Bunionette (Tailor's Bunion): Comprehensive Evaluation and Surgical Management
Key Takeaway
A bunionette, or Tailor’s bunion, is a painful lateral prominence of the fifth metatarsal head. Often associated with splayfoot, it results from structural abnormalities such as an increased 4-5 intermetatarsal angle or lateral bowing of the fifth metatarsal shaft. Management begins with shoe modification and orthotics. Refractory cases require surgical intervention, including lateral condylectomy, distal chevron osteotomy, or diaphyseal osteotomy, tailored to the specific radiographic classification of the deformity.
Introduction and Pathoanatomy
The bony prominence on the lateral aspect of the fifth metatarsal head is classically referred to as a bunionette or tailor’s bunion. The historical nomenclature derives from the traditional cross-legged sitting posture of tailors, which forced the lateral border of the foot against the floor, leading to chronic friction, bursal hypertrophy, and localized pain.
While historical occupational hazards highlighted the condition, modern understanding attributes the bunionette deformity to a combination of intrinsic biomechanical derangements and extrinsic compressive forces (primarily constricting footwear). It is frequently observed in conjunction with a splayfoot deformity and hallux valgus. The underlying pathoanatomy may involve a congenitally enlarged fifth metatarsal head, traumatic hypertrophy, lateral bowing of the metatarsal shaft, or an abnormal divergence of the fifth metatarsal from the fourth metatarsal.
Clinical Pearl: A bunionette is rarely an isolated soft-tissue anomaly. It is almost universally accompanied by underlying structural deviations of the fifth ray. Successful management dictates that the surgeon addresses the specific osseous deformity rather than merely excising the prominent soft tissue.
Clinical Evaluation
Patient Presentation
Patients typically present with localized pain, erythema, and swelling over the lateral eminence of the fifth metatarsophalangeal (MTP) joint. Constricting shoes with a narrow toe box are the primary source of discomfort. Chronic irritation over the bony prominence frequently leads to the development of an adventitial bursa, which can become inflamed, hypertrophic, and occasionally infected.
In advanced or neglected cases, ulceration may ensue. The abnormal pressure distribution often results in an intractable plantar keratosis (IPK) or a diffuse callus.

FIGURE 83-44 Callus beneath fifth metatarsal head. If an extension deformity is present at the fifth metatarsophalangeal joint, a painful callus may develop beneath the fifth metatarsal head.
High-Risk Populations
Special consideration must be given to patients with compromised sensibility or vascularity. In patients with diabetes mellitus, advanced Charcot-Marie-Tooth disease, or spinal dysraphism, the combination of a prominent bunionette, repetitive microtrauma, and peripheral neuropathy can lead to devastating complications. A simple bursal ulceration can rapidly progress to deep space infection, osteomyelitis, and ultimately necessitate the amputation of the entire fifth ray or even a broader partial foot amputation.
Radiographic Evaluation
Standard weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot are mandatory for the accurate assessment of a bunionette deformity. The AP radiograph is utilized to measure several critical angles that dictate surgical decision-making.
Key Radiographic Parameters
- 4-5 Intermetatarsal Angle (IMA): Formed by the intersection of the longitudinal axes of the fourth and fifth metatarsals.
- Normal: Less than 8 degrees.
- Pathologic: Greater than 8 degrees indicates pathological divergence of the fifth ray.
- Fifth Metatarsophalangeal (MTP-5) Angle: Formed by the longitudinal axis of the fifth metatarsal and the longitudinal axis of the proximal phalanx of the fifth toe.
- Pathologic: Usually greater than 14 degrees in symptomatic patients.
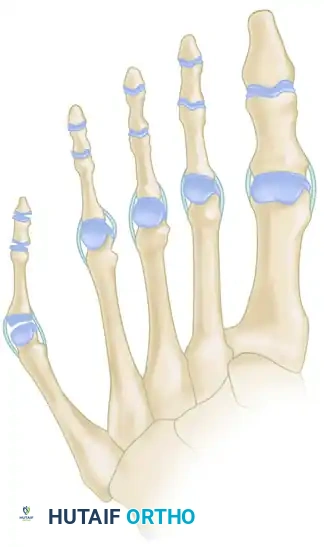
FIGURE 83-40 Measurement of metatarsophalangeal-5 and 4-5 intermetatarsal angles for evaluation of bunionette deformity.
- Lateral Deviation Angle (LDA): This angle evaluates the intrinsic bowing of the fifth metatarsal shaft. It is formed by a line bisecting the metatarsal head and neck intersecting with a line drawn parallel to the medial cortex of the proximal fifth metatarsal shaft.
- Normal: Approximately 2.6 degrees.
- Pathologic: Averages 8 degrees in patients with a symptomatic bunionette.

