Introduction & Epidemiology
Overlapping fifth toe, also known as congenital digitus minimus varus, digitus quintus varus, or overriding fifth toe, is a common congenital forefoot deformity. Characterized by a dorsal and medial deviation of the fifth digit over the fourth, it presents a unique clinical challenge due to its multifactorial etiology and potential for functional impairment. While historically considered a cosmetic concern, progressive deformity can lead to significant morbidity, including painful callosities, difficulty with shoe wear, and aesthetic distress.
The condition is congenital, often noticeable at birth or shortly thereafter, and frequently presents bilaterally in approximately 50% of cases. Epidemiological data indicates no significant predilection for either sex. While the exact incidence varies in literature, it is recognized as one of the more common congenital toe deformities. The Butler procedure, first described by Butler in 1952, has become a widely accepted surgical technique for addressing this specific deformity, aiming to restore proper anatomical alignment and functional integrity of the fifth toe.
Surgical Anatomy & Biomechanics
The overlapping fifth toe deformity is characterized by a complex interplay of skeletal malalignment and soft tissue contractures. A comprehensive understanding of these components is crucial for effective surgical planning and execution. The original description highlights seven primary anatomical deformities:
- Smaller than normal fifth toe: While subtle, the fifth digit may be hypoplastic.
- Adduction of the fifth toe toward the fourth toe: This medial deviation contributes to the overriding position.
- Dorsiflexion contracture of the fifth metatarsophalangeal (MTP) joint: This is a critical component, causing the toe to ride dorsally over the adjacent digit.
- Lateral rotation of the phalanges of the fifth toe: The digit often exhibits external or pronation rotation.
- Shortened extensor digitorum longus (EDL) tendon to the fifth toe: This is widely considered a primary deforming force, contributing significantly to the MTP joint dorsiflexion and dislocation.
- Dorsal dislocation of the fifth MTP joint: A direct consequence of the EDL contracture and capsular tightening, leading to malalignment.
- Contracted skin in the fourth web space: This skin contracture is often secondary but contributes to the adduction and overriding nature of the deformity, hindering reduction.
The biomechanics of the deformity involve an imbalance of forces acting on the fifth MTP joint. The contracted EDL tendon exerts an unopposed dorsiflexion force, leading to a fixed MTP joint extension contracture and eventual dorsal subluxation or dislocation. Concurrently, the adduction contracture, potentially involving the intrinsic muscles (e.g., abductor digiti minimi, although its role in adduction is complex given its primary abduction function) and the contracted skin in the fourth web space, pulls the toe medially. The lateral rotation further exacerbates the malposition, often presenting as a pronated fifth toe.
The MTP joint capsule, particularly its dorsal aspect, undergoes adaptive shortening and thickening in response to chronic dorsal displacement. This capsular contracture becomes a significant barrier to reduction, even after addressing the tendon and skin components. The smaller size of the fifth toe and its intrinsic anatomical variations can predispose it to this type of deformity, particularly in the presence of genetic factors influencing soft tissue development.
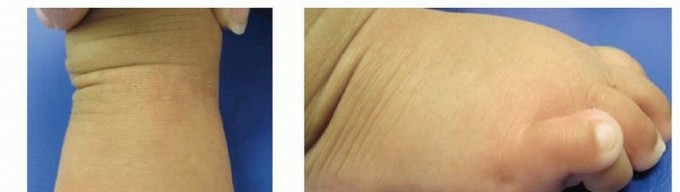
The seed content provided two illustrative images, which elucidate the clinical presentation of this condition.


FIG 1 • A,B. Frontal and lateral views demonstrating the characteristic features of overlapping fifth toe, including dorsal override, adduction, and rotation of the digit.
Understanding these interconnected anatomical and biomechanical factors is paramount for effective surgical correction, as the Butler procedure directly addresses multiple components to achieve comprehensive realignment.
Indications & Contraindications
The decision to proceed with surgical intervention for an overlapping fifth toe is guided by the patient's age, symptom severity, functional impairment, and the response to conservative management.
