SURGICAL ANATOMY OF THE BRACHIAL PLEXUS
The brachial plexus is a highly complex neural network responsible for the motor and sensory innervation of the upper extremity. A profound understanding of its three-dimensional anatomy is the cornerstone of accurate clinical diagnosis and successful surgical reconstruction.
The plexus is formed by the union of the anterior rami of the lower four cervical nerves (C5, C6, C7, C8) and the first thoracic nerve (T1). Anatomical variations are common; a "prefixed" plexus receives significant contributions from C4, while a "postfixed" plexus receives fibers from T2. Shortly after exiting the intervertebral foramen, each root receives its sympathetic component via a gray ramus communicans. The cervical roots receive their sympathetic fibers from the lower cervical sympathetic ganglia, whereas the T1 root receives fibers from its own sympathetic ganglion after contributing a white ramus to it.
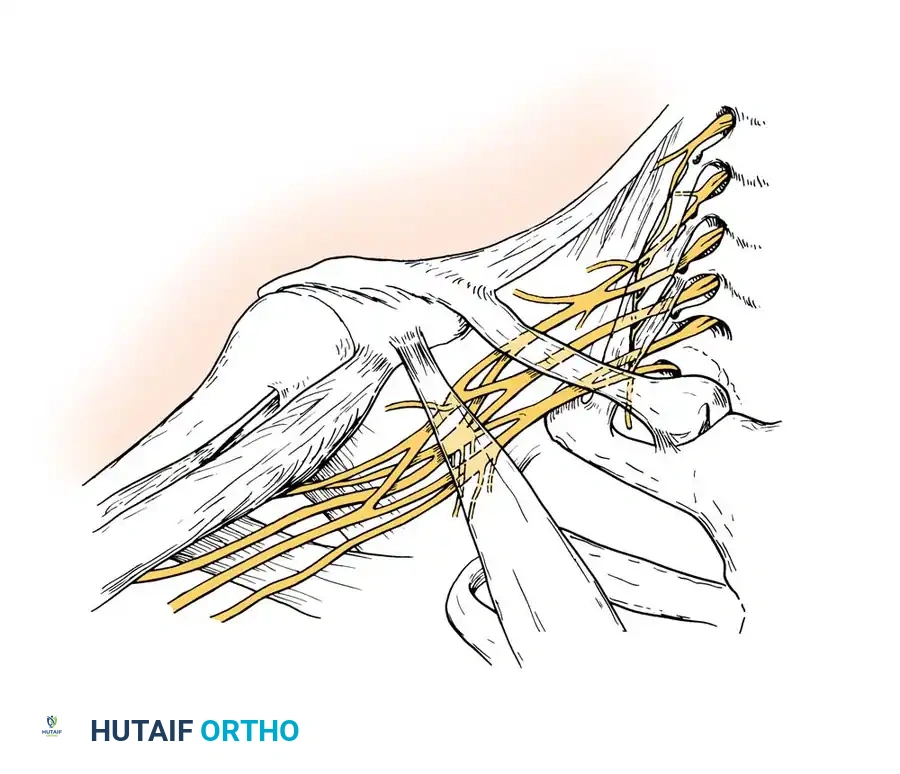
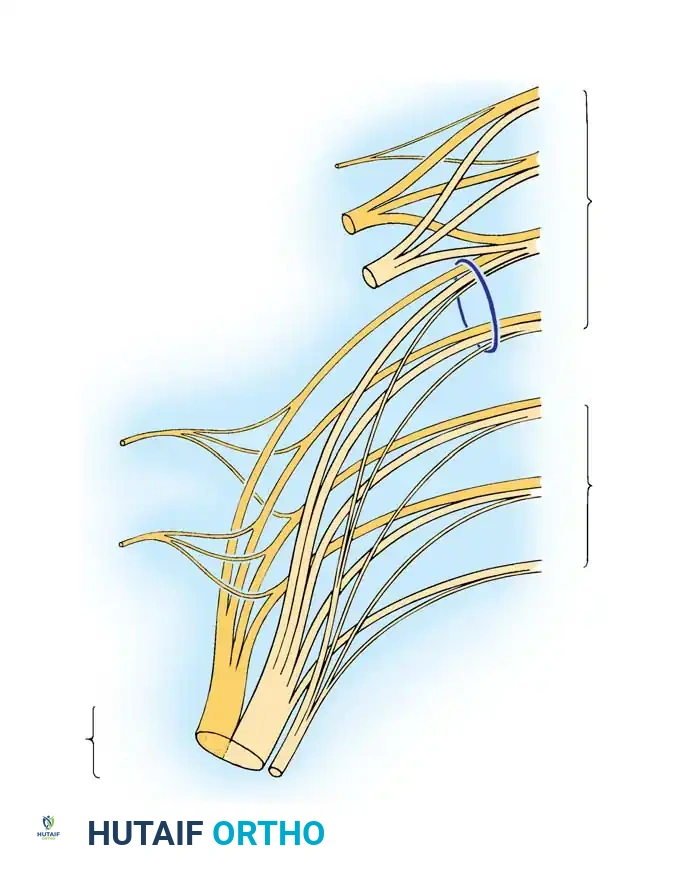
Fig. 59-17: Schematic representation of the Brachial Plexus, illustrating the roots, trunks, divisions, cords, and terminal branches.
Trunks, Divisions, and Cords
The formation of the brachial plexus begins just distal to the scalene muscles in the posterior triangle of the neck.
* Upper Trunk: Formed by the union of the C5 and C6 roots.
* Middle Trunk: Formed by the continuation of the C7 root alone.
