Comprehensive Orthopedic Review | Dr Hutaif General Ort -...
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Comprehensive Introduction and Patho-Epidemiology
The proximal femur represents one of the most biomechanically demanding regions of the human skeleton, subjecting both the developing physis and the mature osseous architecture to immense multi-planar forces. Pathologies affecting this region, particularly those driven by extreme shear forces, demand a rigorous understanding of both mechanical and biological principles. This chapter provides an exhaustive review of two paradigmatic conditions affecting the proximal femur across different age spectrums: high-energy vertically oriented femoral neck fractures (Pauwels type III) in young adults, and Slipped Capital Femoral Epiphysis (SCFE) in the pediatric and adolescent populations. By synthesizing these entities, we elucidate the fundamental orthopedic principles of shear force neutralization, epiphyseal stabilization, and vascular preservation.
Femoral neck fractures in young adults typically result from high-energy mechanisms, such as motor vehicle collisions or falls from significant heights. Unlike the osteoporotic fractures seen in the geriatric population, which often result from low-energy torsional forces, young adult femoral neck fractures are frequently vertically oriented. These fractures, classified as Pauwels type III, are characterized by a fracture line angle exceeding 50 degrees relative to the horizontal plane. Epidemiologically, these injuries carry a disproportionately high rate of complications, including nonunion and avascular necrosis (AVN), primarily due to the conversion of axial physiological loads into devastating shear forces across the fracture interface. The preservation of the native femoral head is paramount in this demographic, necessitating anatomically precise reduction and mechanically robust fixation strategies that can withstand these extreme forces.
Conversely, Slipped Capital Femoral Epiphysis (SCFE) represents the most common hip disorder in adolescents, with an incidence ranging from 1 to 10 per 100,000 children. The pathophysiology of SCFE involves a mechanical failure of the proximal femoral physis, specifically within the hypertrophic zone, allowing the epiphysis to displace posteriorly and inferiorly relative to the metaphysis. While obesity and the adolescent growth spurt are the most common mechanical drivers, a critical subset of patients presents with underlying endocrinopathies or metabolic disorders. Conditions such as chronic kidney disease (renal osteodystrophy), hypothyroidism, and panhypopituitarism profoundly weaken the physeal architecture. In these atypical presentations—such as a 12-year-old obese male with chronic kidney disease—the risk of bilateral involvement approaches 100%, making the prophylactic stabilization of the contralateral, asymptomatic hip a mandatory consideration.
The intersection of these two distinct clinical entities lies in their shared biomechanical vulnerability to shear stress and the catastrophic consequences of vascular disruption. Whether addressing a traumatic vertical shear fracture in a 28-year-old or an impending physeal slip in a metabolically compromised adolescent, the orthopedic surgeon must deploy fixation constructs that neutralize deforming forces while meticulously protecting the tenuous extraosseous and intraosseous blood supply to the femoral head.
Detailed Surgical Anatomy and Biomechanics
Osteovascular Anatomy of the Proximal Femur
A profound comprehension of the proximal femoral vascular anatomy is non-negotiable for the orthopedic surgeon, as iatrogenic or traumatic disruption dictates the catastrophic complication of avascular necrosis. The primary blood supply to the mature femoral head is derived from the medial femoral circumflex artery (MFCA), a branch of the profunda femoris. The MFCA courses posteriorly, giving rise to the critical lateral epiphyseal artery system (retinacular vessels) that penetrates the capsule at the intertrochanteric line and travels along the posterosuperior femoral neck. In pediatric patients, the vascular anatomy is further complicated by the presence of the physis, which acts as a barrier to intraosseous collateral circulation. The ligamentum teres provides a variable, often negligible, contribution to the epiphysis in both adolescents and adults. Any surgical approach, capsulotomy, or hardware placement must meticulously respect the posterosuperior trajectory of these retinacular vessels.