Non-Operative Management
Non-operative treatments are typically the first line of management, especially in younger, asymptomatic, or mildly symptomatic children. These strategies aim to gently reposition the toe and may include:
*
Taping:
Regular taping of the fifth toe into a reduced position, often performed by parents.
*
Stretching exercises:
Passive stretching to counteract soft tissue contractures.
*
Shoe modifications:
Wearing wider shoes with soft toe boxes to accommodate the deformity and reduce pressure.
*
Silicone toe spacers:
To prevent friction and maintain separation.
Non-operative treatment is generally pursued for several months. While it may provide symptomatic relief or transient correction in some cases, it rarely achieves a permanent anatomical correction of the underlying deformity, particularly once soft tissue contractures become fixed.
Operative Indications
Surgical correction, primarily via the Butler procedure, is considered when conservative measures fail to alleviate symptoms or prevent progression of the deformity.
- Persistent pain: Pain arising from dorsal callosities (which occur in approximately 50% of older children and adolescents), recurrent blisters, or irritation due to chronic shoe friction.
- Difficulty with shoe wear: Inability to comfortably wear standard footwear due to the malposition of the toe.
- Progressive deformity: Worsening of the toe's override, adduction, or rotation despite non-operative interventions.
- Fixed contractures: Lack of passive correctability of the MTP joint dorsiflexion or adduction contracture.
- Aesthetic concerns: While typically not the primary indication in isolation, significant cosmetic distress can contribute to the decision, especially in adolescents.
- Age: While there is no absolute age, surgical correction is generally deferred until the child is older than 3-4 years, to allow for some skeletal maturity and to ensure compliance with post-operative protocols. The natural history suggests that pain and shoe wear difficulties are more prevalent in children older than 10 years, making this an often appropriate age for intervention.
Contraindications
- Asymptomatic deformity in young children: When the deformity causes no functional or symptomatic issues, especially in very young children, observation with conservative measures is preferred.
- Mild, flexible deformities: If the toe is easily reducible and symptoms are well-controlled with conservative care, surgery is generally not indicated.
- Unrealistic patient/parent expectations: Thorough counseling on potential outcomes, risks, and recurrence rates is crucial.
- Active infection: Local or systemic infection must be resolved prior to surgery.
- Poor vascular status: Compromised circulation to the digit would contraindicate elective forefoot surgery.
- Coagulopathy or other significant medical comorbidities: These must be adequately managed prior to considering surgery.
The following table summarizes the typical operative versus non-operative indications:
| Category | Operative Indications | Non-Operative Indications |
|---|---|---|
| Symptoms | Persistent pain, painful dorsal callosities, recurrent irritation/blistering, ulceration | Asymptomatic, mild discomfort manageable with non-surgical means |
| Function | Difficulty with shoe wear, functional impairment due to toe malposition | No significant functional limitation |
| Deformity | Progressive deformity, fixed contracture refractory to conservative measures, severe rigid deformity | Mild, flexible deformity, responsive to taping/stretching, easily reducible |
| Age | Generally older children (>3-4 years), adolescents, and young adults; often indicated >10 years | Young children (<3-4 years) who are asymptomatic or have mild, flexible deformities |
| Prior Treatment | Failure of adequate trial of conservative management | Successful management with conservative approaches, initial presentation of a flexible deformity |
| MTP Joint | Dorsal dislocation/subluxation with significant contracture | Mild MTP joint dorsiflexion without significant subluxation |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is essential for a successful outcome following a Butler procedure.
Pre-Operative Assessment
- Clinical Examination: A thorough physical examination should assess the severity of the deformity, flexibility versus rigidity of the MTP joint, the presence of fixed contractures (MTP dorsiflexion, adduction, rotation), and the condition of the skin. Neurovascular status of the digit must be confirmed. Documenting the degree of dorsal override and medial deviation is critical.
-
Radiographic Evaluation:
Weight-bearing anteroposterior (AP) and lateral radiographs of the foot are typically obtained. These views help to:
- Assess the alignment of the fifth MTP joint and identify any dorsal subluxation or dislocation.
- Evaluate for osseous deformities or hypoplasia of the phalanges or metatarsal head.
