Introduction & Epidemiology
Pelvic ring injuries represent a spectrum of high-energy trauma, often associated with significant morbidity and mortality. They typically result from motor vehicle collisions, falls from height, or crush injuries. The Young-Burgess classification system, widely utilized for its correlation with injury mechanism and stability, categorizes these fractures based on the predominant force vector: anteroposterior compression (APC), lateral compression (LC), vertical shear (VS), and combined mechanical (CM).
Anteroposterior Compression (APC) injuries result from external rotation forces applied to the hemipelvis. These forces typically lead to disruption of anterior pelvic structures, progressing posteriorly with increasing energy.
*
APC I:
Involves pubic symphysis diastasis of less than 2.5 cm or an isolated pubic ramus fracture. The posterior sacroiliac (SI) ligamentous complex remains intact, rendering the injury rotationally and vertically stable.
*
APC II:
Characterized by pubic symphysis diastasis greater than 2.5 cm and/or disruption of the anterior sacroiliac ligaments. The sacrotuberous and sacrospinous ligaments may also be disrupted. Crucially, the posterior sacroiliac ligamentous complex remains intact, preventing vertical instability. This injury is considered rotationally unstable but vertically stable, often described as an "open-book" injury.
*
APC III:
Represents complete disruption of the pubic symphysis, anterior and posterior sacroiliac ligaments, often with associated sacral fractures or avulsion of the sacrotuberous and sacrospinous ligaments. This results in both rotational and vertical instability.
Epidemiologically, pelvic ring injuries are critical due to their potential for massive hemorrhage, associated visceral damage (urogenital, gastrointestinal), neurological deficits, and high mortality rates, particularly in hemodynamically unstable patients. APC II injuries, while less severe than APC III or VS injuries, still necessitate prompt recognition and appropriate management to prevent long-term instability, pain, and functional impairment. The incidence of associated injuries can range from 10-30% for urogenital injuries and up to 50% for other organ system damage. Early, effective stabilization is paramount to improving outcomes.
Surgical Anatomy & Biomechanics
A thorough understanding of pelvic anatomy and biomechanics is fundamental to managing APC II injuries. The pelvic ring comprises the two innominate bones (ilium, ischium, pubis) and the sacrum, forming a robust, weight-bearing structure that transfers forces from the axial skeleton to the lower extremities.
Key Anatomical Structures
-
Bony Pelvis:
- Sacrum: A keystone bone articulating with the ilia via the sacroiliac joints.
- Ilium: The largest part of the innominate bone, forming the upper and lateral aspects.
- Pubis: The anterior-most part of the innominate, joining at the pubic symphysis.
- Ischium: The posterior-inferior part, contributing to the acetabulum and ischial tuberosity.
-
Ligamentous Structures: The stability of the pelvic ring is predominantly conferred by its robust ligamentous apparatus.
- Pubic Symphysis: Fibrocartilaginous joint with superior and inferior pubic ligaments. Diastasis here is a hallmark of APC injuries.
-
Sacroiliac Joint Ligaments:
- Anterior Sacroiliac Ligaments: Relatively thin, contributing to rotational stability. Disrupted in APC II and APC III.
- Posterior Sacroiliac Ligaments: Extremely strong, providing the primary vertical stability of the posterior pelvic ring. These typically remain intact in APC II injuries, differentiating them from APC III. They include the interosseous, short posterior, and long posterior SI ligaments.
-
Extrinsic Pelvic Ligaments:
- Sacrotuberous Ligament: Connects the sacrum/coccyx to the ischial tuberosity, limiting upward rotation of the sacrum. May be disrupted in APC II.
- Sacrospinous Ligament: Connects the sacrum/coccyx to the ischial spine, further limiting sacral rotation. May be disrupted in APC II.
- Iliolumbar Ligaments: Connect the L4/L5 transverse processes to the iliac crest, offering additional stability.
-
Neurovascular Structures:
- Lumbosacral Plexus: Formed by L4-S4 nerve roots, it lies anterior to the piriformis muscle and posterior to the internal iliac vessels. Injuries can lead to sciatic or femoral nerve deficits.
- Superior Gluteal Artery and Vein: Emerge from the greater sciatic notch above the piriformis. Vulnerable in posterior SI disruptions or sacral fractures.