Biomechanics of Pauwels Type III Fractures
The biomechanical environment of the proximal femur is governed by the joint reaction force, which is approximately 2.5 to 3 times body weight during normal ambulation. Friedrich Pauwels astutely recognized that the orientation of the femoral neck fracture line dictates the mechanical forces experienced at the fracture site. In Pauwels type I and II fractures (less than 30 degrees and 30-50 degrees, respectively), axial loading generates primarily compressive forces, which promote primary bone healing and construct stability. However, in Pauwels type III fractures (greater than 50 degrees), the physics are inverted. The joint reaction force is resolved almost entirely into shear stress and varus-inducing bending moments.
When multiple parallel cancellous screws are utilized for a Pauwels type III fracture, the construct relies solely on the friction generated by interfragmentary compression. Because the fracture is nearly vertical, physiological loading causes the proximal fragment to slide inferiorly along the fracture plane, leading to rapid varus collapse, hardware failure, and nonunion. Therefore, neutralizing these massive shear forces requires a fixed-angle device, such as a sliding hip screw (SHS) or a cephalomedullary nail. A fixed-angle construct acts as a mechanical buttress, converting the deleterious shear forces into stabilizing compressive forces along the axis of the implant, thereby preventing vertical displacement and varus angulation.
Biomechanics of Slipped Capital Femoral Epiphysis
The biomechanical failure in SCFE occurs at the microstructural level within the physis. During the adolescent growth spurt, the physis widens and the perichondrial ring—a vital stabilizing structure—thins and weakens. The proximal femoral physis normally transitions from a horizontal orientation to a more oblique, vertical orientation during adolescence, increasing its exposure to shear forces. When the mechanical load (exacerbated by obesity) exceeds the structural integrity of the hypertrophic zone, or when metabolic derangements (such as the altered calcium-phosphate metabolism in chronic kidney disease) intrinsically weaken the cartilage matrix, the epiphysis slips. The goal of in situ pinning is not to compress the physis, but to provide a transphyseal mechanical dowel that abruptly halts further shear displacement, allowing the physis to prematurely fuse in a stabilized position.
Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in proximal femoral pathology requires a nuanced synthesis of patient age, physiological reserve, fracture morphology, and underlying metabolic status. The following table delineates the strict indications and relative/absolute contraindications for the primary surgical interventions discussed in this chapter.
| Clinical Entity / Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Pauwels III Femoral Neck Fracture: Sliding Hip Screw (SHS) or Cephalomedullary Nail | - High-energy, vertically oriented fractures (>50 degrees) - Young, physiologically active patients - Polytrauma with ipsilateral femoral shaft fractures (Nail preferred) |
- Established avascular necrosis of the femoral head - Active joint infection - Severe osteoarthritis requiring arthroplasty |
- Severe comminution of the lateral femoral wall (requires specific implant modifications) - Significant delay to surgery (>3 weeks) with established nonunion |
| Pauwels I/II Femoral Neck Fracture: Parallel Cancellous Screws | - Low-angle, horizontally oriented fractures (<50 degrees) - Minimally displaced or valgus-impacted fractures - Physiologically robust elderly patients |
- Pauwels type III vertical fractures (high risk of shear failure) - Pathological fractures secondary to malignancy |
- Severe osteopenia (poor screw purchase) - Posterior comminution |
| SCFE: In Situ Pinning of Affected Hip | - Any confirmed slipped capital femoral epiphysis (stable or unstable) - Acute on chronic slips |
- Complete physeal closure (requires corrective osteotomy instead) - Active systemic infection |
- Severe, chronic slip with massive remodeling (may require Imhäuser osteotomy initially) |
| SCFE: Prophylactic Contralateral Pinning | - Underlying endocrinopathy (Hypothyroidism, Panhypopituitarism) - Renal osteodystrophy / Chronic Kidney Disease - Previous radiation therapy - High-risk morphological parameters (e.g., widened physis, modified Oxford bone age) |
- Closed contralateral physis - Normal metabolic panel in a low-risk, compliant patient who can be closely monitored |
- Extreme obesity complicating fluoroscopic visualization and hardware placement (requires careful risk/benefit analysis) |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Digital Templating
Meticulous pre-operative planning is the cornerstone of successful proximal femoral surgery. For high-energy femoral neck fractures, standard anteroposterior (AP) and cross-table lateral radiographs of the hip, along with a full-length AP of the femur and an AP pelvis, are mandatory. In the setting of high-energy trauma, a fine-cut computed tomography (CT) scan with 3D reconstructions is strongly recommended. The CT scan elucidates the degree of posterior comminution, the presence of occult basicervical extensions, and the true orientation of the fracture line, which often exhibits a spiral morphology not appreciated on plain films. Digital templating must be performed to determine the optimal angle of the sliding hip screw (typically 130 to 145 degrees), the anticipated length of the lag screw, and the necessity of a derotation screw to prevent spinning of the femoral head during hardware insertion.