- Rule out other pathologies.
- Stress views or oblique views may occasionally be helpful to characterize the flexibility or rotation.
-
Surgical Goals:
The primary goals of the Butler procedure are to:
- Reduce the MTP joint dislocation/subluxation.
- Correct the dorsiflexion and adduction contractures.
- Address the lateral rotation of the digit.
- Release the contracted skin in the fourth web space.
- Achieve a plantigrade, well-aligned fifth toe that can function without pain or shoe wear difficulties.
- Informed Consent: Comprehensive discussion with the patient and/or guardians regarding the procedure, expected outcomes, potential complications (recurrence, infection, stiffness, neurovascular injury), post-operative course, and alternative treatments is paramount. Specific attention should be paid to the potential for recurrence and the need for possible revision surgery.
- Pre-operative Markings: Prior to tourniquet inflation, the surgeon should mark the planned elliptical skin incision, typically centered over the dorsal aspect of the fifth MTP joint, extending into the fourth web space if significant skin contracture is present. The course of the neurovascular bundles should be anticipated.
Patient Positioning and Anesthesia
- Anesthesia: General anesthesia is commonly employed, especially in pediatric patients. Regional anesthesia (e.g., ankle block) can be used as an adjunct for post-operative pain control.
- Patient Positioning: The patient is positioned supine on the operating table.
- Tourniquet: A thigh tourniquet is applied to provide a bloodless field, which is crucial for precise dissection and identification of delicate structures. A well-padded tourniquet should be inflated after exsanguination of the limb.
- Foot Preparation and Draping: The affected foot and ankle are prepped with an antiseptic solution and sterilely draped, exposing the entire foot and distal leg up to the tourniquet. Care is taken to ensure free movement of the ankle and toes for intraoperative assessment.
Detailed Surgical Approach / Technique (Butler Procedure)
The Butler procedure is a versatile soft tissue release designed to correct the multiplanar deformity of the overlapping fifth toe. Its hallmark is the elliptical skin incision, which simultaneously releases contracted skin and provides access to underlying structures.
Step 1: Skin Incision and Elliptical Skin Excision
- A dorsal elliptical incision is made on the fifth toe, centered over the fifth MTP joint. The ellipse typically extends from the proximal phalanx, across the MTP joint, and onto the distal aspect of the fifth metatarsal. Crucially, the apex of the ellipse usually extends slightly into the fourth web space to address the skin contracture there and allow for future skin advancement. The width of the ellipse is determined by the severity of the skin contracture and the amount of redundant skin that needs to be removed to achieve a tension-free closure after reduction.
-
The elliptical skin segment is then carefully excised.
- Rationale: This elliptical excision serves a dual purpose: it removes the redundant, contracted dorsal skin that contributes to the override and creates a soft tissue defect that, when closed longitudinally, acts to pull the toe distally and plantarly, thereby correcting the dorsiflexion and adduction.
Step 2: Subcutaneous Dissection and Neurovascular Preservation
- Following skin excision, sharp and blunt dissection proceeds through the subcutaneous tissue.
- Crucial step: Meticulous care must be taken to identify and protect the dorsal digital neurovascular bundles to the fifth toe (medial branch from the fourth common digital nerve and artery, and lateral branch from the proper plantar digital nerve/artery or dorsal digital nerve). These structures typically lie along the dorsolateral and dorsomedial aspects of the toe. Retraction of these bundles should be gentle to prevent injury.
Step 3: Extensor Digitorum Longus (EDL) Tendon Lengthening
- The extensor digitorum longus (EDL) tendon to the fifth toe is identified. In cases of overlapping fifth toe, this tendon is often found to be taut and shortened, contributing significantly to the MTP joint dorsiflexion contracture and dislocation.
-
A
Z-plasty lengthening
of the EDL tendon is performed. The tendon is incised longitudinally for approximately 1-1.5 cm, and then transversely at opposing ends of the longitudinal cut, creating two flaps. This allows for lengthening of the tendon when the flaps are overlapped and sutured.