* Lower Trunk: Formed by the union of the C8 and T1 roots.
These three trunks proceed inferolaterally behind the clavicle. As they pass through the cervicoaxillary canal, each trunk divides into anterior and posterior divisions, reflecting the evolutionary separation of flexor and extensor muscle group innervation.
* Posterior Cord: Formed by the union of all three posterior divisions.
* Lateral Cord: Formed by the union of the anterior divisions of the upper and middle trunks.
* Medial Cord: Formed by the continuation of the anterior division of the lower trunk.
These cords embrace the axillary artery, and their nomenclature (lateral, posterior, medial) is derived strictly from their anatomical relationship to this vessel.
Surgically Significant Branches
Understanding the precise origin of peripheral branches is critical for localizing lesions:
* Branches from the Roots: The long thoracic nerve (C5, C6, C7) arises immediately after the roots emerge from the foramina, traversing posterior to the plexus to innervate the serratus anterior. The dorsal scapular nerve (C5) arises lateral to the long thoracic contribution, innervating the levator scapulae and rhomboids.
* Branches from the Trunks: The only surgically significant branch here is the suprascapular nerve, arising from the upper trunk. It passes through the suprascapular notch to supply the supraspinatus and infraspinatus.
* Branches from the Cords:
* Lateral Cord: Lateral pectoral nerve, musculocutaneous nerve, and the lateral root of the median nerve.
* Medial Cord: Medial pectoral nerve, medial brachial cutaneous, medial antebrachial cutaneous, ulnar nerve, and the medial root of the median nerve.
* Posterior Cord: Upper and lower subscapular nerves, thoracodorsal nerve, axillary nerve, and the radial nerve.
Clinical Pearl: The dorsal scapular and long thoracic nerves are the only nerves that leave the roots before their union to form the trunks. Preservation of rhomboid and serratus anterior function in the presence of severe distal deficits strongly suggests a postganglionic lesion distal to the nerve roots.
ETIOLOGY AND CLASSIFICATION OF INJURIES
Brachial plexus injuries are broadly categorized into open and closed trauma. In military combat, penetrating wounds from high-velocity missiles or shrapnel cause the majority of injuries. In civilian populations, traction injuries dominate.
According to Narakas, approximately 70% of traumatic brachial plexus injuries occur secondary to motor vehicle accidents, with 70% of those involving motorcycles or bicycles. The mechanism typically involves a high-energy fall where the shoulder is violently depressed while the head and neck are forced in the opposite direction, applying massive traction to the plexus.
Associated Injuries
Severe polytrauma is present in 80% of patients with brachial plexus injuries. Surgeons must maintain a high index of suspicion for:
* Vascular Compromise: Rupture or intimal tearing of the subclavian or axillary artery occurs in up to 20% of patients.
* Fractures: Proximal humerus, scapula, clavicle, ribs, and cervical transverse processes.
* Joint Dislocations: Glenohumeral, acromioclavicular, and sternoclavicular joints.
* Soft Tissue: Massive rotator cuff tears are frequently associated with upper trunk traction injuries in older adults.
Classification Systems
While the Seddon and Sunderland classifications (neuropraxia, axonotmesis, neurotmesis) describe the microscopic nerve injury, clinical classifications focus on the anatomical level. The Leffert classification categorizes injuries by mechanism and level. More commonly, injuries are divided into:
1. Upper Plexus Injuries (Erb-Duchenne): Involving C5-C6 (+/- C7).
2. Lower Plexus Injuries (Klumpke): Involving C8-T1.
3. Total Plexus Injuries: Involving C5-T1, often presenting with a completely flail, anesthetic limb.
DIAGNOSIS AND CLINICAL EVALUATION
Accurate localization of the lesion—specifically differentiating between preganglionic (root avulsion) and postganglionic (rupture) injuries—is the most critical step in management, as true root avulsions are not amenable to direct surgical repair.
Clinical Syndromes
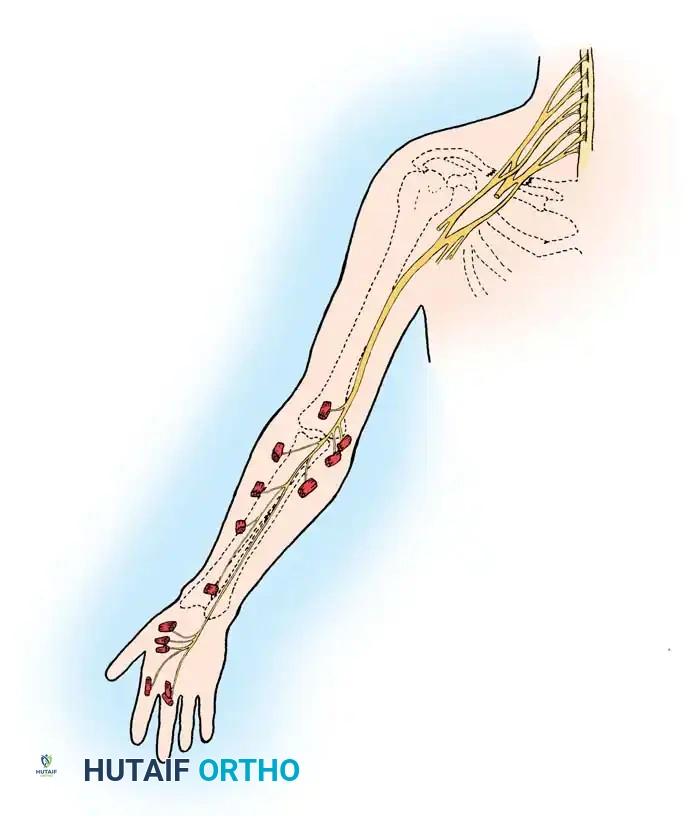
Upper Plexus Injury (Erb's Palsy):
Involves segments innervated by C5 and C6. The patient presents with the classic "waiter's tip" posture: the limb is extended at the elbow, flaccid at the side, adducted, and internally rotated.