- Internal Iliac Artery and Vein: Main blood supply to pelvic organs and gluteal region. Branches (e.g., obturator artery) are near the anterior pubic ring.
- Urogenital Structures: Bladder and urethra are intimately associated with the anterior pelvic ring. The bladder sits superior to the pubic symphysis, and the urethra passes just inferior. Spermatic cords in males and round ligaments in females pass through the inguinal canal, superior to the pubis.
Biomechanics of APC II Injuries
The APC mechanism involves an external rotation force that "opens" the pelvis like a book.
* In APC II injuries, this force first disrupts the pubic symphysis, leading to diastasis greater than 2.5 cm.
* Concurrently, the anterior sacroiliac ligaments are torn, allowing for further external rotation of the hemipelvis.
* The sacrotuberous and sacrospinous ligaments, which resist external rotation, may also stretch or tear.
* Crucially, the strong posterior sacroiliac ligaments remain intact, acting as a hinge. This prevents superior migration of the hemipelvis and maintains vertical stability, distinguishing APC II from APC III injuries.
* The integrity of the posterior SI ligaments is key to the "rotationally unstable, vertically stable" classification of APC II injuries. Failure to recognize and address the rotational instability can lead to chronic pain, gait disturbance, and persistent deformity.
Indications & Contraindications
The decision-making process for managing APC II pelvic ring injuries involves a careful assessment of the patient's hemodynamic status, the extent of pelvic ring instability, and associated injuries.
Indications for Operative Management
The primary goal of operative management for APC II injuries is to restore mechanical stability of the pelvic ring and reduce pain.
-
Pubic Symphysis Diastasis:
- Diastasis greater than 2.5 cm in an APC mechanism is the defining characteristic requiring stabilization.
- Failure of closed reduction to adequately narrow the symphysis diastasis (typically to < 1 cm) or to maintain reduction.
- Rotational Instability: Clinically evident rotational instability of the hemipelvis, confirmed by imaging (e.g., significant gapping on external rotation views, or persistent symphysis diastasis despite binder application).
- Associated Open Fracture: Any open pelvic fracture component necessitates surgical debridement and stabilization to prevent infection and promote healing.
- Neurological Deficit: Progressive or new neurological deficits attributable to the pelvic injury, though less common in pure APC II, may necessitate exploration and stabilization.
- Hemodynamic Instability: While not a direct indication for definitive plating, persistent hemodynamic instability due to pelvic hemorrhage, not controlled by non-operative measures (e.g., pelvic binder, angioembolization, pre-peritoneal packing), often leads to emergent external fixation for temporary stabilization, followed by definitive internal fixation once stabilized.
- Need for Early Mobilization: In polytrauma patients or those with multiple comorbidities, early definitive fixation allows for more aggressive mobilization and rehabilitation, reducing complications associated with prolonged bed rest.
Contraindications for Operative Management
Absolute contraindications are few and mostly relate to the patient's overall medical status. Relative contraindications may lead to delayed or staged surgical approaches.
-
Absolute Contraindications:
- Uncontrolled Hemorrhage/Shock: The patient must be hemodynamically stable and resuscitated prior to elective or semi-elective definitive fixation. Emergent external fixation can be a life-saving temporizing measure.
- Severe Local Soft Tissue Compromise: Extensive degloving injuries (e.g., Morel-Lavallée lesion) or severe open wounds over the intended surgical site may necessitate staged management, allowing soft tissue healing or coverage prior to internal fixation.
- Active Infection: Pre-existing systemic infection or cellulitis at the surgical site.
- Uncontrolled Coagulopathy: Risk of massive bleeding outweighs benefits.
-
Relative Contraindications:
- Major Comorbidities: Patients with severe cardiac, pulmonary, or other medical conditions that significantly increase anesthetic or surgical risk. Optimization of these conditions is crucial.
- Associated Life-Threatening Injuries: Other more pressing life-threatening injuries (e.g., severe head injury, abdominal trauma) may necessitate delaying definitive pelvic fixation until the patient is stable and cleared by other surgical teams.
- Stable APC I Injuries: These are managed non-operatively.