- Alternative: A simple tenotomy or partial tenotomy can be performed, but Z-plasty offers a more controlled lengthening and maintains tendon continuity, which is generally preferred to prevent extensor lag.
- Rationale: Lengthening the EDL releases the primary deforming force that causes dorsal subluxation of the MTP joint.
Step 4: Dorsal MTP Joint Capsulotomy and Release
- Deep to the EDL tendon, the dorsal aspect of the fifth MTP joint capsule is identified.
-
A
dorsal capsulotomy
is performed, often in a transverse or inverted V-shape, to release the tight dorsal capsule that is typically contracted and thickened. This release allows for the complete reduction of the MTP joint. Any remaining adhesions or restrictive soft tissues around the joint should be addressed.
- Rationale: The contracted dorsal capsule often prevents full plantarflexion and reduction of the MTP joint even after EDL lengthening.
Step 5: Adductor Release (Optional, but often necessary)
-
If a significant adduction contracture persists after the dorsal release and EDL lengthening, an
adductor tenotomy
of the fifth toe (if a discernible adductor digiti minimi tendon contribution is identified) or a release of the deep transverse metatarsal ligament (DTML) in the fourth web space may be performed. The medial collateral ligament of the MTP joint may also require release in resistant cases.
- Rationale: This addresses the medial deviation of the toe.
Step 6: MTP Joint Reduction and K-wire Fixation
- With all contractures released, the fifth MTP joint is manually reduced. The toe should now sit plantigrade and in line with the fifth metatarsal, with passive range of motion restored.
-
A
K-wire (usually 0.035 or 0.045 inch)
is typically inserted to maintain the corrected position. The K-wire can be inserted in an antegrade fashion from the tip of the toe, across the interphalangeal (IP) joints, and then retrograde across the MTP joint into the fifth metatarsal, ensuring the MTP joint is reduced and slightly plantarflexed. Alternatively, a transarticular K-wire can be inserted from the dorsal aspect of the metatarsal head, across the MTP joint, and into the proximal phalanx. The K-wire should be cut short and bent to prevent migration and skin irritation.
- Rationale: K-wire fixation maintains the reduction and allows soft tissues to heal in the corrected position, preventing early recurrence.
Step 7: Skin Closure
- The elliptical skin defect is closed longitudinally. This longitudinal closure, sometimes referred to as a V-Y advancement or Z-plasty modification depending on the incision geometry, creates a lengthening effect on the skin and helps to pull the toe distally and plantarly.
-
The skin edges are approximated meticulously with fine, absorbable sutures (e.g., 5-0 or 6-0 Monocryl or Vicryl Rapide) in a subcuticular fashion, followed by adhesive strips or non-absorbable sutures to the skin.
- Rationale: The tension generated by the skin closure further contributes to the overall correction, reinforcing the plantar and distal positioning of the toe. Proper closure is essential for wound healing and cosmetic outcome.
The third image provided is often associated with the surgical result or a different view of the deformity.

This image could represent a post-operative clinical view, demonstrating the corrected alignment after a Butler procedure, or perhaps a different intraoperative stage if the context were clearer. For the purpose of this surgical guide, if depicting a post-operative view, it would show the successful reduction and alignment of the fifth digit.
Adjunctive Procedures
In very severe or recurrent cases, or those with significant osseous deformity, adjunctive procedures might be considered, though less common with a primary Butler:
*
Proximal Phalanx Osteotomy:
For severe fixed rotation or angular deformity of the phalanx.
*
Distal Metatarsal Osteotomy:
Rarely indicated for fifth toe override, usually reserved for metatarsus adductus or bunionette deformities.
*
Skin grafting:
In rare instances of severe skin deficiency, though the elliptical excision and longitudinal closure usually suffice.
The Butler procedure, by addressing the skin, tendon, and capsular contractures, offers a comprehensive correction for the overlapping fifth toe with good reported outcomes.
Complications & Management
While the Butler procedure is generally considered safe and effective, like any surgical intervention, it carries potential risks and complications. Understanding these and their management strategies is crucial for surgeons.