* Motor Deficits: Abduction is impossible (deltoid, supraspinatus paralysis). External rotation is absent (infraspinatus, teres minor). Active elbow flexion is lost (biceps, brachialis, brachioradialis). Supination is impossible.
* Sensory Deficits: Anesthesia over the deltoid and the lateral aspect of the forearm and hand.
Lower Plexus Injury (Klumpke's Palsy):
Involves C8 and T1. The primary dysfunction manifests in the intrinsic musculature of the hand (claw hand deformity) along with paralysis of the wrist and finger flexors. Sensory deficits track along the medial aspect of the arm, forearm, and hand.
Surgical Warning: The presence of Horner syndrome (ptosis, miosis, anhidrosis) strongly indicates a preganglionic avulsion of the T1 root, as the sympathetic ganglion is disrupted near the spinal cord.
Cord Syndromes:
* Lateral Cord: Paralysis of the biceps, flexor carpi radialis, and pronator teres. Glenohumeral subluxation may occur.
* Posterior Cord: Inability to internally rotate the shoulder (subscapularis, teres major), elevate the limb (deltoid), or extend the elbow, wrist, and fingers (radial nerve distribution).
* Medial Cord: Combined ulnar and median nerve motor deficits (excluding FCR and pronator teres) with extensive medial sensory loss.
Advanced Diagnostic Modalities
1. Imaging (MRI and CT Myelography):
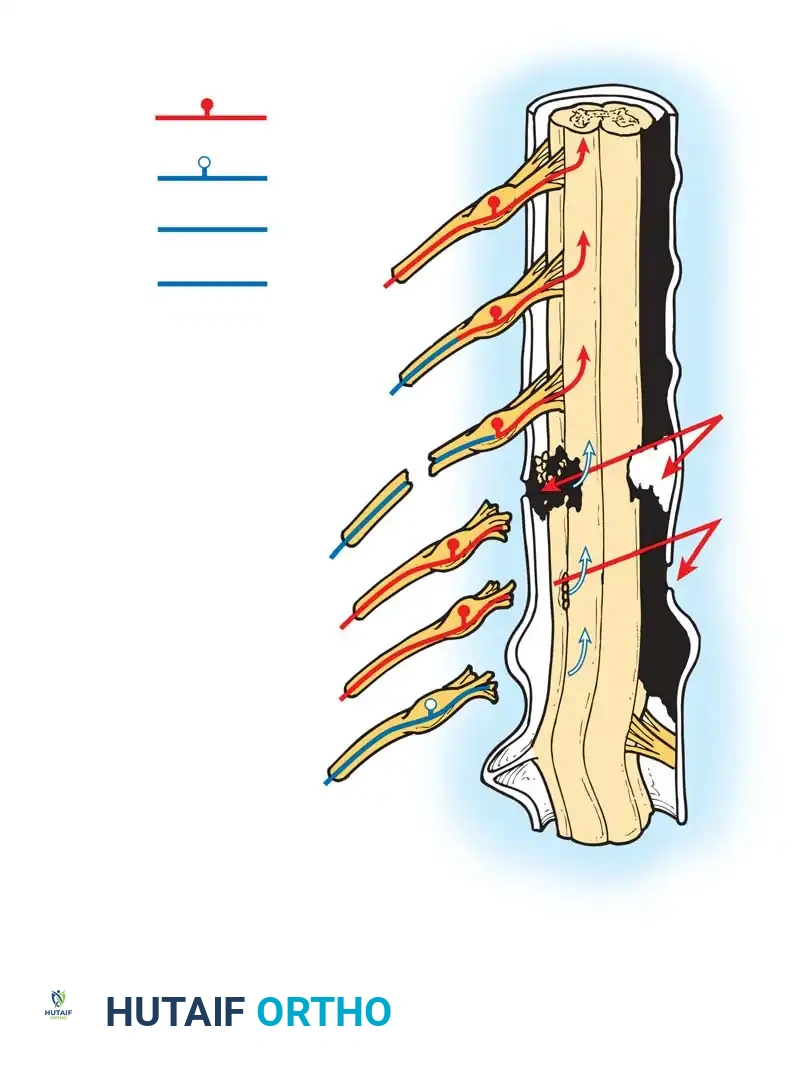
Historically, Pantopaque myelography was utilized to visualize pseudomeningoceles—extravasations of cerebrospinal fluid indicating root avulsion. Rorabeck and Harris noted that 31 of 34 patients with pseudomeningoceles showed no spontaneous recovery. Today, high-resolution MRI is the gold standard, offering superior visualization of the roots, trunks, and cords, as well as surrounding soft tissue edema and neuromas. CT myelography remains highly accurate (75% correlation with intraoperative findings) but should be delayed 6 to 12 weeks post-injury to prevent clotted blood from obscuring pseudomeningoceles.