Operative vs. Non-Operative Indications for Pelvic Ring Injuries
| Feature / Injury Type | Operative Management | Non-Operative Management |
|---|---|---|
| APC II Pelvic Ring | Pubic symphysis diastasis > 2.5 cm | APC I (symphysis < 2.5 cm, stable) |
| Anterior SI ligament disruption | Minimal displacement (<2.5 cm) | |
| Inability to maintain closed reduction | Co-morbidities precluding surgery (relative) | |
| Associated open fracture | Severe local soft tissue compromise (initial) | |
| Progressive neurological deficit | ||
| Hemodynamic Status | Unstable (after initial resuscitation/embolization) | Stable (e.g., APC I, some LC I) |
| Persistent instability despite external fixation | ||
| Soft Tissue Conditions | Minor soft tissue injury or controlled open wound | Significant local soft tissue compromise, active infection |
| Patient Status | Medically optimized for surgery | High surgical risk, life-threatening associated injuries |
| Specific Ligamentous | Anterior sacroiliac ligament disruption (APC II, III) | Intact posterior sacroiliac complex (APC I, LC I) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes in APC II pelvic ring injuries, reducing operative time, and minimizing complications.
Initial Resuscitation & Stabilization
- ATLS Protocol: Adherence to Advanced Trauma Life Support guidelines is paramount. Initial assessment, resuscitation, and management of life-threatening injuries take precedence.
-
Hemorrhage Control:
Pelvic ring injuries are notorious for significant blood loss.
- Pelvic Binder/Sheet: Immediate application of a pelvic binder or sheet wrap at the level of the greater trochanters can effectively reduce pelvic volume, tamponade venous bleeding, and partially reduce an open-book injury.
- Angiography and Embolization: For arterial hemorrhage, often from branches of the internal iliac artery, angiography with selective embolization is a life-saving intervention.
- Pre-peritoneal Pelvic Packing: Surgical packing of the retroperitoneal space can be effective for venous or small arterial bleeding not amenable to embolization, particularly in hemodynamically unstable patients.
- Massive Transfusion Protocol: Activation of a massive transfusion protocol is often required.
Diagnostic Imaging
-
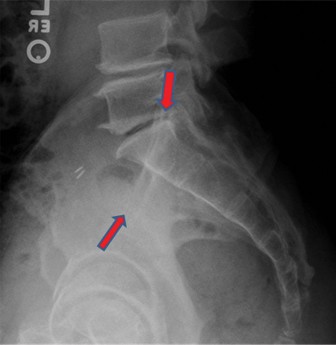
Plain Radiographs:
AP pelvis, inlet, and outlet views are standard for initial assessment.
- AP View: Demonstrates symphysis diastasis and gross pelvic architecture.
- Inlet View: Provides information about anterior-posterior displacement and rotation of the hemipelvis; crucial for assessing symphyseal and anterior SI joint widening.
- Outlet View: Shows vertical displacement of the hemipelvis and sacral anatomy.
-
Computed Tomography (CT) Scan:
The cornerstone of definitive diagnostic imaging.
- Axial, Coronal, and Sagittal Views: Provide detailed assessment of the pubic symphysis, anterior SI joint, posterior SI ligaments, and sacrum.
- 3D Reconstructions: Invaluable for visualizing the overall pelvic deformity, fracture patterns, and planning surgical approaches. Essential for confirming rotational instability and integrity of posterior SI ligaments in APC II injuries.
- CT Angiography: May be performed if there is suspicion of ongoing arterial hemorrhage.
Timing of Surgery
- Emergent Stabilization: Hemodynamically unstable patients may require emergent pelvic external fixation (anterior frame) to rapidly stabilize the pelvic ring, reduce volume, and control hemorrhage. This is often a temporizing measure.
- Definitive Internal Fixation: Ideally performed once the patient is hemodynamically stable, soft tissues are amenable (swelling has decreased, no open wounds or degloving requiring immediate attention), and associated life-threatening injuries have been managed. This window is typically within 24-72 hours, but can be delayed up to 5-7 days if necessary. Early definitive fixation is associated with better outcomes and reduced complications.
Patient Positioning
The patient is typically positioned supine on a radiolucent operating table.
1.
Table Setup:
Ensure the entire pelvis and lower extremities are within the C-arm imaging field. A radiolucent carbon fiber table is preferred.
2.
Leg Positioning:
Legs are abducted and slightly flexed at the hip and knee, often supported on padded bolsters or leg holders, to allow access for fluoroscopy and to potentially assist with reduction maneuvers. The lower extremities should be freely movable for intraoperative checks of limb length and rotation.
