipment:
- Ensure availability of appropriate implants, instruments (large reduction clamps, bone holders, traction devices), and C-arm fluoroscopy.
- Experienced surgical team, including an orthopedic trauma surgeon, assistants, and anesthesia.
Patient Positioning
The choice of patient positioning depends on the surgical approach and the preference of the surgeon.
*
Supine Position on a Fracture Table:
*
Advantages:
Provides continuous longitudinal traction, which can aid in reduction of length and alignment. The contralateral limb can be flexed and abducted for C-arm access.
*
Disadvantages:
Can make rotational control challenging. Access to the hip for direct manipulation of the proximal fragment may be limited. Obese patients may be difficult to position.
*
Setup:
Patient supine with the pelvis secured. The affected leg is placed in a traction boot or skeletal traction. The contralateral leg is often placed in a well-padded knee flexor attachment to allow for C-arm imaging of the injured hip. Ensure adequate padding at all pressure points.
-
Supine Position on a Radiolucent Operating Table (Free-Draping):
- Advantages: Allows for greater freedom in hip positioning (flexion, adduction, abduction, rotation) which can be crucial for achieving reduction, especially of the proximal fragment. Easier access for manual manipulation and adjunctive techniques.
- Disadvantages: Requires an assistant to maintain traction and support the limb. Risk of rotational malalignment if not carefully monitored.
- Setup: Patient supine, with the affected limb free-draped. The hip and knee can be gently flexed to relax muscle tension. The C-arm can be brought in from the contralateral side for AP views and from the caudal aspect for lateral views.
Regardless of the positioning method, key considerations include:
*
C-arm Access:
Ensure unrestricted intra-operative fluoroscopic imaging in multiple planes (AP and lateral) of the entire fracture and planned implant trajectory.
*
Padding:
Meticulous padding of all pressure points to prevent nerve palsies (e.g., peroneal nerve at the fibular head, ulnar nerve at the elbow) and skin breakdown.
*
Sterile Field:
Prepare a wide sterile field to allow for potential extension of the approach or additional access points.
*
Pre-reduction:
Gentle traction in the emergency department can sometimes improve initial alignment and facilitate positioning.
Detailed Surgical Approach / Technique
Intramedullary nailing (IMN) is the preferred method for the vast majority of subtrochanteric femur fractures due to its biomechanical advantages, load-sharing properties, and less invasive nature compared to plating. Plate fixation remains an option for specific fracture patterns.
Intramedullary Nailing (IMN)
The general principles involve achieving an acceptable reduction, preparing the medullary canal, inserting the nail, and securing it with proximal and distal locking screws.
-
Preparation and Draping:
- Patient positioned as planned (fracture table or radiolucent table).
- A wide surgical field is prepared and draped to allow for optimal C-arm access and potential need for an open reduction.
-
Incision and Entry Point:
- Skin Incision: A longitudinal incision is made over the tip of the greater trochanter, typically 3-5 cm in length, centered at the trochanteric tip.
- Deep Dissection: Dissect through subcutaneous tissue and fascia lata. Split the gluteus medius fibers longitudinally in line with its fibers and the underlying vastus lateralis.
- Entry Point: The ideal entry point for most modern trochanteric entry nails is at or slightly medial to the tip of the greater trochanter, in line with the femoral canal. This helps avoid iatrogenic piriformis fossa avascular necrosis (AVN) which can occur with a more medial entry. Fluoroscopic guidance is essential to confirm the guidewire's position in the center of the medullary canal in both AP and lateral views. An awl or cannulated starting reamer is used to create the cortical opening.
-
Reduction:
- This is often the most challenging step due to the powerful deforming muscle forces.
- Longitudinal Traction: Applied manually or via a fracture table.
-
Addressing Proximal Fragment Deformity:
- Flexion: The proximal fragment is often flexed by the iliopsoas. This can be counteracted by increasing hip flexion (if on a radiolucent table), placing a bolster under the buttock, or using a femoral distractor.
- Abduction/External Rotation: Reduced by adducting and internally rotating the entire limb. A large Schanz pin placed in the proximal fragment and used as a joystick can also aid in reduction.
-
Indirect Reduction Techniques:
- Blocking Screws (Poller Screws): Placed in the metaphysis adjacent to the nail path (usually medial and/or anterior) to guide the nail into the desired alignment and prevent uncontrolled angulation during nail insertion.
