Surgical Management of the Spastic Hand: Proximal Row Carpectomy and Thumb-in-Palm Deformity Correction
Key Takeaway
Surgical management of the spastic hand in cerebral palsy requires a meticulous understanding of altered biomechanics. Proximal row carpectomy combined with tendon transfers addresses severe wrist flexion contractures, while targeted myotomies and skeletal stabilization correct thumb-in-palm deformities. This guide details the indications, step-by-step surgical techniques, and postoperative protocols necessary to optimize both cosmetic appearance and functional outcomes in these complex pediatric and adult orthopedic patients.
INTRODUCTION TO THE SPASTIC HAND IN CEREBRAL PALSY
The surgical management of the upper extremity in cerebral palsy presents a formidable challenge to the orthopedic surgeon. The fundamental pathoanatomy involves a complex interplay of muscle spasticity, myostatic contracture, muscle weakness, and impaired voluntary motor control. The primary goals of surgical intervention are to improve hygiene, enhance cosmetic appearance, and, when possible, augment the functional capacity of the hand for grasp and release. Two of the most challenging and frequently encountered deformities in this patient population are the severe spastic wrist flexion contracture and the thumb-in-palm deformity.
This comprehensive guide details the evidence-based surgical techniques for addressing these deformities, specifically focusing on proximal row carpectomy (PRC) combined with tendon transfer, and the multifaceted approach required for correcting the clutched thumb.
PROXIMAL ROW CARPECTOMY IN THE SPASTIC WRIST
Severe wrist flexion deformities in cerebral palsy often result from overpowering spasticity of the volar flexor compartment, particularly the flexor carpi ulnaris (FCU) and flexor carpi radialis (FCR), combined with profound weakness of the wrist extensors. When fixed myostatic contractures develop, soft tissue releases alone may be insufficient.
Omer and Capen popularized the use of proximal row carpectomy as a powerful skeletal shortening procedure to address severe, rigid wrist flexion deformities. By excising the proximal carpal row, the carpus is effectively shortened. This skeletal shortening achieves a critical biomechanical objective: it provides a relative lengthening of all flexor muscle-tendon units that cross the radiocarpal joint, thereby reducing their spastic deforming force without requiring extensive, multi-level fractional tendon lengthenings.
💡 Clinical Pearl: Functional Expectations
Omer and Capen explicitly warned that while proximal row carpectomy dramatically improves the cosmetic appearance of the severely flexed wrist and facilitates hygiene, it rarely improves active functional capacity. It is primarily considered a salvage procedure for appearance and nursing care. Patient and caregiver expectations must be meticulously managed preoperatively.
Indications and Patient Selection
- Severe, fixed wrist flexion contracture that is not passively correctable.
- Age: Patients should be older than 11 years of age to ensure adequate skeletal maturity of the carpus.
- Primary Goal: Improvement of severe cosmetic deformity or facilitation of palmar hygiene.
- Concomitant Procedures: Typically performed in conjunction with a transfer of the flexor carpi ulnaris (FCU) to the extensor carpi radialis brevis (ECRB) to provide a dorsal tether and augment wrist extension and forearm supination.
Surgical Technique: Proximal Row Carpectomy and FCU Transfer
The procedure is performed under general anesthesia with a well-padded pneumatic tourniquet applied to the proximal arm.
Step 1: Dorsal Approach and Carpectomy
- Incision: Make a longitudinal incision over the dorsum of the wrist, centered over the radiocarpal joint, in line with the third metacarpal.
- Dissection: Deepen the incision through the subcutaneous tissues. Identify and carefully protect the sensory branches of the radial nerve and the dorsal branch of the ulnar nerve.
- Extensor Retinaculum: Identify the distal edge of the dorsal carpal ligament (extensor retinaculum). Open the third dorsal compartment, transpose the extensor pollicis longus (EPL) radially, and retract the common digital extensor tendons ulnarward to expose the dorsal wrist capsule.
- Capsulotomy: Make a broad, T-shaped or H-shaped incision in the dorsal capsule to widely expose the proximal carpal row. Raise full-thickness capsular flaps to preserve tissue for later imbrication.