3.
Pelvic Bump:
Some surgeons place a small, rolled blanket or bump under the ipsilateral gluteal region to slightly elevate and internally rotate the hemipelvis, which can facilitate exposure during the anterior approach to the symphysis.
4.
C-arm Access:
Ensure unrestricted access for intraoperative fluoroscopy (AP, inlet, and outlet views). Sterile draping should accommodate this.
5.
Catheterization:
A Foley catheter is inserted prior to draping to decompress the bladder and protect it from iatrogenic injury during dissection.
6.
Prepping and Draping:
The abdomen from the xiphoid to the mid-thighs should be prepped and draped in a sterile fashion.
Detailed Surgical Approach / Technique
The definitive treatment for an APC II pelvic ring injury primarily involves anterior fixation of the pubic symphysis. The goal is to anatomically reduce the symphysis diastasis and provide rigid fixation to restore rotational stability.
General Principles
- Reduction First, Fixation Second: Accurate reduction of the pubic symphysis is paramount. Fluoroscopic guidance is essential throughout the procedure.
- Protection of Neurovascular and Urogenital Structures: Careful dissection and retraction are critical to avoid injury to the bladder, urethra, spermatic cords/round ligaments, and associated vessels.
- Stable Fixation: The construct must be strong enough to withstand physiological loads during the healing phase.
Surgical Approach: Anterior Plating of the Pubic Symphysis
The most common approach is the Pfannenstiel incision or a modified Stoppa approach.
-
Incision:
- Pfannenstiel Incision: A curvilinear transverse incision made approximately 2-3 cm superior to the pubic symphysis, extending laterally for 8-12 cm. This offers excellent cosmetic results and adequate exposure.
- Modified Stoppa (Midline Infraumbilical) Incision: A vertical incision from the umbilicus to the pubic symphysis can be used, particularly in polytrauma settings, if more extensive exposure is needed for associated abdominal pathology, or if dealing with a concomitant vertical shear component requiring access to the anterior sacrum or iliac wings. For pure APC II, Pfannenstiel is often sufficient.
-
Dissection:
- Skin and Subcutaneous Tissue: Incise and retract. Identify and coagulate any superficial vessels.
- Anterior Rectus Sheath: Incise the anterior rectus sheath transversely (Pfannenstiel) or longitudinally (midline).
- Rectus Abdominis Muscles: The rectus muscles are then separated in the midline, revealing the underlying preperitoneal fat. Careful blunt dissection here avoids injury to vessels (inferior epigastric vessels course laterally) and nerves.
-
Preperitoneal Space:
Bluntly dissect the preperitoneal fat and peritoneum from the posterior aspect of the pubic symphysis and superior pubic rami.
-
Key Structures to Identify and Protect:
- Bladder: Located immediately posterior and inferior to the pubic symphysis. Keep the Foley catheter in place and ensure it is not pulled or lacerated during retraction. It should be gently retracted superiorly and posteriorly.
- Spermatic Cords (Males) / Round Ligaments (Females): These structures exit the inguinal canal laterally and superiorly to the pubic tubercles. Identify and protect them, often by retracting them laterally.
- Obturator Neurovascular Bundle: Lies more posteriorly within the obturator foramen but can be at risk with deep dissection or misplaced screws.
-
Key Structures to Identify and Protect:
- Exposure: Expose the anterior and superior surfaces of the pubic symphysis and approximately 2-3 cm of the superior pubic rami bilaterally. Clear any hematoma or debris from the symphyseal joint space.
-
Reduction:
- Initial Assessment: Visually inspect the symphysis diastasis and confirm rotational instability.
-
Reduction Maneuver:
- External Compression: The most common method involves direct manual compression of the greater trochanters by an assistant. This attempts to "close the book."
- Pelvic Reduction Clamps: A C-clamp or specific symphysis reduction clamps (e.g., Jungbluth clamp) can be applied. The points of the clamp are typically placed on the anterior superior iliac spines (ASIS) or iliac crests to apply controlled compression.
- Internal Reduction: A bone hook or pointed reduction clamp can be used directly on the pubic tubercles to achieve reduction.