- External Fixator: A temporary external fixator can provide powerful reduction capabilities, particularly for length and rotation.
- Cerclage Wires: May be used cautiously for highly comminuted patterns, but require open exposure and can compromise periosteal blood supply.
- Direct Reduction Techniques (Open Reduction): If closed reduction is unsuccessful, a limited lateral approach can be used to directly visualize and reduce the fracture. Large reduction clamps (e.g., point reduction clamp, Verbrugge clamp) or bone hooks can be employed. Minimize soft tissue stripping to preserve biology.
-
Reaming and Nail Insertion:
- Guidewire Insertion: Advance a ball-tipped guidewire past the fracture site into the distal femoral canal. Ensure it is centrally located in both AP and lateral views.
- Reaming: Serially ream the medullary canal, typically 1.5-2 mm larger than the chosen nail diameter. Reaming should be performed slowly and progressively to minimize heat necrosis and fat embolization. In fractures with significant comminution or those requiring high stability, slight over-reaming can allow for a larger diameter nail and improved cortical contact.
- Nail Insertion: Advance the chosen intramedullary nail over the guidewire. Gentle rotation and impaction may be necessary. Ensure the nail passes the fracture site without significant resistance or iatrogenic comminution. The nail should be inserted to the templated depth, ensuring adequate length for distal locking and optimal proximal fit.
-
Proximal Locking:
- Utilize a targeting guide for accurate screw placement.
- Typically, two screws are placed in the proximal fragment: one anterior-posterior and one medial-lateral. These provide rotational stability and prevent proximal fragment migration.
- Confirm screw position and length with fluoroscopy to ensure they are fully within the bone and do not protrude excessively.
-
Distal Locking:
- Fluoroscopic freehand technique or a targeting guide can be used.
- Often, two distal locking screws are sufficient to prevent shortening and rotation.
- Dynamic locking (slot) may be considered if some controlled collapse is desired, but static locking (round hole) is generally preferred for subtrochanteric fractures to provide maximal stability.
- Confirm screw position and length.
-
Final Checks:
- Obtain AP and lateral fluoroscopic views of the entire femur to confirm fracture reduction, nail position, and screw placement.
- Assess limb length and rotation clinically.
- Remove all guidewires and instruments. Close the incision in layers.
Plate Fixation
While less common, plate fixation (e.g., LCP, LISS) can be indicated for specific subtrochanteric fracture patterns:
* Fractures with significant comminution extending into the piriformis fossa or femoral neck, making IMN entry or proximal fixation challenging.
* Extremely wide medullary canals where an IMN would not provide adequate fill.
* Reverse obliquity fractures (AO/OTA 32-A3.3) where IMN may be biomechanically less stable against medialization of the distal fragment.
* Failed IMN.
- Approach: Standard lateral approach to the proximal femur, splitting the vastus lateralis muscle to expose the fracture site. Minimize periosteal stripping.
- Reduction: Open reduction often necessary. Use of temporary clamps, cerclage wires (if needed), or external fixators to achieve length, alignment, and rotation. Aim for indirect reduction techniques where possible to preserve biology.
-
Plate Application:
A long, broad, anatomically contoured locking plate is chosen (e.g., 10-14 holes). The plate is applied to the lateral cortex, spanning the fracture with adequate screws proximally and distally.
- Biplanar fixation: Consider screws in multiple planes (e.g., anterior-posterior in addition to medial-lateral) in the proximal fragment for enhanced stability.
- Working length: Ensure sufficient space between proximal and distal screw clusters over the fracture zone to allow for micro-motion and callus formation.
- Lag screws: May be used through the plate to compress specific fragments, if applicable.
- Bone Grafting: Consider autologous or allograft bone grafting for significant bone defects or anticipated delayed union.
Special Considerations for Atypical Femoral Fractures (AFFs)
- Prophylactic Nailing: In patients with prodromal pain or incomplete AFFs, prophylactic intramedullary nailing of the affected femur is recommended. Nailing of the contralateral femur may also be considered due to the high bilaterality.
- Healing: AFFs are associated with delayed healing. Consider adjuvant measures like bone grafting or biological augmentation. Discontinuation of bisphosphonates (if possible) is usually recommended.
Complications & Management
Subtrochanteric femur fractures are associated with a relatively high rate of complications due to their complex biomechanics, the often comminuted nature of the injury, and the patient demographics. Prompt recognition and appropriate management are crucial for salvage and optimizing patient outcomes.