- Bone Excision:
- Excise the lunate entirely. Use a combination of sharp dissection and a small rongeur, being meticulous not to damage the volar radiocarpal ligaments.
- Excise the proximal half of the scaphoid. Crucial Step: Leave the distal half of the scaphoid intact with its capsular and ligamentous attachments to the trapezium and trapezoid. This preserves the scaphotrapezial-trapezoidal (STT) joint complex and prevents destabilization of the radial column.
- Excise the triquetrum, but carefully dissect it free from the pisiform. The pisiform must be left intact within the FCU tendon sheath to preserve the integrity of the FCU insertion for the subsequent transfer.
Step 2: Volar Approach and FCU Harvest
- Incision: Make a longitudinal incision over the volar-ulnar aspect of the wrist, beginning at the pisiform and extending proximally over the FCU muscle belly for approximately 10 to 12 centimeters.
- Neurovascular Protection: Identify and meticulously protect the ulnar neurovascular bundle, which lies immediately radial and deep to the FCU tendon.
- Mobilization: Free the FCU tendon and muscle belly from the surrounding intermuscular septum.
- Detachment: Divide the FCU tendon as distally as possible, near its insertion on the pisiform.
Step 3: Tendon Routing and Transfer
- Routing Options:
- For pure wrist extension: Pass the FCU tendon through a surgically created window in the interosseous membrane to the dorsal aspect of the forearm.
- For combined extension and supination (Preferred in severe pronation deformities): Pass the FCU tendon subcutaneously around the ulnar border of the forearm. This routing provides a supination vector, which is highly beneficial in the spastic, pronated forearm.
- Insertion: Route the transferred FCU tendon to the extensor carpi radialis brevis (ECRB) tendon.
- Fixation: Weave the FCU tendon through the ECRB tendon using a Pulvertaft weave technique. Anchor the transfer securely with multiple nonabsorbable monofilament sutures (e.g., 3-0 Prolene or braided polyester) under appropriate tension.
Step 4: Capsular Imbrication and Closure
- Positioning: Place the wrist in maximum passive dorsiflexion.
- Capsulorrhaphy: Imbricate (overlap and tighten) the dorsal capsule of the wrist using strong absorbable sutures. This dorsal capsular tightening is critical to act as a static checkrein against recurrent volar flexion.
- Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the skin in layers.
🚨 Surgical Warning: Postoperative Splinting
Omer and Capen emphasized that prolonged postoperative splinting is absolutely mandatory. Because the carpectomy increases the relative length of all flexor muscle-tendon units crossing the wrist, the wrist is highly susceptible to recurrent flexion deformity if the dorsal capsular imbrication and tendon transfer are not protected until mature scar tissue forms.
Postoperative Care Protocol
- Immediate Post-op: The arm is placed in a bulky, compressive dressing reinforced with a volar plaster splint holding the fingers and wrist in extension.
- Day 5: The initial dressing is removed. A circular long-arm cast is applied. The position must be strictly maintained: elbow flexed to 90 degrees, forearm in maximum achievable supination, and the wrist and fingers in extension. This cast is maintained for 6 weeks.
- Week 6 to Month 4: The long-arm cast is removed. A circular short-arm cast, incorporating dynamic outriggers for extension of the fingers, is applied. Continuous splinting is maintained for a total of 4 months postoperatively.
- Long-Term: After 4 months, the patient is transitioned to a rigid thermoplastic resting splint used exclusively at night for an indefinite period to prevent recurrence of the myostatic contracture.
THUMB-IN-PALM DEFORMITY
The thumb-in-palm (also known as adducted thumb or clutched thumb) deformity is the second most frequent and functionally devastating deformity of the hand in cerebral palsy. This posture physically blocks the entry of objects into the palm and prevents the thumb from opposing the fingers, thereby destroying both grasp and pinch kinematics.
Pathoanatomy and Deforming Forces
The deformity is rarely the result of a single spastic muscle; rather, it is a complex imbalance between overpowering spastic flexors/adductors and weak, overstretched extensors/abductors.