- Fluoroscopic Confirmation: Under C-arm guidance (AP view), confirm anatomical reduction of the pubic symphysis (diastasis < 1 cm, parallel cortical margins). Inlet and outlet views should also be checked to ensure no residual rotational or vertical malalignment. The posterior elements (SI joints, sacrum) should appear normal on inlet/outlet views, confirming the APC II nature of the injury.
-
Fixation:
-
Plate Selection:
- 3.5 mm Reconstruction Plate: A common choice, typically a 4-hole or 6-hole plate contoured to fit the superior aspect of the pubic bodies.
- Dedicated Symphysis Plate: Some manufacturers offer pre-contoured symphysis plates designed for improved anatomical fit and strength.
- Two-Plate Construct: For very unstable or obese patients, two parallel 3.5 mm plates (e.g., 2-hole or 3-hole) can be applied superiorly and anteriorly for enhanced rotational stability. This configuration offers increased stiffness against torsional forces.
- Plate Placement: The plate is usually placed on the superior aspect of the pubic bodies, just posterior to the anterior cortical edge, to maximize bone purchase and avoid irritation from overlying soft tissues. Ensure the plate lies flat without tenting.
-
Screw Insertion:
- Pilot Holes: Drill pilot holes for screws, ensuring appropriate angulation. The screws should be directed slightly superiorly and posteriorly to achieve bicortical purchase while avoiding the bladder and urethra posteriorly and inferiorly.
- Screw Length: Measure screw lengths carefully. Aim for bicortical purchase (engaging both anterior and posterior cortices of the pubic bone) for maximum stability. Screw tips should not protrude significantly posteriorly to avoid irritation or injury to the bladder or neurovascular structures.
- Number of Screws: Typically, at least two bicortical screws are placed in each pubic body segment (total of 4-6 screws for a 4- or 6-hole plate).
- Compression: For symphyseal plating, compression across the fracture is not usually the primary goal, as the goal is to close an existing diastasis. However, lag screw technique can be considered for symphyseal fractures if present in addition to diastasis.
-
Plate Selection:
-
Closure:
- Irrigation: Thoroughly irrigate the wound.
- Drain: A suction drain may be placed in the preperitoneal space if there is significant hematoma or anticipated seroma.
- Rectus Sheath: Reapproximate the anterior rectus sheath with absorbable sutures.
- Subcutaneous Tissue and Skin: Close in layers.
Potential Additional Posterior Fixation for APC II?
While classic APC II is considered vertically stable due to intact posterior SI ligaments, some surgeons may consider supplemental posterior fixation (e.g., SI screws, transiliac internal fixator) in specific circumstances:
* If there is any doubt about the integrity of the posterior SI complex (e.g., subtle widening on stress views or equivocal CT findings).
* In very high-demand patients or those with significant obesity where anterior plating alone might be insufficient to prevent long-term loosening or failure.
* If there's an associated sacral fracture, even if minimally displaced, that contributes to rotational instability.
However, for a pure APC II injury, anterior symphysis plating remains the gold standard and is generally sufficient for restoring rotational stability.
Complications & Management
Pelvic ring injuries and their surgical management are associated with a significant risk of complications. Proactive recognition, prevention, and timely management are crucial for optimal patient outcomes.
General Complications of Pelvic Trauma & Surgery
-
Hemorrhage:
The most life-threatening early complication. Can be arterial (often from internal iliac branches) or venous (from cancellous bone or disrupted venous plexuses).
- Incidence: Varies widely, but significant bleeding requiring transfusion is common.
- Management: Aggressive resuscitation, pelvic binder, angioembolization (for arterial), pre-peritoneal packing (for venous), massive transfusion protocol. Intraoperatively, meticulous hemostasis.
-
Infection:
Surgical site infection (SSI) can be superficial or deep.
- Incidence: 1-5% for anterior pelvic fixation. Higher in open fractures.
- Management: Prophylactic antibiotics, strict aseptic technique. For superficial SSI: wound care, oral antibiotics. For deep SSI: surgical debridement, intravenous antibiotics, potential hardware removal if chronic or persistent.
-
Neurovascular Injury:
Damage to nerves or vessels during initial trauma or surgical dissection/screw placement.
- Incidence: < 1-2%, though specific nerve irritation can be higher.
- Management: Careful anatomical dissection, meticulous screw placement under fluoroscopy. For vascular injury: immediate repair, vascular consultation. For nerve injury: decompression, observation, possible exploration and repair.
-
Urogenital Injury:
Bladder or urethral injury.