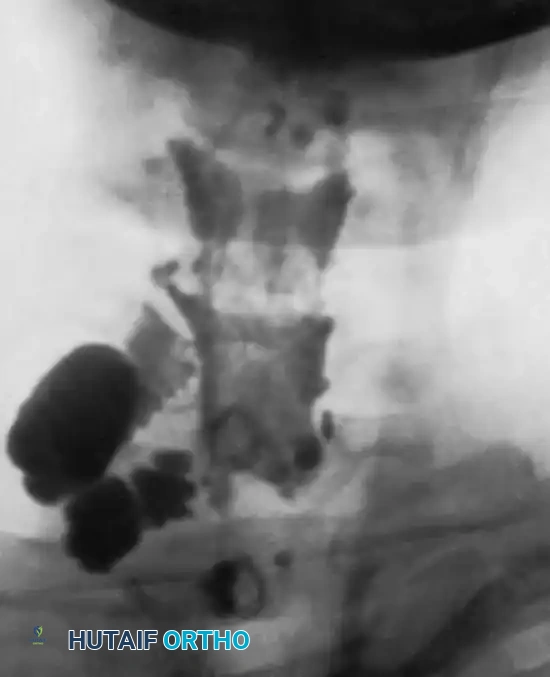
Fig. 59-18: Myelogram demonstrating a massive pseudomeningocele produced by avulsion of the C7 and C8 roots.
2. Electrodiagnostic Studies (EMG/NCS):
EMG is invaluable but must be timed appropriately (3-4 weeks post-injury) to allow for Wallerian degeneration. Denervation potentials in the segmental paraspinous musculature (innervated by posterior primary rami) confirm a preganglionic root avulsion.
3. Histamine Axon Reflex Test:
This test differentiates preganglionic from postganglionic lesions. A drop of histamine is scratched into the skin. A normal response (vasodilation, wheal, and flare) in an anesthetic dermatome indicates an intact sensory pathway from the skin to the dorsal root ganglion, proving the lesion is proximal to the ganglion (preganglionic avulsion). Absence of the flare response indicates a postganglionic injury, which may be surgically repairable.
INDICATIONS FOR SURGERY AND TIMING
The surgical management of brachial plexus injuries requires meticulous patient selection.
Open Injuries
When the plexus is injured by sharp objects (e.g., stab wounds, glass) and the patient's hemodynamic status permits, immediate exploration and primary repair are indicated. However, if there is concomitant life-threatening vascular or thoracic injury, those take precedence. In such cases, the orthopedic surgeon should briefly inspect the plexus, tag the severed neural elements with non-absorbable epineurial sutures (e.g., 6-0 Prolene), and place a Silastic sheet to separate the nerves from vascular repairs. This prevents severe scarring and facilitates a safer secondary reconstruction.
Closed Traction Injuries
For closed injuries, immediate surgery is rarely indicated unless there is an expanding hematoma or vascular compromise. A period of clinical observation (3 to 6 weeks) is standard. During this time, baseline neurological deficits are documented, and EMG is obtained.