Common Complications and Management Strategies
| Complication | Incidence | Etiology | Salvage Strategies / Management |
|---|---|---|---|
| Nonunion | 5-15% (can be higher in complex fractures, AFFs, or poor technique) | Inadequate reduction, unstable fixation, poor biology (excessive stripping, infection), delayed weight-bearing, metabolic factors, bisphosphonate use (AFFs) | Hypertrophic nonunion: Stable construct but no healing. Requires revision IMN (larger diameter nail, exchange nailing), potentially with bone grafting (autograft/allograft). Atrophic nonunion: Unstable construct, poor biology. Requires stable revision fixation (exchange nailing, plate osteosynthesis) with vigorous bone grafting (autograft). |
| Malunion | 10-25% (especially rotational and varus) | Inadequate reduction during surgery, unstable fixation, early unrestricted weight-bearing, failure to recognize deforming forces | Symptomatic varus/shortening/rotational malunion: Corrective osteotomy (proximal femoral osteotomy) with stable internal fixation (plate or IMN). Asymptomatic malunion: Conservative management, gait training, shoe lift for shortening. |
| Infection | 1-5% (deep), higher in open fractures or prolonged surgeries | Contamination, extensive soft tissue dissection, compromised host immunity | Acute: Surgical debridement, thorough irrigation, intravenous antibiotics (culture-directed). Chronic: Hardware removal (if fracture healed), extensive debridement, prolonged antibiotics, potential soft tissue coverage. May require re-fixation in a second stage. |
| Hardware Failure | 5-10% (nail breakage, screw pullout) | Inadequate reduction (especially medial comminution), poor bone quality, premature full weight-bearing, nonunion, improper implant selection/sizing, eccentric nail placement. | Revision surgery: Exchange nailing (larger diameter, longer nail), adjunctive plating, or conversion to plate osteosynthesis, often combined with bone grafting if nonunion is present. Address underlying cause (e.g., correct comminution, optimize bone biology). |
| Iatrogenic Fracture | <1% (distal comminution during reaming/nail insertion), entry point fracture | Aggressive reaming, oversized nail, improper entry point, excessive force during insertion, poor bone quality | Intra-operative fixation with additional screws/cerclage wires or longer nail/plate to span the new fracture. Preventative measures: careful reaming, appropriate nail sizing, correct entry point. |
| Avascular Necrosis (AVN) of Femoral Head | Rare (0.1-0.5%) | Piriformis fossa entry point (historically more common), direct injury to retinacular vessels during reduction or guidewire manipulation. | Recognition and monitoring. Non-weight-bearing initially. Core decompression for early stages. Total hip arthroplasty (THA) for advanced collapse and symptoms in appropriate patients. |
| Nerve/Vascular Injury | Very rare | Direct trauma during approach or screw insertion (e.g., sciatic nerve with posterior screw, femoral artery/nerve with anterior perforation) | Immediate recognition and surgical repair for vascular injury. Observation and supportive care for neuropraxia. Nerve exploration and repair for persistent deficits. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | DVT: 10-40% (without prophylaxis); PE: 1-5% (symptomatic) | Immobilization, surgical trauma, underlying hypercoagulable states, advanced age | Prophylaxis: Chemical (LMWH, fondaparinux) and mechanical (compression stockings, IPCs). Management: Anticoagulation (therapeutic). |
| Pain at Greater Trochanteric Entry Site | 10-20% | Nail prominence, irritation of the gluteus medius/trochanteric bursa | Conservative management (NSAIDs, physical therapy). If persistent and symptomatic, hardware removal (nail extraction) once fracture is healed and stable. |
General Principles of Complication Management
- Early Recognition: Vigilant post-operative monitoring and a low threshold for investigation (radiographs, CT, lab tests).
- Correction of Underlying Issues: Address medical comorbidities, nutritional deficiencies, and bone health.
- Revision Surgery: Many complications necessitate re-operation. The choice of revision strategy depends on the specific complication, fracture healing status, bone quality, and patient factors.
- Prophylaxis: Strict adherence to surgical principles (asepsis, gentle tissue handling), proper implant selection and technique, and routine DVT prophylaxis are essential preventive measures.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral component of successful treatment for subtrochanteric femur fractures. The primary goals are to restore function, prevent stiffness, and facilitate union while protecting the surgical construct. Protocols must be individualized based on fracture stability, quality of fixation, patient comorbidities, and surgeon preference.