- Incidence: < 1% with anterior plating, higher with complex trauma.
- Management: Pre-operative Foley catheter. If injury suspected or identified: urological consultation, primary repair, prolonged catheterization.
-
Malunion/Nonunion:
Failure of the symphysis to heal in an anatomically acceptable position.
- Incidence: 2-10%, depending on injury severity and fixation quality.
- Management: Symptomatic malunion/nonunion may require revision surgery with osteotomy, bone grafting, and stronger fixation.
-
Chronic Pain:
Persistent pain in the pelvic region.
- Incidence: Up to 20-40% despite adequate fixation and union. Often multifactorial (ligamentous laxity, nerve irritation, muscle imbalance).
- Management: Multimodal pain management, physical therapy, psychological support, hardware removal if symptomatic (e.g., prominent plate causing bursitis or nerve irritation).
Specific Complications of Anterior Symphysis Plating
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Neurovascular Injury | <1-2% | Immediate vascular repair, nerve decompression/exploration, careful surgical technique, fluoroscopic guidance for screws. |
| Urogenital Injury | <1% | Urological consultation, primary repair of bladder/urethra, prolonged Foley catheterization. Careful bladder retraction. |
| Surgical Site Infection | 1-5% | Debridement, targeted antibiotics, hardware removal if deep and persistent, vacuum-assisted closure. |
| Malunion / Nonunion | 2-10% | Revision surgery with osteotomy, bone grafting, stronger plate construct, or supplemental posterior fixation. |
| Hardware Failure | 5-15% | Screw pullout, plate bending/fracture. Revision with stronger/longer plate, bicortical screws, consideration of two-plate construct. |
| Heterotopic Ossification (HO) | Up to 20% | NSAIDs (e.g., Indomethacin) or radiation prophylaxis in high-risk patients. Surgical excision if symptomatic and mature. |
| Chronic Pain/Bursitis | 20-40% | Multimodal pain management, physical therapy, hardware removal if symptomatic (e.g., prominent plate, pseudoarthrosis). |
| Inguinal Hernia | <1% | Surgical repair of fascial defect. Careful rectus sheath closure. |
Prevention and Mitigation Strategies
- Comprehensive Pre-operative Planning: Detailed CT scans, including 3D reconstructions, for accurate injury assessment.
- Optimal Patient Positioning: Ensure adequate exposure and fluoroscopic access.
- Careful Surgical Technique: Meticulous dissection, identification, and protection of vital structures (bladder, spermatic cords, neurovascular bundles).
- Anatomic Reduction: Achieve and maintain precise reduction of the symphysis.
- Rigid Fixation: Use appropriate plate size, length, and bicortical screw purchase to ensure mechanical stability.
- Prophylactic Measures: DVT prophylaxis, prophylactic antibiotics, and HO prophylaxis (if indicated).
- Early Mobilization: As soon as pain and stability allow, to reduce complications of immobility.
- Post-operative Monitoring: Close observation for signs of infection, neurovascular compromise, or hardware-related issues.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to maximizing functional recovery, preventing stiffness, and minimizing long-term disability following surgical fixation of APC II pelvic ring injuries. Protocols are typically progressive and tailored to individual patient needs, injury severity, and bone healing.
Phase 1: Immediate Post-Operative (0-6 weeks)
Goals:
Pain control, wound healing, prevention of complications, initiation of gentle motion, protection of fixation.
*
Weight-Bearing Status:
*
Protected Weight-Bearing:
Often initiated as touch-down weight-bearing (TDWB) or non-weight-bearing (NWB) on the affected lower extremity using crutches or a walker. This allows initial soft tissue healing and minimizes stress on the symphyseal repair.
*
Early Weight-Bearing:
In stable APC II repairs with robust fixation and no associated posterior instability, some surgeons advocate for early partial weight-bearing (PWB) as tolerated, progressing to full weight-bearing (FWB) over the initial weeks, citing benefits in bone healing and functional recovery. This decision is based on surgeon preference and radiographic stability.
*
Pain Management:
Multimodal approach including NSAIDs, acetaminophen, nerve blocks, and opioid analgesics as needed.
*
Wound Care:
Daily inspection of incision for signs of infection or dehiscence.