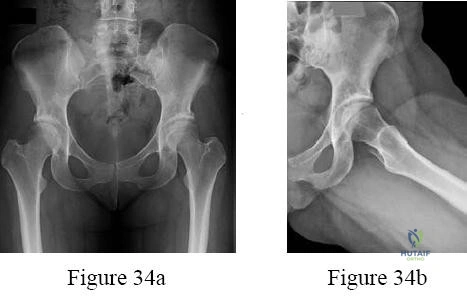
For the pediatric patient presenting with suspected SCFE, AP pelvis and frog-leg lateral radiographs are the gold standard. The AP radiograph is scrutinized for the disruption of Klein's line (a line drawn along the superior border of the femoral neck, which should normally intersect a portion of the lateral epiphysis). The frog-leg lateral view is critical for quantifying the slip angle (Southwick angle), which categorizes the severity of the deformity. In patients with metabolic disorders, such as chronic kidney disease, comprehensive laboratory panels including BUN, Creatinine, Calcium, Phosphate, Parathyroid Hormone (PTH), and Thyroid Stimulating Hormone (TSH) must be obtained prior to surgical clearance.
Patient Positioning and Fluoroscopic Setup
Patient positioning dictates the ease of reduction and the precision of hardware placement. For young adults with Pauwels III fractures, the patient is typically placed supine on a radiolucent fracture table. The contralateral limb is placed in a well-leg holder and abducted to allow unobstructed access for the C-arm fluoroscope in the lateral plane. Traction is applied to the operative limb, followed by internal rotation to correct the typical external rotation deformity and profile the femoral neck. However, the surgeon must be cautious; forceful or repeated closed reduction maneuvers can tear intact retinacular vessels, exacerbating the risk of AVN. If an anatomic closed reduction cannot be achieved seamlessly, the surgeon must be prepared to transition immediately to an open reduction.
For SCFE pinning, the patient is placed supine on a radiolucent Jackson or OSI flat table. A fracture table is generally avoided, as forceful traction or internal rotation is strictly contraindicated; attempting to "reduce" a chronic or stable SCFE dramatically increases the risk of AVN by stretching the already compromised posterior retinacular vessels. The C-arm is positioned to swing freely between the AP and true lateral planes. The operative limb is prepped and draped free to allow gentle manipulation during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Fixation of Pauwels Type III Fractures with a Fixed-Angle Device
The surgical management of a vertical shear fracture demands anatomical reduction and rigid fixed-angle stabilization. If closed reduction is inadequate, an open reduction via a Watson-Jones (anterolateral) or Smith-Petersen (anterior) approach is utilized. The Watson-Jones approach exploits the internervous plane between the tensor fasciae latae (superior gluteal nerve) and the gluteus medius (superior gluteal nerve). A capsulotomy in line with the femoral neck is performed, allowing direct visualization of the fracture. Hematoma is evacuated, and the fracture is anatomically reduced using point-to-point Weber clamps or a Jungbluth pelvic reduction forceps.