Primary Deforming Forces (Spastic/Contracted):
- Flexor pollicis longus (FPL)
- Adductor pollicis (AP)
- Flexor pollicis brevis (FPB)
- First dorsal interosseous (FDI)
Secondary Contributing Factors:
- Weakness of the extensor pollicis longus (EPL), extensor pollicis brevis (EPB), and abductor pollicis longus (APL).
- Paradoxical spasticity: In some cases, spasticity in the EPL muscle may actually contribute to an adduction deformity of the thumb during the release phase, pulling the thumb against the second metacarpal.
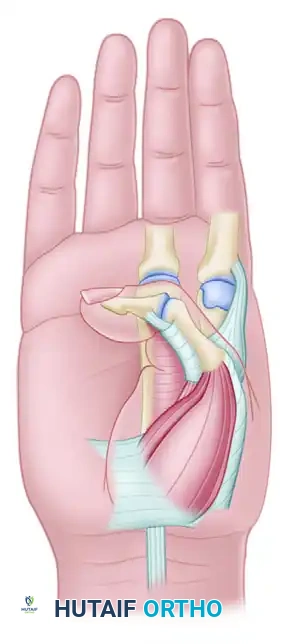
Figure 1: The adducted thumb position in cerebral palsy is the result of forces exerted by powerful spastic muscles, including the adductor pollicis, first dorsal interosseous, flexor pollicis longus, and flexor pollicis brevis.
Clinical Evaluation and Differentiating Spasticity
A meticulous clinical examination is paramount. The surgeon must differentiate between dynamic spasticity and fixed myostatic contracture.
The Tenodesis Test: To determine if the FPL is the principal deforming force, the examiner passively flexes the patient's wrist. If wrist flexion causes the thumb interphalangeal (IP) and metacarpophalangeal (MCP) joints to spontaneously extend or become easily correctable, dynamic FPL spasticity is the primary culprit. Conversely, if extending the wrist exacerbates the thumb-in-palm posture, the FPL is tight. If the thumb remains rigidly adducted into the palm regardless of wrist position, a fixed contracture of the adductor pollicis, first web space skin, or joint capsule is present.
Classification Systems
Proper classification guides surgical decision-making. Two primary systems are utilized:
House Classification (1981)
Based on the clinical appearance and joint involvement:
- Type I: Simple metacarpal adduction contracture (Most common pattern).
- Type II: Metacarpal adduction contracture combined with an MCP flexion deformity.
- Type III: Metacarpal adduction contracture combined with an MCP hyperextension deformity or profound volar plate instability (Second most common).
- Type IV: Metacarpal adduction contracture combined with both MCP and IP flexion deformities. This is the most severe form, driven by profound spasticity in both the FPL and the intrinsic thumb musculature.
Tonkin Classification
Focuses on the specific joint postures:
- Type 1: Flexed MCP joint and an extended IP joint.
- Type 2: Flexed MCP joint and flexed IP joint.
- Type 3: Flexed MCP and IP joints combined with a severe adduction contracture.
Surgical Treatment Strategies
Treatment must be highly individualized. A modern, dynamic approach (as advocated by House et al.) involves a triad of interventions: (1) Release of spastic/contracted muscles, (2) Augmentation of weak antagonist muscles, and (3) Skeletal stabilization.
1. Soft Tissue Releases and Myotomies
If a fixed contracture is present, soft tissue release is the mandatory first step.
- Adductor Pollicis Myotomy (Matev Procedure): Performed through a palmar incision parallel to the thenar crease, or via a Z-plasty in the first web space if severe skin contracture exists.
- Preoperative EMG: Highly recommended. If the adductor shows active firing during voluntary grasp (selective control), only the transverse head should be released. A complete myotomy in a patient with selective control will result in devastating pinch weakness.
- First Dorsal Interosseous Release: The origin of the FDI from the first metacarpal is stripped subperiosteally to further open the first web space.