* If clinical exam and imaging suggest a postganglionic rupture without spontaneous recovery by 3 months, exploration and nerve grafting are indicated.
* If imaging confirms multi-root avulsions, early nerve transfer (neurotization) is indicated to restore critical functions (elbow flexion and shoulder abduction) before irreversible motor endplate atrophy occurs (typically 12-18 months).
SURGICAL APPROACHES AND TECHNIQUES
Surgical exploration of the brachial plexus is a formidable undertaking requiring extensive extensile exposures, microsurgical instrumentation, and intraoperative nerve stimulation.
Patient Positioning and Preparation
The patient is placed in the supine position with a sandbag under the ipsilateral scapula. The head is turned to the contralateral side. The entire upper extremity, neck, and ipsilateral chest are prepped and draped free to allow intraoperative manipulation and observation of muscle contractions during nerve stimulation. Both lower extremities are prepped for potential sural nerve graft harvesting.
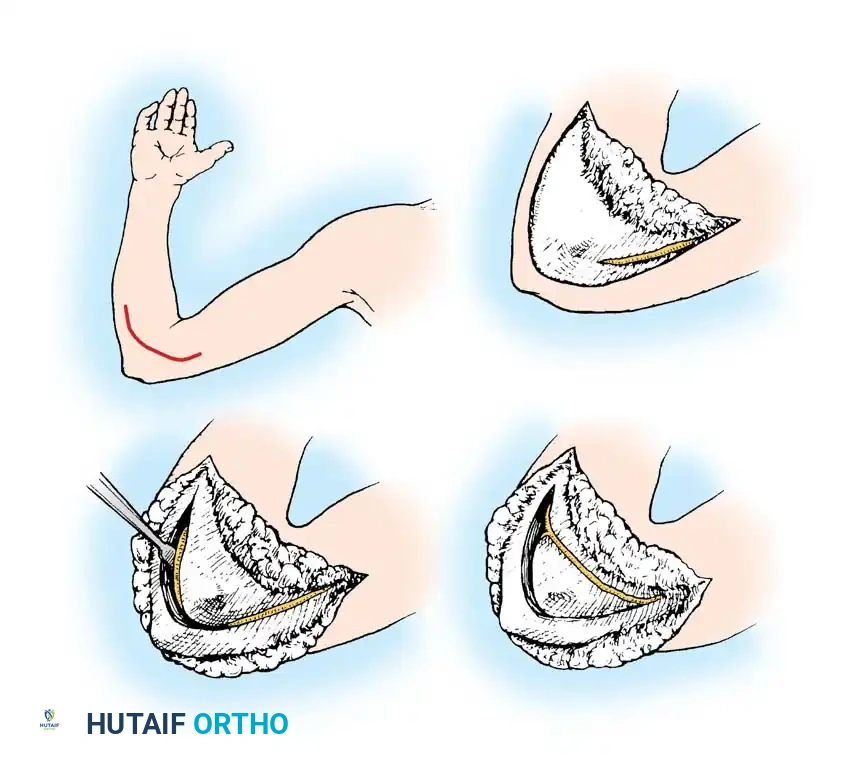
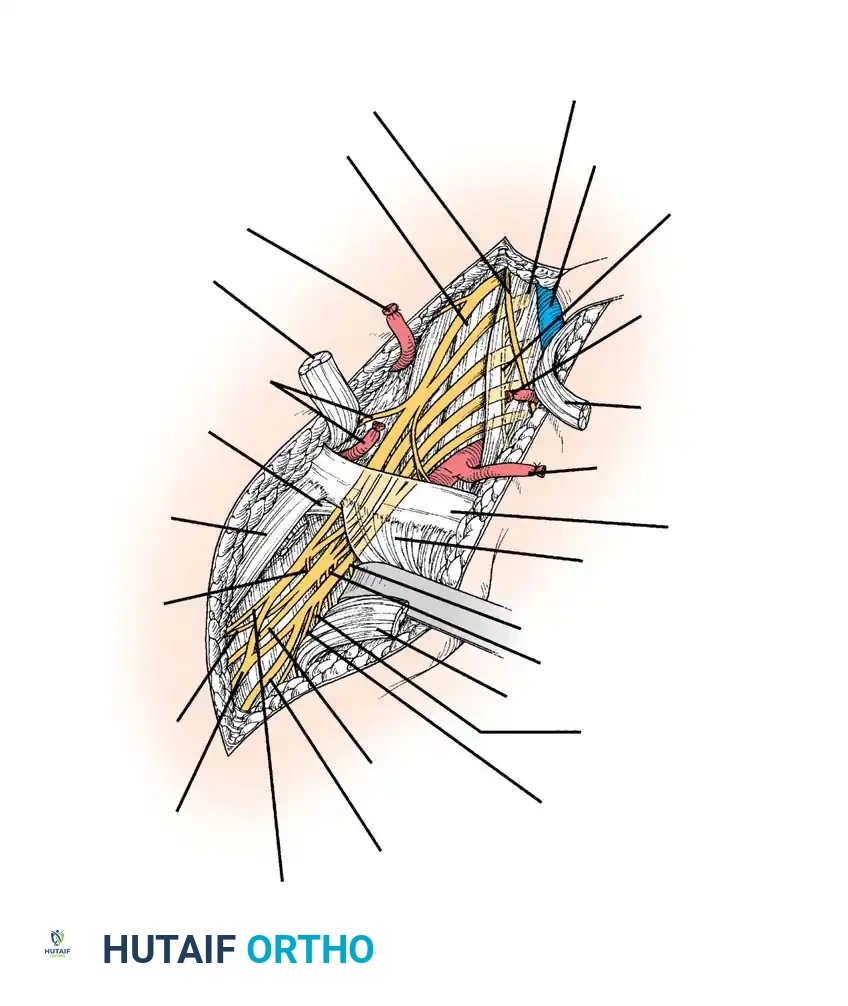
The Supraclavicular Approach
This approach is utilized for exploring the roots and trunks.
1. Incision: A zigzag or L-shaped incision is made along the posterior border of the sternocleidomastoid (SCM) muscle, extending laterally parallel to the clavicle.
2. Dissection: The platysma is divided. The external jugular vein is ligated or retracted. The omohyoid muscle is identified and divided.
3. Identification of Landmarks: The transverse cervical and suprascapular vessels are identified and protected. The anterior scalene muscle is exposed.
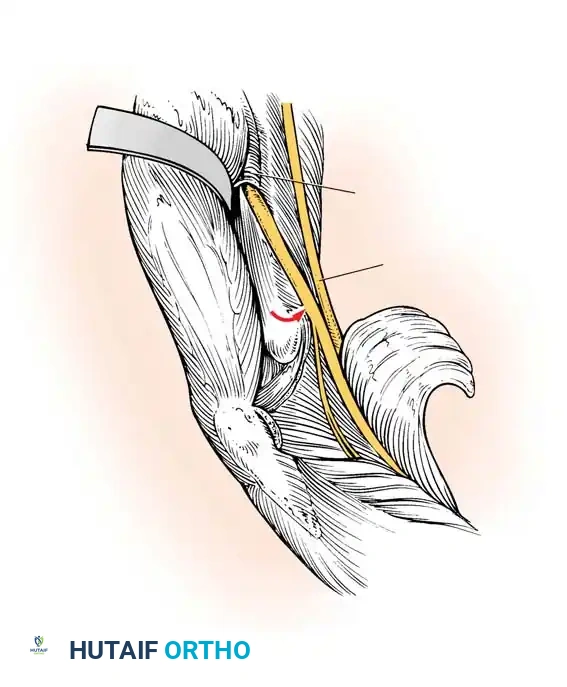
4. Phrenic Nerve Protection: The phrenic nerve courses from lateral to medial across the anterior surface of the anterior scalene. It must be meticulously identified, stimulated, and protected.
5. Plexus Exposure: The anterior scalene can be divided to fully expose the underlying roots (C5-C8) and trunks. The C5 root is traced proximally to the intervertebral foramen.