*
Deep Vein Thrombosis (DVT) Prophylaxis:
Pharmacological (low molecular weight heparin or direct oral anticoagulants) and mechanical (sequential compression devices) prophylaxis is critical due to the high risk in pelvic trauma patients.
*
Early Mobilization:
*
Bed Mobility:
Instruct on safe log-rolling and transfers.
*
Transfers:
Progression from bed to chair, then chair to standing with assistance.
*
Ambulation:
With assistive devices (walker, crutches) while adhering to prescribed weight-bearing restrictions.
*
Gentle Range of Motion (ROM):
Passive or active-assisted ROM for hips, knees, and ankles within pain limits. Avoid extreme external rotation or abduction of the hip on the injured side.
*
Core Stability (Gentle):
Isometric abdominal contractions (pelvic tilts) can be initiated cautiously to help activate core muscles without stressing the repair.
Phase 2: Intermediate Healing (6-12 weeks)
Goals:
Progressive increase in weight-bearing, restoring muscle strength, improving balance and gait mechanics, enhancing hip ROM.
*
Weight-Bearing Progression:
* Gradual increase in weight-bearing from TDWB/NWB to PWB, and eventually FWB, as pain allows and radiographic signs of healing appear (e.g., callus formation at symphysis, no signs of hardware loosening). This typically occurs around 8-10 weeks.
* Discontinuation of assistive devices when gait is normalized and stability is ensured.
*
Therapeutic Exercises:
*
Hip ROM:
Active and passive hip flexion, extension, abduction, and internal/external rotation, emphasizing gentle stretching to improve flexibility.
*
Strengthening:
* Isometric strengthening of hip abductors, adductors, extensors, and flexors.
* Progress to isotonic exercises with light resistance (e.g., resistance bands).
* Focus on gluteal muscle activation (glute bridges, clam shells).
* Continue core strengthening exercises, progressively increasing intensity.
*
Gait Training:
Focus on normal gait mechanics, stride length, and cadence.
*
Proprioception and Balance:
Single-leg standing exercises, wobble board training (if appropriate).
Phase 3: Advanced Rehabilitation & Return to Activity (3-6 months and beyond)
Goals:
Full restoration of strength, endurance, agility, and functional capacity; safe return to recreational, work, or sport-specific activities.
*
Full Weight-Bearing:
By 3-4 months, most patients should be able to tolerate full weight-bearing without assistive devices.
*
Progressive Strengthening:
* Advanced resistance training for lower extremities and core.
* Plyometric exercises and agility drills for athletes.
* Sport-specific training and simulations.
*
Functional Training:
Stairs, uneven surfaces, squatting, lifting.
*
Endurance Training:
Cycling, swimming, walking.
*
Activity Modification:
Avoid high-impact activities or positions that cause pain or place undue stress on the pelvis during the initial healing period. Gradually reintroduce activities.
*
Return to Work/Sport:
Dependent on the individual's recovery, occupation, and desired activity level. Generally, return to light duties at 3-6 months, and strenuous labor or competitive sports typically at 6-12 months, assuming radiographic union and full functional recovery.
*
Hardware Removal:
Not routinely performed unless symptomatic (e.g., pain, bursitis, infection, prominent hardware). If required, it is usually considered after 12-18 months, once complete bone healing is confirmed. Patients are typically allowed to FWB immediately after hardware removal if healing is complete.
Throughout the rehabilitation process, regular follow-up with the orthopedic surgeon is essential, including clinical examination and serial radiographs, to monitor healing, assess stability, and guide progression of the rehabilitation protocol. Patient education on activity modification and adherence to the rehabilitation plan is critical for long-term success.
Summary of Key Literature / Guidelines
The management of APC II pelvic ring injuries has evolved significantly, underpinned by a robust body of literature and clinical guidelines from major orthopedic trauma organizations.
Classification Systems and Stability
- Young-Burgess Classification (1990): This mechanism-based classification remains the most widely accepted due to its strong correlation with injury pattern, stability, and prognosis. APC II is defined by anterior rotational instability (symphysis diastasis > 2.5 cm, anterior SI ligament disruption) but vertical stability due to intact posterior SI ligaments.
- Tile Classification (1988, 1999): Provides a complementary anatomical description, categorizing injuries as stable, rotationally unstable, or rotationally and vertically unstable. APC II corresponds to Tile Type B1 (unstable anteriorly, stable posteriorly). The distinction between rotationally unstable (APC II, LC II) and vertically unstable (APC III, LC III, VS) injuries is critical for guiding treatment.