Immediate Post-Operative Period (Day 0-7)
- Pain Management: Aggressive multi-modal pain management (opioids, NSAIDs, acetaminophen, nerve blocks) to facilitate early mobilization.
-
Weight-Bearing (WB) Status:
- Protected Weight-Bearing (PWB) or Touch-Down Weight-Bearing (TDWB): For most stable IMN constructs, early protected weight-bearing is initiated. This typically involves 10-25% body weight, emphasizing touch-down to maintain proprioception and stimulate healing without overloading the implant.
- Non-Weight-Bearing (NWB): May be indicated for highly comminuted fractures, very unstable fixation, severe osteoporosis, or cases where plate fixation was used without strong medial cortical support.
- Toe-Touch Weight-Bearing (TTWB): Often used interchangeably with TDWB, emphasizing minimal load.
-
Range of Motion (ROM):
- Ankle Pumps: Essential to prevent DVT.
- Knee Flexion/Extension: Gentle active and passive ROM exercises for the knee. Continuous passive motion (CPM) may be used but is not universally indicated.
- Hip Flexion: Active and active-assistive hip flexion up to 90 degrees as tolerated, avoiding excessive abduction or external rotation against resistance if the proximal fragment was unstable.
-
Transfers and Mobility:
- Begin with assisted transfers to a chair or commode.
- Ambulation with appropriate assistive devices (walker, crutches), emphasizing proper weight-bearing technique as prescribed.
- Incision Care: Monitor wound for signs of infection.
Early Rehabilitation Phase (Weeks 1-6)
-
Progression of Weight-Bearing:
- Gradual increase in weight-bearing as pain allows and radiographic healing progresses. This is typically guided by follow-up radiographs (at 2, 6, and 12 weeks post-op).
- Progression from PWB/TDWB to Partial Weight-Bearing (PWB, 50%) and then Weight-Bearing As Tolerated (WBAT).
-
Strengthening:
- Isometric Exercises: Quadriceps sets, gluteal sets.
- Gentle Active-Assistive and Active ROM: Focus on hip and knee.
- Resistance Exercises: Begin with elastic bands for hip abductors, adductors, flexors, and extensors. Leg presses (with caution) may be introduced.
- Core Strengthening: Crucial for overall stability.
- Gait Training: Refine ambulation mechanics with assistive devices. Focus on equal step length and symmetry.
- Patient Education: Reinforce weight-bearing precautions, proper use of assistive devices, and home exercise program.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Full Weight-Bearing (FWB): Typically achieved around 8-12 weeks, once radiographic evidence of bridging callus is present and the fracture site is clinically stable.
-
Advanced Strengthening:
- Increase resistance and repetitions for all muscle groups.
- Introduce closed-chain exercises (mini-squats, step-ups, lunges).
- Balance and proprioception exercises.
- Endurance Training: Stationary cycling, swimming (once incision healed).
- Weaning from Assistive Devices: Progress from walker to crutches, then to a cane, and finally independent ambulation.
Advanced Rehabilitation Phase (Months 3-6 and Beyond)
-
Functional Training:
- Sport-specific or activity-specific drills.
- Plyometrics and agility training for younger, active individuals.
- Return to work or recreational activities as appropriate.
-
Long-Term Goals:
- Achieve full, pain-free ROM and strength.
- Maintain bone health (especially in elderly patients, consider osteoporosis management).
- Address any residual gait abnormalities or muscle imbalances.
-
Hardware Removal:
- Generally not routine unless symptomatic (e.g., trochanteric pain from nail prominence, irritation from distal locking screws).
- Considered typically 12-18 months post-op, after documented radiographic union and resolution of pain.
Important Considerations:
- Atypical Femoral Fractures (AFFs): Often require prolonged protected weight-bearing due to delayed healing, potentially up to 6 months or more.
- Individualization: Protocols must be tailored to each patient's progress, pain levels, and specific fracture characteristics. Close communication between the surgeon, physical therapist, and patient is essential.
- Radiographic Monitoring: Regular follow-up radiographs are critical to assess healing progression and guide weight-bearing advancement.