Once reduced, provisional fixation is achieved with terminally threaded Kirschner wires placed anteriorly or posteriorly to avoid interfering with the definitive hardware trajectory. For a sliding hip screw construct, a guide wire is advanced from the lateral cortex, aiming for the exact center-center position within the femoral head on both AP and lateral fluoroscopic views. Given the high shear forces, placing an anti-rotation cancellous screw superior to the planned SHS lag screw is highly recommended to prevent rotation of the proximal fragment during reaming and screw insertion. The lateral cortex is reamed, the lag screw is inserted to within 5 millimeters of the subchondral bone, and the side plate is applied to the femoral shaft. The construct is then compressed, effectively converting the deleterious shear forces into stabilizing compression across the fracture site.
Prophylactic and Therapeutic In Situ Pinning for SCFE
The objective of in situ pinning is to stabilize the epiphysis exactly where it lies, preventing further slip progression. A percutaneous or mini-open approach is utilized over the lateral proximal femur. Under fluoroscopic guidance, a guide wire is introduced at the level of the lesser trochanter. The trajectory is critical: the wire must pass through the center of the femoral neck and enter the center of the displaced epiphysis, perpendicular to the physis. Because the epiphysis is displaced posteriorly and inferiorly, the starting point on the lateral cortex is typically more anterior than in standard femoral neck pinning.
The surgeon must employ the "approach-withdrawal" fluoroscopic technique to ensure the wire and subsequent screw do not penetrate the articular surface. This involves rotating the hip through a full arc of motion under live fluoroscopy; if the hardware appears to breach the joint space at any point during rotation, it is intra-articular and must be repositioned. A single, fully threaded or partially threaded cannulated screw (typically 6.5 mm or 7.3 mm) is advanced over the guide wire. The threads must cross the physis and achieve robust purchase in the epiphyseal bone, with at least 4 to 5 threads engaging the epiphysis. In a patient with chronic kidney disease, bone quality may be compromised by renal osteodystrophy, necessitating meticulous tactile feedback during screw insertion to avoid stripping the cancellous bone. The identical procedure is then performed on the contralateral hip for prophylactic stabilization.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, interventions in the proximal femur carry significant complication profiles. The orthopedic surgeon must be vigilant in early detection and aggressive in salvage management.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Avascular Necrosis (AVN) - Trauma | 15% - 30% | Disruption of the MFCA retinacular vessels; poor initial reduction; delayed fixation. | Core decompression (early stages); Proximal femoral osteotomy; Total Hip Arthroplasty (THA) for end-stage collapse. |
| Nonunion / Fixation Failure | 10% - 20% | Failure to neutralize shear forces (e.g., using parallel screws for Pauwels III); varus collapse; poor bone quality. | Valgus intertrochanteric osteotomy to convert shear forces to compressive forces; Revision to fixed-angle device; THA. |
| Avascular Necrosis (AVN) - SCFE | 10% - 45% (Unstable) < 5% (Stable) |
Forceful reduction of the slip; intra-articular tamponade; posterosuperior hardware placement injuring vessels. | Restricted weight-bearing; hinged hip orthosis; ultimately may require THA in young adulthood if massive collapse occurs. |
| Chondrolysis | 5% - 7% | Unrecognized intra-articular hardware penetration; severe initial slip deformity. | Hardware removal; aggressive physical therapy; NSAIDs; arthrodiastasis; rarely arthrodesis. |
| Slip Progression | 2% - 5% | Inadequate thread purchase in the epiphysis; single screw failure in severe metabolic bone disease. | Revision fixation, potentially utilizing two screws if metabolic bone disease (e.g., severe CKD) precludes single-screw stability. |
| Femoroacetabular Impingement (FAI) | 30% - 50% | Prominent anterior metaphysis (cam deformity) impinging on the acetabular rim during flexion. | Arthroscopic or open osteochondroplasty of the femoral neck; surgical hip dislocation for complex remodeling. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation Following High-Energy Femoral Neck Fixation
The post-operative rehabilitation for a young adult following fixation of a Pauwels type III fracture must balance the need for early mobilization to prevent systemic complications with the mechanical necessity of protecting the fracture construct.