Initial Management and Resuscitation
- ATLS Guidelines: Emphasize rapid assessment, resuscitation, and hemorrhage control as primary goals in unstable pelvic trauma patients.
- Pelvic Binders: Early application of a circumferential pelvic binder (or sheet) at the level of the greater trochanters is a well-established intervention for temporary stabilization of APC and vertically unstable injuries. It reduces pelvic volume, tamponades bleeding, and can improve hemodynamic stability. Studies by Ghanayem et al. (1995) and other trauma groups have demonstrated the effectiveness of external compression in reducing pelvic volume and blood loss.
- Angioembolization and Pre-peritoneal Packing: Consensus guidelines from the Orthopaedic Trauma Association (OTA) and major trauma societies recommend prompt angiography with embolization for arterial hemorrhage and pre-peritoneal packing for refractory venous/small arterial bleeding in hemodynamically unstable patients, often prior to definitive fixation.
Surgical Timing and Definitive Fixation
- Early Definitive Fixation: A growing body of evidence supports early definitive stabilization of unstable pelvic ring injuries (within 24-72 hours) once the patient is hemodynamically stable and soft tissue conditions allow. Studies by Starr et al. (2009) and others have demonstrated that early fixation is associated with reduced rates of DVT, pulmonary complications, length of hospital stay, and improved functional outcomes compared to delayed fixation, particularly in polytrauma patients.
-
Anterior Plating for APC II:
Anterior fixation of the pubic symphysis with a plate remains the cornerstone of definitive treatment for APC II injuries.
- Technique: The Pfannenstiel approach is commonly used, allowing for anatomical reduction and stable fixation. A 3.5 mm reconstruction plate or dedicated symphysis plate is typically used, with at least two bicortical screws per pubic body. The importance of bicortical screw purchase for optimal stability is emphasized by biomechanical studies (e.g., Simonian et al., 1996).
- Two-Plate Construct: While a single plate is often sufficient, some authors advocate for a two-plate construct in obese patients or those with particularly unstable injuries to enhance rotational stability and resistance to failure (e.g., Gardner et al., 2011). Biomechanical studies have shown increased stiffness with two parallel plates.
- Role of Posterior Fixation in APC II: While APC II is classically vertically stable, a subtle posterior component may exist. Current consensus typically supports anterior plating alone for pure APC II injuries with definitively intact posterior SI ligaments. However, if there is any suspicion of posterior ligamentous injury or subtle widening of the posterior SI joint on stress views, supplemental posterior fixation (e.g., percutaneous iliosacral screw) may be considered to prevent late instability, as suggested by studies exploring the nuances of SI joint stability (e.g., Routt et al., 1993). This often requires a high degree of clinical judgment.
Outcomes and Complications
- Functional Outcomes: Studies report good to excellent functional outcomes in 70-85% of patients treated for APC II injuries. However, a significant proportion (20-40%) may experience chronic pain, often related to soft tissue injuries, residual ligamentous laxity, or sacroiliac joint dysfunction, even with anatomically reduced fractures (e.g., Gänsslen et al., 2005).
- Complications: The literature consistently highlights the risk of complications such as infection, neurovascular injury, bladder/urethral injury, hardware failure, and heterotopic ossification (HO). Prophylaxis for HO (e.g., NSAIDs, radiation) can reduce its incidence, particularly in high-risk patients. Hardware removal for symptomatic implants is common.
- Long-term Instability: Malunion or nonunion of the symphysis can lead to chronic pain and gait abnormalities, emphasizing the need for meticulous reduction and rigid fixation.
Guidelines and Future Directions
Organizations like the Orthopaedic Trauma Association (OTA) and AO Trauma provide comprehensive educational resources and guidelines for the management of pelvic ring injuries. These advocate for a multidisciplinary approach involving trauma surgeons, orthopedic surgeons, interventional radiologists, and urologists.
Future research continues to focus on refining classification systems, optimizing surgical techniques (e.g., minimally invasive approaches, novel fixation devices), improving outcomes in polytrauma patients, and developing better strategies for predicting and managing chronic pain and functional limitations. The role of advanced imaging techniques like dynamic CT or MRI to better assess ligamentous stability also continues to be explored.