Common Complications
-
Recurrence: This is arguably the most common and challenging complication. Despite adequate initial correction, the deformity can gradually return, particularly if initial soft tissue releases were insufficient or if the K-wire fixation was inadequate or removed prematurely.
- Incidence: Reported rates vary widely, from 5% to 20% in different series.
- Management: For mild, flexible recurrence, conservative measures like taping and stretching can be re-attempted. For significant, symptomatic, or rigid recurrence, revision surgery may be necessary. Revision may involve more extensive soft tissue releases, a repeat EDL Z-plasty, capsulotomy, adductor release, or in some cases, an additional osteotomy (e.g., proximal phalanx closing wedge osteotomy) or even fusion of the MTP joint in older, refractory cases, although fusion is rare for this condition.
-
Undercorrection/Overcorrection:
- Incidence: Low, but possible.
- Management: Undercorrection may present similarly to recurrence and often requires revision surgery if symptomatic. Overcorrection (e.g., a "curly toe" appearance or malalignment in the opposite direction) is less common with the Butler procedure but can occur with overly aggressive skin excision or soft tissue release. Mild cases may improve with stretching; severe cases may require soft tissue balancing or osteotomy.
-
Infection: Superficial or deep wound infection.
- Incidence: Low, typically <5%.
- Management: Superficial infections usually respond to oral antibiotics and local wound care. Deep infections, especially around K-wires, may require intravenous antibiotics, K-wire removal, and surgical debridement.
-
Neurovascular Injury: Damage to the dorsal digital nerves or arteries.
- Incidence: Rare with meticulous dissection and identification of neurovascular structures.
- Management: Careful identification and protection are paramount. If identified intraoperatively, primary repair may be indicated. Post-operative numbness or vascular compromise requires observation; severe ischemia mandates immediate re-exploration and vascular consultation.
-
Stiffness/Adhesions: Restricted MTP joint range of motion.
- Incidence: Common to some degree, often mild and transient.
- Management: Early initiation of passive and active range of motion exercises post-K-wire removal, along with physical therapy, can help restore mobility. In rare cases, manipulation under anesthesia or arthroscopic lysis of adhesions may be considered.
-
Painful Scar:
- Incidence: Low.
- Management: Scar massage, silicone sheeting, and topical steroids can help improve scar quality. Revision scar excision may be considered for severe, symptomatic keloids or hypertrophic scars, though recurrence risk exists.
-
K-wire Related Issues: K-wire breakage, migration, skin irritation, or localized infection.
- Incidence: Low.
- Management: Prompt removal of the K-wire, local wound care, and antibiotics if infection is present. Careful K-wire insertion and bending reduce the risk of migration and irritation.
-
Vascular Compromise/Toe Ischemia: Extremely rare, but a serious complication.
- Incidence: Very rare.
- Management: Immediate removal of any constrictive dressings or K-wires. Assessment of toe perfusion. May require immediate vascular consultation and re-exploration to identify and address the cause (e.g., vessel injury, severe hematoma).
-
Swelling/Edema: Common post-operatively.
- Incidence: Common (transient).
- Management: Elevation of the foot, compression dressings, and early mobilization help to minimize and resolve post-operative swelling.
The following table summarizes common complications and their management:
| Complication | Incidence | Management/Salvage Strategy |
|---|---|---|
| Recurrence | 5-20% | Conservative (taping, stretching) for mild; Revision surgery (extended releases, osteotomy, fusion) for severe/symptomatic. |
| Undercorrection/Overcorrection | Low | Observation for mild; Revision surgery for significant symptomatic malalignment. |
| Infection | <5% | Oral/IV antibiotics, local wound care; Debridement and K-wire removal for severe cases. |
| Neurovascular Injury | Rare | Meticulous dissection for prevention; Observation for mild neuropathy; Surgical repair or neurolysis for significant injury. |
| Stiffness/Adhesions | Common | Early range of motion exercises, physical therapy; Manipulation under anesthesia or arthroscopic lysis for severe cases. |
| Painful Scar | Low | Scar massage, silicone sheeting; Revision scar excision for severe, symptomatic scars. |
| K-wire Related Issues | Low | K-wire removal, antibiotics if infection; Careful insertion to prevent migration/breakage. |
| Vascular Compromise (Toe Ischemia) | Very Rare | Immediate removal of constrictive elements (dressing, K-wire); Vascular consultation; Re-exploration. |
| Swelling/Edema | Common | Elevation, compression, early mobilization. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for achieving optimal functional outcomes and minimizing the risk of complications following a Butler procedure. The protocol is typically structured around protection, controlled mobilization, and progressive weight-bearing.