* Phase I (0-6 Weeks): The patient is generally restricted to toe-touch weight-bearing (TTWB) or flat-foot weight-bearing (maximum 20 lbs) on the operative extremity. Deep vein thrombosis (DVT) prophylaxis is mandatory, typically utilizing low molecular weight heparin or direct oral anticoagulants for a minimum of 28 to 35 days. Active and active-assisted range of motion (ROM) of the hip, knee, and ankle is initiated immediately to prevent capsular contracture.
* Phase II (6-12 Weeks): Clinical and radiographic evaluations are performed to assess for early callus formation and the absence of varus collapse. If stable, weight-bearing is progressively advanced by 25% of body weight per week. Closed-chain kinetic exercises and abductor strengthening are initiated.
* Phase III (3-6 Months): Progression to full, unrestricted weight-bearing. Advanced proprioceptive training and work-hardening programs are introduced. The patient is monitored for up to two years with serial radiographs to ensure complete union and to screen for late-onset avascular necrosis.
Rehabilitation Following SCFE Pinning
Rehabilitation following in situ pinning for SCFE is distinctly different, particularly when prophylactic bilateral pinning has been performed.
* Phase I (0-4 Weeks): For stable slips, patients are typically allowed touch-down to partial weight-bearing with bilateral axillary crutches. In the case of unstable slips, strict non-weight-bearing is enforced. Wheelchair use may be necessary for the patient who has undergone simultaneous bilateral pinning. Gentle, pain-free ROM is encouraged to nourish the articular cartilage and prevent stiffness.
* Phase II (4-8 Weeks): As acute post-operative pain subsides and early physeal stabilization occurs, patients are transitioned to full weight-bearing as tolerated. Physical therapy focuses on restoring full abductor strength and normalizing the gait pattern.
* Phase III (Long-Term Monitoring): Patients require longitudinal follow-up until complete physeal closure is documented bilaterally. In patients with underlying metabolic conditions, such as chronic kidney disease, close coordination with pediatric nephrology and endocrinology is vital to manage the underlying renal osteodystrophy, ensuring that the bone matrix is optimized to support the hardware until physeal fusion is complete.
Summary of Landmark Literature and Clinical Guidelines
The evolution of treatment for proximal femoral shear pathologies is deeply rooted in landmark orthopedic literature and evolving clinical guidelines.
Regarding femoral neck fractures, Friedrich Pauwels' original biomechanical classification remains the foundational text for understanding the conversion of physiological loads into shear stress. Modern biomechanical studies, such as those by Liporace et al., have definitively demonstrated that fixed-angle devices (SHS or cephalomedullary nails) provide vastly superior cycles-to-failure and load-to-failure metrics in vertical fracture patterns compared to parallel cancellous screws. Furthermore, the FAITH (Fixation using Alternative Implants for the Treatment of Hip fractures) trial, while primarily focused on an older demographic, underscored the high failure rates of cancellous screws in basicervical and vertical fracture patterns, reinforcing the absolute indication for sliding hip screws in high-shear environments.
In the realm of pediatric orthopedics, the Loder classification fundamentally shifted the paradigm of SCFE management by categorizing slips into "stable" (able to bear weight with or without crutches) and "unstable" (unable to bear weight). Loder's work highlighted the catastrophic rate of AVN (up to 47%) associated with unstable slips, driving the modern consensus against forceful closed reduction. Furthermore, guidelines established by the Pediatric Orthopaedic Society of North America (POSNA) strongly advocate for prophylactic contralateral pinning in patients presenting with SCFE who have an underlying endocrinopathy, previous radiation therapy, or renal osteodystrophy. The literature clearly demonstrates that in these metabolically compromised populations, the risk of a subsequent contralateral slip approaches certainty, justifying the minimal morbidity of prophylactic in situ pinning to prevent the devastating consequences of a missed unstable slip.