Summary of Key Literature / Guidelines
The surgical management of subtrochanteric femur fractures has evolved considerably, with clear consensus emerging on optimal treatment strategies, largely driven by biomechanical studies and clinical outcomes.
Intramedullary Nailing as the Gold Standard
- Consensus: Extensive literature consistently supports antegrade intramedullary nailing (IMN) as the gold standard for nearly all subtrochanteric femur fractures. This is primarily due to its load-sharing characteristics, high biomechanical stability, and minimally invasive nature compared to plate osteosynthesis.
- Key Studies: Meta-analyses and systematic reviews comparing IMN to plate fixation (e.g., dynamic hip screw, static side plates) for subtrochanteric fractures generally demonstrate superior or equivalent union rates and lower rates of re-operation, hardware failure, and infection with IMN.
- Trochanteric Entry Nails: Modern trochanteric entry nails are generally preferred over piriformis entry nails. Studies have shown that trochanteric entry is associated with a lower risk of iatrogenic avascular necrosis of the femoral head and easier insertion due to better alignment with the femoral canal, without compromising stability.
- Long vs. Short Nails: For subtrochanteric fractures, particularly those with comminution or extension into the diaphysis, long intramedullary nails extending to the distal femoral metaphysis are generally recommended. This approach reduces the risk of distal femoral shaft fractures above the tip of a short nail, providing a more robust construct and protecting the entire diaphyseal segment.
- Reamed vs. Unreamed Nailing: Reamed intramedullary nailing typically allows for insertion of a larger diameter nail, improving bone-implant contact and construct stability, with good union rates. While concerns about fat embolization exist, modern reaming techniques have minimized this risk.
Role of Plate Osteosynthesis
-
Limited Indications:
Plate fixation (e.g., LCP, LISS) is reserved for specific situations where IMN is difficult or contraindicated. These include:
- Fractures with significant comminution extending into the piriformis fossa or femoral neck, making proximal IMN fixation challenging.
- Extremely wide medullary canals that cannot be adequately filled by available IMNs.
- Certain reverse obliquity patterns (AO/OTA 32-A3.3) where IMN may allow medial displacement of the distal fragment, although controversy exists, and blocking screws with IMN can address this.
- Failed IMN necessitating revision.
- Biomechanical Considerations: Plating requires a more extensive soft tissue dissection and is typically a load-bearing construct. When utilized, locking plates are preferred for their angular stability, reducing the risk of screw pullout in osteoporotic bone.
Atypical Femoral Fractures (AFFs)
- Specific Guidelines: The American Academy of Orthopaedic Surgeons (AAOS) has published clinical practice guidelines for AFFs.
- Management: Prophylactic nailing is indicated for incomplete AFFs due to the high risk of progression to complete fracture. Discontinuation of bisphosphonates (if possible) is recommended, and the patient should be evaluated for other risk factors and nutritional deficiencies (e.g., Vitamin D).
- Healing Challenges: AFFs are known for delayed healing and a higher incidence of nonunion, necessitating prolonged protected weight-bearing and potential adjunctive biological treatments. Prophylactic nailing of the contralateral femur is often considered due to the high rate of bilaterality.
Adjunctive Techniques
- Blocking Screws (Poller Screws): These are strategically placed screws (typically unicortical) that block the nail path, guiding it into the desired anatomical reduction. They are particularly useful for correcting varus-valgus and anterior-posterior angulation, especially in fractures with significant comminution or those tending towards malalignment. Evidence supports their use in optimizing reduction and preventing malunion.
- Cerclage Wires: While useful for achieving reduction in highly comminuted patterns, their use in subtrochanteric fractures can be controversial. They require open exposure and can compromise the periosteal blood supply, potentially increasing the risk of nonunion. They should be used judiciously and minimally.
- Bone Grafting: While not routinely indicated for primary IMN of acute subtrochanteric fractures, bone grafting (autograft or allograft) may be considered for significant segmental bone loss, anticipated delayed union, or in the setting of nonunion revision surgery.
Conclusion
The current literature overwhelmingly supports a protocolized approach to subtrochanteric femur fractures, emphasizing meticulous pre-operative planning, the primary use of antegrade intramedullary nailing (preferably long, trochanteric-entry nails), precise reduction techniques often aided by blocking screws, and robust post-operative rehabilitation. Continuous medical optimization, diligent monitoring for complications, and a readiness for revision surgery remain critical to achieving favorable outcomes in this challenging fracture population.