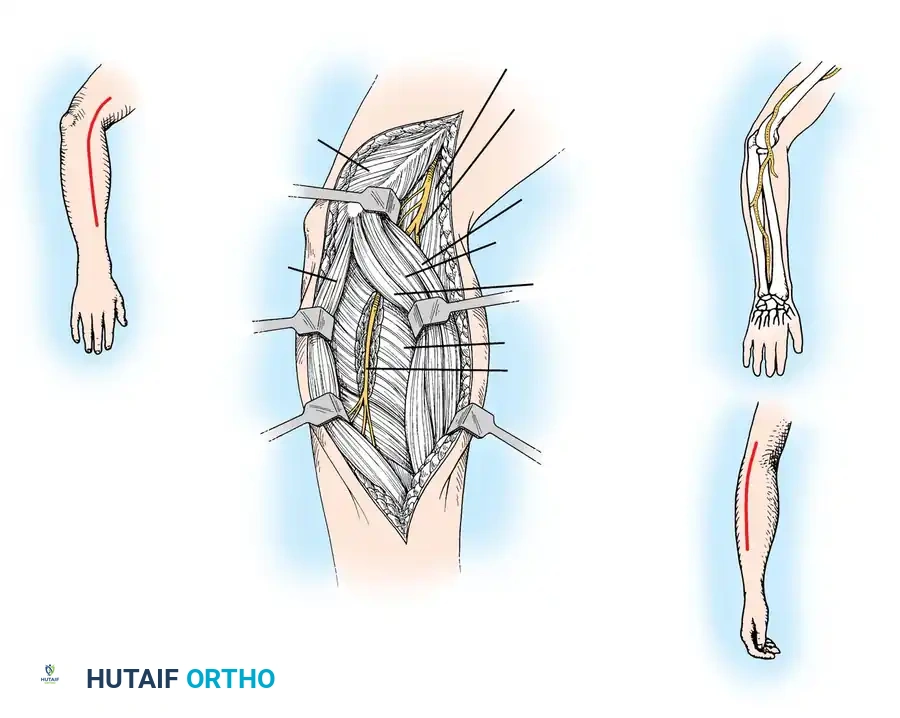
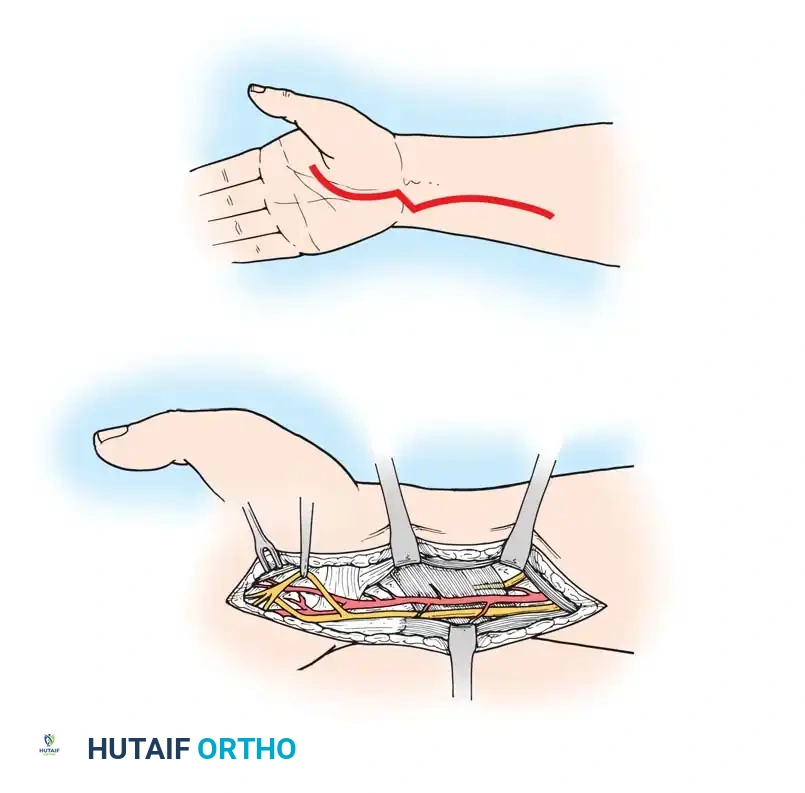
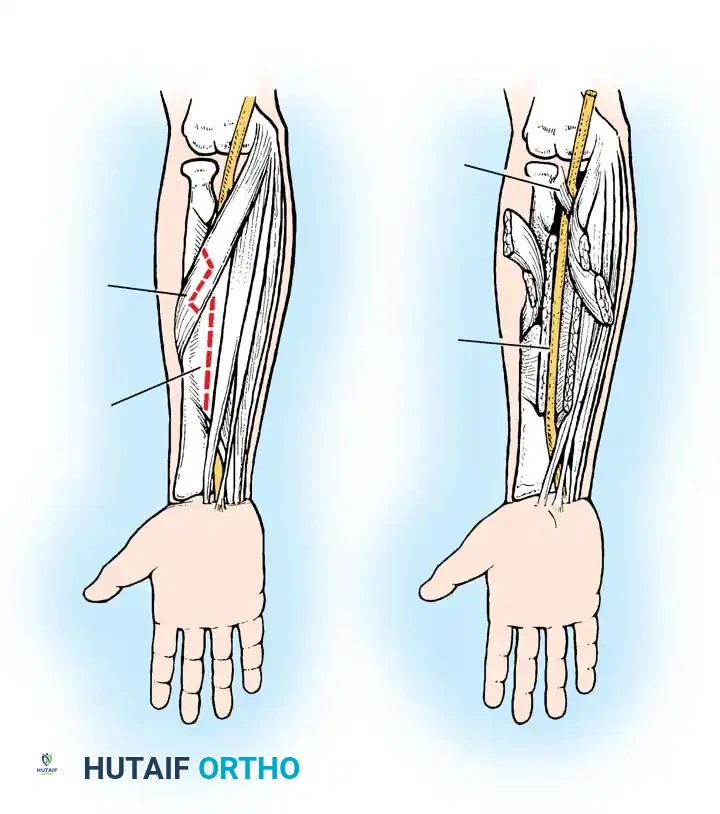
The Infraclavicular Approach
Used for exploring the divisions, cords, and terminal branches.