FIGURE 83-42 Measurement of lateral deviation angle in the evaluation of bunionette deformity.
Classification of Bunionette Deformity
The classification system proposed by Cohen and Nicholson is the most widely accepted framework for categorizing bunionette deformities. It is based entirely on the structural radiographic appearance of the fifth metatarsal and directly guides surgical intervention.
Type I: Enlarged Metatarsal Head
Type I is characterized by an isolated enlargement or lateral prominence of the fifth metatarsal head. The 4-5 IMA and the lateral deviation angle remain within normal limits. This is often described as a "dumbbell-shaped" metatarsal head.

FIGURE 83-41A Type I, lateral prominence of the metatarsal head.
Type II: Lateral Bowing of the Metatarsal Shaft
Type II features an abnormal lateral bend or bowing of the distal third of the fifth metatarsal shaft. The 4-5 IMA is normal, but the Lateral Deviation Angle (LDA) is significantly increased.

FIGURE 83-41B Type II, lateral bowing of the fifth metatarsal.
Type III: Widened 4-5 Intermetatarsal Angle
Type III is the most common variant. It is characterized by a divergent fifth metatarsal shaft resulting in an increased 4-5 IMA (greater than 8 degrees). This divergence significantly widens the forefoot (splayfoot).

FIGURE 83-41C Type III, widening of the 4-5 intermetatarsal angle.
Surgical Warning: Misclassifying a Type III deformity as a Type I and performing a simple lateral condylectomy will inevitably lead to recurrent symptoms, as the underlying divergent structural pathology (the widened IMA) has not been addressed.
Conservative Management
Non-operative treatment is the first line of management for all bunionette deformities and focuses on accommodating the deformity and relieving pressure.
- Footwear Modification: The cornerstone of conservative care. Patients must transition to shoes with a wide toe box and soft, accommodating upper materials.
- Orthotic Devices: Metatarsal pads or bars can help offload the fifth metatarsal head. Semirigid shoe inserts with a specific relief (or "well") beneath the plantar aspect of the condyle are highly effective for patients with an associated intractable plantar keratosis.
- Padding: The application of 1/8- to 1/4-inch foam rubber or silicone padding between the bony prominence and the shoe can provide immediate symptomatic relief.
- Callus Care: Routine debridement of hypertrophic calluses or IPKs by a podiatrist or orthopedic specialist.
Surgical Indications and Decision Making
Surgical intervention is indicated only when exhaustive conservative measures fail to relieve pain and the deformity interferes with the patient's activities of daily living or ability to wear standard footwear.
The choice of surgical procedure is dictated by the Cohen classification:
1. Type I Deformity: Lateral condylectomy (partial head resection).
2. Type II Deformity: Distal metatarsal osteotomy (e.g., Chevron) or diaphyseal osteotomy to correct the lateral bowing.
3. Type III Deformity: Proximal or diaphyseal osteotomy to reduce the widened 4-5 IMA.
4. Salvage: Resection of the fifth metatarsal head is reserved for severe degenerative joint disease, chronic infection, or non-reconstructable deformities in low-demand patients.
Surgical Techniques
1. Lateral Condylectomy (Partial Metatarsal Head Resection)
Indications: Strictly reserved for symptomatic Type I deformities (hypertrophic lateral condyle with normal 4-5 IMA and normal LDA).
Positioning and Anesthesia:
The patient is placed supine. A regional ankle block or local Mayo block is typically sufficient, supplemented with monitored anesthesia care (MAC). A calf or ankle tourniquet is utilized for hemostasis.
Surgical Approach:
1. Make a 3- to 4-cm dorsolateral longitudinal incision centered over the fifth MTP joint.
2. Carefully dissect through the subcutaneous tissue. Pitfall: Identify and protect the dorsal cutaneous branches of the sural nerve and the proper digital nerve to the fifth toe. Retract these neurovascular structures dorsally or plantarward as dictated by the exposure.
3. Perform a longitudinal capsulotomy of the fifth MTP joint. Reflect the capsule to expose the lateral eminence of the metatarsal head.
Bone Resection:
1. Using a microsaw or sharp osteotome, resect the prominent lateral third of the fifth metatarsal head. The cut should be made in line with the lateral cortex of the metatarsal shaft.
2. Crucial Step: If the patient has an associated plantar callus, the plantar aspect of the metatarsal head must also be resected to decompress the plantar skin. Bevel the plantar-lateral aspect smoothly.