Immediate Post-Operative Phase (Days 0-3 weeks)
-
Dressing and Splinting:
- A sterile, non-adherent dressing is applied to the wound.
- A soft, well-padded compression dressing is then applied, which may be incorporated into a posterior splint or a surgical shoe. The dressing should provide gentle support without causing undue pressure or vascular compromise.
- The K-wire, if used, should be visible and protected.
- Elevation and Ice: Strict elevation of the operative limb above heart level is maintained for the first 48-72 hours to minimize swelling and pain. Intermittent application of ice packs (with a barrier) to the dressing can also aid in edema control.
- Pain Management: A multi-modal analgesic regimen, including NSAIDs, acetaminophen, and short-term opioids as needed, should be implemented. Regional nerve blocks can provide excellent initial post-operative analgesia.
- Weight-Bearing: Non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) with crutches or a knee scooter is typically prescribed for the first 2-3 weeks, or until K-wire removal. A post-operative shoe or boot may be used for protection during transfers.
- Wound Care: The dressing is typically changed by the surgeon or a qualified nurse at 7-10 days, at which point the wound is inspected for signs of infection or complications. The K-wire site should be cleaned with antiseptic solution at each dressing change.
Intermediate Phase (3-6 weeks)
- K-wire Removal: K-wires are generally removed at 3 to 4 weeks post-operatively, once sufficient soft tissue healing and stability are achieved. This is typically done in the clinic setting.
-
Initiation of Range of Motion (ROM):
- Following K-wire removal, gentle active and passive range of motion exercises for the fifth MTP and IP joints are immediately initiated. The goal is to prevent stiffness and restore mobility.
- Patients are instructed on self-stretching exercises to maintain the corrected alignment and counteract any tendency for recurrence of contracture (e.g., plantarflexion of the MTP joint, abducting the toe).
-
Progressive Weight-Bearing:
- Once the K-wire is removed, progressive weight-bearing in a stiff-soled shoe or post-operative boot is commenced, as tolerated. The duration of boot use can vary but typically ranges from 2-4 weeks after K-wire removal.
- Physical Therapy: Referral to physical therapy may be beneficial, particularly for patients with persistent stiffness, gait abnormalities, or difficulty regaining full function. Therapists can guide ROM exercises, strengthening, and gait training.
- Shoe Wear: Patients transition to a wide, comfortable, soft-soled shoe as swelling subsides and comfort allows, typically around 6-8 weeks post-op.
Advanced Phase (6 weeks - 3 months and beyond)
- Full Activity Resumption: Gradual return to full activities, including sports, is typically permitted by 3 months post-operatively, provided there is no pain, swelling, or residual deformity.
- Long-Term Monitoring: Patients should be monitored for signs of recurrence, which can occur even years after surgery. Regular follow-up appointments should be scheduled to assess alignment, function, and scar quality.
- Custom Orthotics/Toe Spacers: In some cases, custom orthotics or silicone toe spacers may be recommended for long-term support and to prevent recurrence, particularly during high-impact activities or prolonged shoe wear.
The specific timing and progression of rehabilitation may be modified based on individual patient healing, the complexity of the initial deformity, and any intraoperative findings or post-operative complications. Patient compliance with the rehabilitation protocol is paramount for a successful long-term outcome.
Summary of Key Literature / Guidelines
The Butler procedure has a long history in the surgical management of the overlapping fifth toe, evolving from its initial description in 1952. Its enduring popularity stems from its comprehensive approach to correcting the multiplanar deformity by addressing skin, tendon, and capsular contractures.