1. Incision: The supraclavicular incision is extended distally across the clavicle into the deltopectoral groove.
2. Clavicular Osteotomy (Optional): While routine osteotomy is avoided due to nonunion risks, it may be necessary for massive scarring. Alternatively, working above and below the clavicle is preferred.
3. Pectoralis Division: The pectoralis major is retracted or its clavicular insertion divided. The pectoralis minor is divided at its coracoid insertion to expose the neurovascular bundle.
4. Cord Identification: The axillary artery is the primary landmark. The lateral, posterior, and medial cords are identified based on their relationship to the artery.
Reconstructive Techniques
1. Neurolysis:
Indicated for lesions in continuity (neuroma-in-continuity) where intraoperative nerve action potentials (NAPs) demonstrate conduction across the scar. External neurolysis frees the nerve from surrounding scar bed, while internal neurolysis separates individual fascicles.
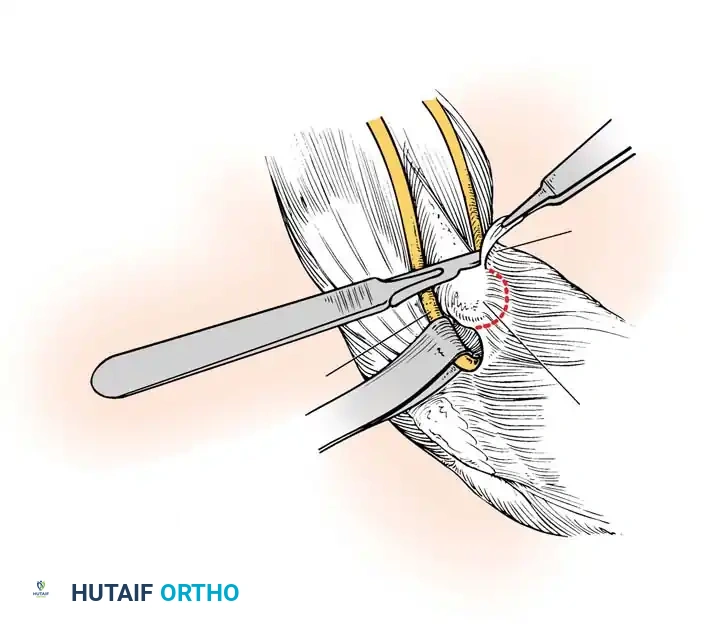
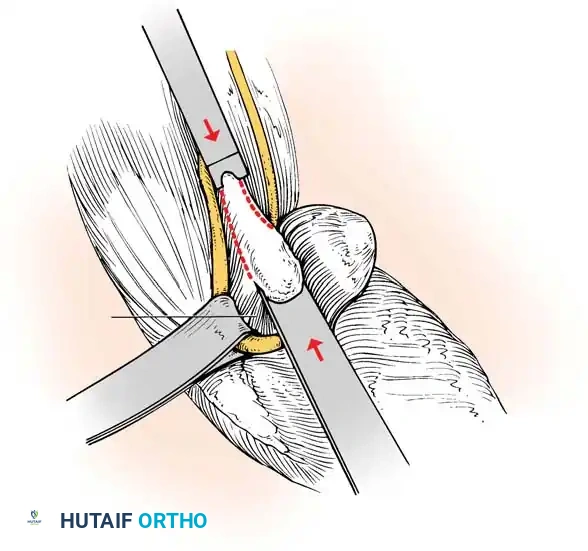
2. Interfascicular Nerve Grafting:
When a postganglionic rupture is identified, the neuroma is resected back to healthy fascicles (visualized under the operating microscope). Direct end-to-end repair is rarely possible without tension. Autogenous interfascicular nerve grafts, most commonly harvested from the sural nerve, are used to bridge the defect. Fibrin glue or 8-0 to 10-0 nylon sutures are used for coaptation.
3. Nerve Transfers (Neurotization):
In cases of preganglionic root avulsion, no proximal nerve stump is available. Expendable donor nerves are transferred to critical distal motor targets.
* Spinal Accessory Nerve (CN XI) to Suprascapular Nerve: Restores shoulder abduction and external rotation.
* Intercostal Nerves to Musculocutaneous Nerve: Restores elbow flexion.
* Oberlin Transfer: Transfer of a fascicle of the ulnar nerve to the biceps motor branch, highly effective for restoring elbow flexion in upper trunk avulsions.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of brachial plexus reconstruction relies heavily on strict postoperative management and prolonged rehabilitation.
- Immobilization: Postoperatively, the limb is immobilized in a sling and swathe or a custom orthosis for 3 to 4 weeks. This prevents tension on the delicate microsurgical nerve coaptations or grafts.
- Passive Range of Motion (ROM): Once immobilization is discontinued, aggressive passive ROM exercises are initiated to prevent joint contractures, particularly at the shoulder and elbow. A stiff joint will negate the benefits of a successful nerve recovery.
- Electrical Stimulation and Biofeedback: While the efficacy of direct electrical muscle stimulation remains debated, biofeedback is highly beneficial once early reinnervation potentials are detected.