FIGURE 83-46 The plantar aspect of the fifth metatarsal head should be removed in addition to the lateral flare to address plantar keratosis.

Surgical Diagram: Resection of the lateral flare of the fifth metatarsal head.
Closure:
1. Smooth all bony edges with a rasp.
2. Irrigate the joint copiously.
3. Perform a capsulorrhaphy. Plicate the lateral capsule to correct any residual medial deviation of the fifth toe.
4. Close the skin with non-absorbable sutures.
2. Distal Metatarsal Osteotomy (Chevron Osteotomy)
Indications: Mild to moderate Type II or Type III deformities. It allows for medial translation of the metatarsal head, effectively reducing the lateral prominence and mildly decreasing the 4-5 IMA.
Technique:
1. Utilize the same dorsolateral approach and capsulotomy as described above.
2. Resect the lateral eminence (condylectomy) to create a flat surface.
3. Create a V-shaped osteotomy (Chevron) in the distal metatarsal neck. The apex of the osteotomy should point distally, with the dorsal and plantar arms diverging at approximately 60 degrees.
4. Translate the capital fragment medially by 3 to 5 mm (up to 50% of the bone width).
5. Fix the osteotomy with a single 0.045-inch Kirschner wire (K-wire) or a low-profile 2.0 mm titanium screw.
6. Resect the overhanging medial bony prominence of the proximal fragment.
7. Close the capsule and skin in layers.
3. Diaphyseal Osteotomy of the Fifth Metatarsal
Indications: Severe Type II (severe lateral bowing) and severe Type III (4-5 IMA > 12 degrees) deformities. A diaphyseal osteotomy provides greater corrective power for large intermetatarsal angles compared to distal osteotomies.
Technique:
1. Make a longitudinal incision over the midshaft of the fifth metatarsal.
2. Elevate the periosteum minimally to preserve the blood supply to the diaphysis.
3. Perform an oblique or step-cut (scarf-type) osteotomy in the diaphysis. An oblique osteotomy running from distal-lateral to proximal-medial allows for smooth medial translation and rotation of the distal fragment.
4. Translate the distal fragment medially to close the 4-5 IMA.
5. Secure the osteotomy rigidly. Given the diaphyseal location, fixation with two low-profile cortical screws or a specialized locking plate is preferred to prevent rotational instability and nonunion.
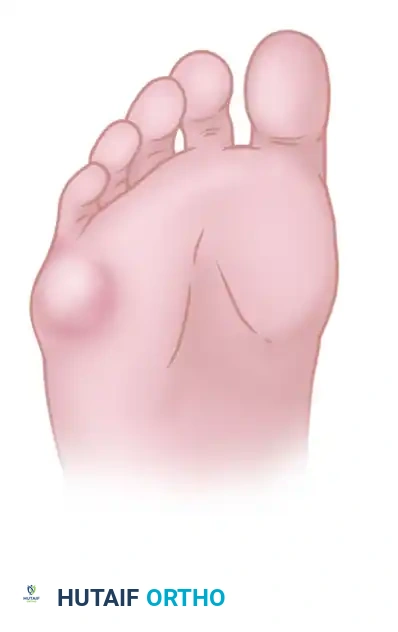
FIGURE 83-45 Diaphyseal osteotomy for metatarsus quintus varus. This provides powerful correction for severe Type II and Type III deformities.
4. Resection of the Fifth Metatarsal Head
Indications: This is a salvage procedure. It is indicated in elderly, low-demand patients with severe rheumatoid arthritis, chronic osteomyelitis of the metatarsal head, or severe degenerative joint disease where joint preservation is impossible.
Technique:
1. Expose the MTP joint via a dorsolateral approach.
2. Perform a complete transverse osteotomy at the surgical neck of the fifth metatarsal.
3. Excise the metatarsal head.
4. Smooth the distal stump of the metatarsal shaft meticulously to prevent a new pressure prominence.
5. Interpose the joint capsule over the bony stump if possible.
Surgical Warning: Routine resection of the fifth metatarsal head in young, active patients is strongly discouraged. It frequently leads to transfer metatarsalgia (increased pressure under the fourth metatarsal head), retraction of the fifth toe, and significant cosmetic deformity.
Postoperative Protocol
The postoperative rehabilitation protocol varies based on the surgical procedure performed:
- Lateral Condylectomy / Head Resection: Patients may bear weight as tolerated immediately postoperatively in a rigid-soled postoperative shoe. Sutures are removed at 14 days. Transition to wide, comfortable athletic shoes occurs at 3 to 4 weeks.