- Flexor Pollicis Brevis Release: In long-standing Type II deformities, the origin of the FPB may also require release.
- FPL Lengthening: For Type IV deformities with severe IP flexion, the FPL tendon is lengthened via a fractional lengthening at the musculotendinous junction proximal to the wrist.
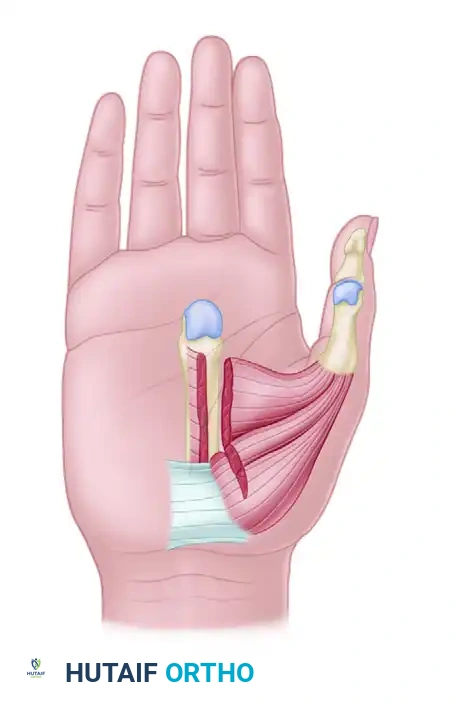
Figure 2: Myotomies of the intrinsic muscles of the thumb (Adductor pollicis, Flexor pollicis brevis) are critical for releasing the severe thumb-in-palm deformity.
2. Tendon Transfers and Augmentation
Once the deforming forces are released, the weak abductors and extensors must be augmented to pull the thumb out of the palm.
- APL Augmentation: The most common procedure. The weak abductor pollicis longus is augmented using a transfer of the palmaris longus (PL), brachioradialis (BR), or flexor carpi radialis (FCR). The transferred tendon is woven into the APL to provide a robust abduction vector.
- EPL Rerouting (Manske Procedure): If the EPL is contributing to adduction, it is transposed out of the third dorsal compartment (Lister's tubercle) and rerouted radially, often into the first dorsal compartment. This changes its vector from an adductor/extensor to a pure abductor/extensor. Manske reported significant functional improvement in 90% of patients using this technique.
- FPL Transfer (Smith Procedure): For patients with some voluntary control but severe spasticity, the FPL tendon can be transferred to the radial side of the thumb (often to the EPL), combined with an IP joint tenodesis. This converts a deforming flexor into an active extensor/abductor.
3. Skeletal Stabilization
Soft tissue balancing will fail if the underlying skeletal foundation is unstable, particularly at the MCP joint.
- MCP Arthrodesis: The gold standard for Type III deformities (MCP hyperextension/instability). In skeletally immature patients, arthrodesis can be performed without damaging the physis by meticulously removing only the articular cartilage (cup-and-cone technique) and stabilizing the joint with smooth Kirschner wires. The joint is typically fused in 15 degrees of flexion and slight pronation.
- Sesamoid Metacarpal Synostosis (Zancolli Procedure): An alternative to fusion for MCP hyperextension instability. The radial sesamoid and the volar plate are advanced proximally and fused to the neck of the first metacarpal. This creates a robust volar tether, preventing hyperextension while preserving some MCP flexion.
Postoperative Rehabilitation for Thumb Reconstruction
Following thumb-in-palm reconstruction, the hand is immobilized in a bulky dressing and a thumb spica splint with the thumb in maximum palmar abduction and extension.
- At 10 to 14 days, sutures are removed, and a well-molded short-arm thumb spica cast is applied.
- Immobilization is maintained for a minimum of 4 to 6 weeks (longer if an arthrodesis was performed, until radiographic union is confirmed).
- Following cast removal, a rigorous occupational therapy program is initiated, focusing on active grasp and release, utilizing the newly balanced tendon transfers. Nighttime thermoplastic splinting in abduction is continued for at least 6 months to prevent recurrence of the adduction contracture.
===
You Might Also Like