- Long-Term Monitoring: Nerve regeneration occurs at approximately 1 mm per day (1 inch per month). Patients must be counseled that functional recovery may take 12 to 24 months. Serial clinical examinations and EMGs are required to track the advancing Tinel's sign and motor unit potentials.
Surgical Pitfall: Failure to manage patient expectations is a common error. Patients must understand that the goal of surgery is to restore functional utility (e.g., elbow flexion, shoulder stability, protective sensation), not to return the limb to its pre-injury normal state.
In conclusion, the management of brachial plexus injuries demands a rigorous, evidence-based approach. From the initial clinical evaluation and advanced imaging to the execution of complex microsurgical reconstructions, the orthopedic surgeon must navigate intricate anatomy to optimize the patient's functional outcome. Isolated upper trunk injuries generally carry the best prognosis, whereas complete avulsions require innovative nerve transfer strategies to salvage limb function.
📚 Medical References
- brachial plexus injuries, Orthopedics 9:899, 1986.
- Michelow BJ, Clarke HM, Curtis CG, et al: The natural history of obstetrical brachial plexus palsy, Plast Reconstr Surg 93:675, 1994.
- Millesi H: Surgical management of brachial plexus injuries, J Hand Surg 2:367, 1977.
- Narakas A: Brachial plexus surgery, Orthop Clin North Am 12:303, 1981.
- Narakas A: The treatment of brachial plexus injuries, Int Orthop 9:29, 1985.
- Narakas AO: Injuries to the brachial plexus. In Bora FW Jr, ed: The pediatric upper extremity: diagnosis and management, Philadelphia, 1986, Saunders. Pagnotta A, Haerle M, Gilbert A: Long-term results on abduction and external rotation of the shoulder after latissimus dorsi transfer for sequelae of obstetric palsy, Clin Orthop Relat Res 426:199, 2004.
- Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy, J Bone Joint Surg 80A:659, 1998.
- Perry J, Hsu J, Barber L, Hoffer M: Orthoses in patients with brachial plexus injuries, Arch Phys Med Rehabil 55:132, 1974.
- Riordan DC: Tendon transplantation in median nerve and ulnar nerve paralysis, J Bone Joint Surg 35A:312, 1953.
- Rogers MH: An operation for the correction of deformity due to obstetrical paralysis, Boston Med Surg J 174:163, 1916.
- Seddon HJ: Brachial plexus injuries, J Bone Joint Surg 31B:3, 1949.
- [Seddon HJ: Lesions of individual nerves: upper limb. In Seddon HJ, ed: Surgical disorders of the peripheral nerves, Churchill Livingstone, 1949, London.
Sever JW: The results of a new operation for obstetrical paralysis, Am J Orthop Surg 16:248, 1918.](https://pubmed.ncbi.nlm.nih.gov/?term=Seddon%20HJ%3A%20Lesions%20of%20individual%20nerves%3A%20upper%20limb.%20In%20Seddon%20HJ%2C%20ed%3A%20Surgical%20disorders%20of%20the%20peripheral%20nerves%2C%20Churchill%20Livingstone%2C%201949%2C%20London.%0A%0ASever%20JW%3A%20The%20results%20of%20a%20new%20operation%20for%20obstetrical%20paralysis%2C%20Am%20J%20Orthop%20Surg%2016%3A248%2C%201918.)
- Sever JW: Obstetric paralysis, JAMA 85:1862, 1925.
- Sever JW: Obstetrical paralysis, Surg Gynecol Obstet 44:547, 1927.
- Solonen KA, Telaranta T, Ryöppy S: Early reconstruction of birth injuries of the brachial plexus, J Pediatr Orthop 1:367, 1981.
- Sugioka H: Evoked potentials in the investigation of traumatic lesions of the peripheral nerve and the brachial plexus, Clin Orthop Relat Res 184:85, 1984.
- Sunderland S: Nerves and nerve injuries, 2nd ed, New York, 1978, Churchill Livingstone. Tada K, Tsuyuguchi Y, Kawai H: Birth palsy: natural recovery course and combined root avulsion, J Pediatr Orthop 4:279, 1984.
- Terzis JK, Liberson WT, Levine R: Obstetric brachial plexus palsy, Hand Clin 2:773, 1986.
- Terzis JK, Vekris MD, Okajima S, et al: Shoulder deformities in obstetric brachial plexus paralysis: a computed tomography study, J Pediatr Orthop 23:254, 2003.
- Van der Sluijs JA, van Ouwerkerk WJR, de Gast A, et al: Treatment of internal rotation contracture of the shoulder in obstetric brachial plexus lesions by subscapular tendon lengthening and open reduction: early results and complications, J Pediatr Orthop 13B:218, 2004.
- Waters PM: Comparison of the natural history, the outcome of microsurgical repair, and the outcome of operative reconstruction in brachial plexus birth palsy, J Bone Joint Surg 81A:649, 1999.
- Waters PM: The upper limb. In Morrissy RT, Weinstein SL, eds: Lovell and Winter’s pediatric orthopaedics, Philadelphia, 2001, Lippincott Williams & Wilkins. Waters PM, Peljovich AE: Shoulder reconstruction in patients with chronic brachial plexus birth palsy, Clin Orthop Relat Res 364:144, 1999.
- Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy, J Bone Joint Surg 80A:668, 1998.
- Wickstrom J: Birth injuries of the brachial plexus: treatment of defects in the shoulder, Clin Orthop 23:187, 1962.
- Zancolli EA: Classifi cation and management of the shoulder in birth palsy, Orthop Clin North Am 12:433, 1980.