Historical Context and Evolution
Early surgical interventions for overlapping fifth toe were often limited to simple skin excisions or tendon lengthenings, leading to high recurrence rates. Butler's contribution was significant in recognizing the interplay of skin contracture, EDL shortening, and dorsal MTP joint capsular tightening. The elliptical skin incision with longitudinal closure, combined with EDL Z-plasty and dorsal capsulotomy, became the cornerstone of the technique, providing a more stable and lasting correction.
Comparison to Other Techniques
Numerous other surgical techniques exist for overlapping fifth toe, each with its proponents and specific indications:
*
Lapidus Procedure:
Originally described for bunion correction, a modified Lapidus procedure involves a dorsal V-Y plasties of skin and capsule combined with an EDL tenotomy and dorsal capsulotomy. It is often cited as an alternative to Butler, sharing many principles. Some literature suggests similar efficacy between Butler and Lapidus, with outcomes largely dependent on thoroughness of soft tissue release.
*
V-Y Skin Plasty:
Simple V-Y skin advancements are used, often combined with tendon and capsular releases. These techniques aim to lengthen the dorsal skin and allow plantar displacement of the toe.
*
Z-Plasty of Skin:
Similar to V-Y plasties, Z-plasty techniques can be used to lengthen contracted skin, particularly in the web space.
*
Isolated EDL Lengthening/Tenotomy and Capsulotomy:
While these are components of the Butler, performing them in isolation without addressing the skin contracture often leads to recurrence.
*
Phalangeal or Metatarsal Osteotomies:
In cases of severe, rigid osseous deformity, or failure of soft tissue procedures, osteotomies (e.g., closing wedge osteotomy of the proximal phalanx or distal metatarsal osteotomy) may be considered, but they are more invasive and typically reserved for older adolescents or adults with significant structural abnormalities.
*
Fusion of the MTP Joint:
Rarely indicated for this condition, but an option for severe, painful, and recalcitrant deformities in older individuals where all other methods have failed.
Evidence for Efficacy and Outcomes
Contemporary literature generally supports the Butler procedure as a reliable option for correction of overlapping fifth toe, particularly in pediatric and adolescent populations.
*
High Success Rates:
Studies often report high patient satisfaction and good functional outcomes, with reported success rates ranging from 80% to 95%.
*
Recurrence:
As noted, recurrence remains the most significant complication, with rates varying depending on the study population, follow-up duration, and surgical technique. A systematic review by authors like Fallat and Fallat (2007) highlighted the variability but generally supported the efficacy of soft tissue procedures.
*
Age and Timing:
Most studies suggest better outcomes when performed after 3-4 years of age, to allow for sufficient toe size and patient compliance, and often around 8-12 years when symptoms become more pronounced. Early intervention in infancy is generally reserved for very severe or rapidly progressing deformities.
*
Comprehensive Release:
The key message from the literature is the importance of a comprehensive release of all deforming forces—skin, EDL, and dorsal MTP joint capsule—to minimize recurrence. Simply addressing one component is insufficient.
Current Guidelines and Consensus
There is a general consensus that:
* Conservative management should be the first line of treatment, especially in younger, asymptomatic individuals.
* Surgical intervention is indicated for symptomatic deformities that fail conservative management or for progressive, rigid deformities.
* The Butler procedure, or similar comprehensive soft tissue releases (like the modified Lapidus), remains the workhorse procedure.
* Meticulous technique, particularly protection of neurovascular structures and adequate release of all contracted tissues, is paramount.
* Post-operative immobilization with K-wires for 3-4 weeks is standard practice to allow for stable healing in the corrected position.
* Patient and parent counseling regarding potential for recurrence and the need for prolonged follow-up is essential.
Future Directions
Research continues to explore long-term recurrence rates, refine surgical techniques for resistant cases, and investigate the role of genetics in recurrence. The advent of minimally invasive techniques for soft tissue release is also an area of ongoing investigation, although open techniques remain the gold standard for robust correction. The emphasis remains on understanding the individual patient's specific anatomical deformities to tailor the surgical approach, ensuring all deforming forces are effectively neutralized.
Clinical & Radiographic Imaging