- Distal Osteotomy (Chevron): Heel-weight-bearing or flat-foot weight-bearing in a rigid postoperative shoe or controlled ankle motion (CAM) boot is permitted. Active and passive range of motion (ROM) of the MTP joint begins at 2 weeks to prevent stiffness. Radiographic union is typically observed at 6 weeks, at which point transition to normal footwear begins.
- Diaphyseal Osteotomy: Due to the cortical nature of the bone and higher risk of delayed union, patients are typically kept strictly non-weight-bearing or touch-down weight-bearing for 4 to 6 weeks in a short leg cast or CAM boot. Full weight-bearing is resumed only after radiographic evidence of bridging callus is confirmed.
Complications
Orthopedic surgeons must be vigilant regarding potential complications following bunionette correction:
- Recurrence: The most common complication, almost exclusively resulting from choosing an inadequate procedure (e.g., performing a simple condylectomy for a Type III deformity).
- Nonunion/Delayed Union: More common with diaphyseal osteotomies due to the watershed blood supply of the fifth metatarsal shaft. Meticulous surgical technique and rigid fixation mitigate this risk.
- Transfer Metatarsalgia: Can occur if the fifth metatarsal is excessively shortened or elevated during osteotomy, shifting weight-bearing forces to the fourth metatarsal head.
- Nerve Injury: Iatrogenic injury to the dorsal cutaneous branch of the sural nerve leads to painful neuromas.
- Avascular Necrosis (AVN): Excessive soft tissue stripping around the metatarsal head during distal osteotomies can compromise the vascular supply, leading to AVN of the capital fragment.
Conclusion
The successful management of a bunionette deformity requires a thorough understanding of the underlying biomechanics and precise radiographic evaluation. While conservative measures remain the first line of defense, surgical intervention is highly successful when the procedure is accurately matched to the specific pathoanatomy outlined by the Cohen classification. Meticulous surgical execution and adherence to postoperative protocols ensure optimal functional outcomes and high patient satisfaction.
📚 Medical References
- bunionette deformity, Instr Course Lect 39:37, 1990.
- Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair, Foot Ankle 11:195, 1991.
- Diebold PF: Basal osteotomy of the fi fth metatarsal for the bunionette, Foot Ankle 12:74, 1991.
- Diebold PF, Bejjani FJ: Basal osteotomy of the fi fth metatarsal with intermetatarsal pinning: a new approach to tailor’s bunion, Foot Ankle 8:40, 1987.
- Holmes GB Jr: Surgical management of foot disorders: bunions and bunionettes, Curr Opin Rheumatol 3:98, 1991.
- Karasick D: Preoperative assessment of symptomatic bunionette deformity: radiologic fi ndings, AJR Am J Roentgenol 164:147, 1995.
- Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: long-term follow-up, Foot Ankle 11:345, 1991.
- Kitaoka HB, Holiday AD Jr: Lateral condylar resection for bunionette, Clin Orthop Relat Res 278:183, 1992.
- Kitaoka HB, Holiday AD Jr, Campbell DC II: Distal chevron metatarsal osteotomy for bunionette, Foot Ankle 12:80, 1991.
- Kitaoka HB, Leventen EO: Medial displacement metatarsal osteotomy for treatment of painful bunionette, Clin Orthop Relat Res 243:172, 1989.
- Konradsen L, Neilsen PT: Distal metatarsal osteotomy for bunionette deformity, J Foot Surg 27:493, 1988.
- Moran MM, Claridge RJ: Chevron osteotomy for bunionette, Foot Ankle Int 15:684, 1994.
- Nestor BJ, Kitaoka HB, Ilstrup DM, et al: Radiologic anatomy of the painful bunionette, Foot Ankle 11:6, 1990.
- Steinke MS, Boll KL: Hohmann-Thomasen metatarsal osteotomy for tailor’s bunion (bunionette), J Bone Joint Surg 71A:423, 1989.
You Might Also Like

