Introduction and Biomechanics
Bimalleolar ankle fractures represent a significant disruption of both the medial and lateral stabilizing structures of the ankle joint. The tibiotalar joint is a highly congruent, weight-bearing hinge joint; even minor displacements can lead to catastrophic alterations in joint kinematics. Classic biomechanical studies have demonstrated that a mere 1 mm lateral shift of the talus reduces the tibiotalar contact area by 42%. This exponential decrease in contact area leads to a proportional increase in peak articular cartilage contact stresses, rapidly predisposing the patient to post-traumatic arthrosis.
While closed reduction can often be accomplished in the emergency department, it is notoriously difficult to maintain in a cast due to the inherent instability of the bimalleolar injury pattern. Therefore, Open Reduction and Internal Fixation (ORIF) is the gold standard of treatment, aiming to restore precise anatomic alignment, stabilize the mortise, and permit early range of motion.
Clinical Pearl: Anatomic restoration of the fibula (length, rotation, and alignment) is the cornerstone of ankle fracture management. The talus faithfully follows the lateral malleolus; if the fibula is malreduced, the talus will remain subluxated, leading to inevitable joint degeneration.
Initial Evaluation and Surgical Timing
The management of periarticular fractures—and ankle fractures in particular—is heavily dictated by the condition of the soft tissue envelope. Operative treatment is generally limited to two distinct time windows: early and late.
The "Early" Window (< 12 Hours)
ORIF may be safely performed within the first 12 hours following the injury, provided the surgical team can intervene before the onset of massive soft tissue edema. Immediate surgery has been associated with briefer hospitalizations and diminished postoperative pain.
The "Late" Window (2 to 3 Weeks)
If the early window is missed, surgery may not be possible for 2 to 3 weeks due to excessive swelling, fracture blisters, and compromised skin perfusion. Operating through severely edematous tissue exponentially increases the risk of wound dehiscence and deep infection.
Surgical Warning: If open reduction is delayed, immediate closed reduction of the fracture-dislocation and application of a well-padded plaster splint are absolutely mandatory. Failure to reduce a dislocated ankle will result in sustained pressure on the skin, leading to irreversible skin necrosis and potentially limb-threatening complications.
Equally good functional results have been found when comparing immediate versus delayed ORIF of Danis-Weber type B bimalleolar (or bimalleolar equivalent) ankle fractures. There are no statistically significant differences in long-term complications, adequacy of reduction, range of motion, or operative time between the two timelines. When surgery is delayed, the "wrinkle test" (the reappearance of skin lines when the ankle is dorsiflexed) is the most reliable clinical indicator that swelling has subsided sufficiently to proceed with ORIF. In cases of severe closed soft tissue injury, delayed closure or even skin grafting may ultimately be necessary.
Operative Techniques: Medial Malleolus
The medial malleolus is critical for the competence of the deltoid ligament complex and the medial stability of the mortise. The choice of fixation is dictated by the size, morphology, and comminution of the fracture fragment.
Fixation Strategies Based on Fracture Morphology
1. Large Fragments:
Large, solid medial malleolar fragments are typically fixed with a single or double lag screw technique. Two screws are preferred to control rotation, but a single robust lag screw may suffice if the fragment is appropriately captured.
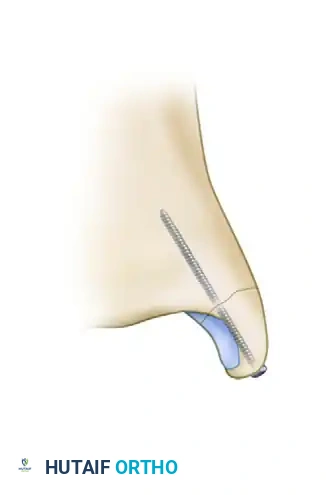
2. Small Fragments:
Smaller fragments may shatter if two screws are attempted. In these cases, the fragment can be fixed with one 4.0-mm partially threaded cancellous lag screw and one parallel Kirschner wire (K-wire) to prevent rotation.

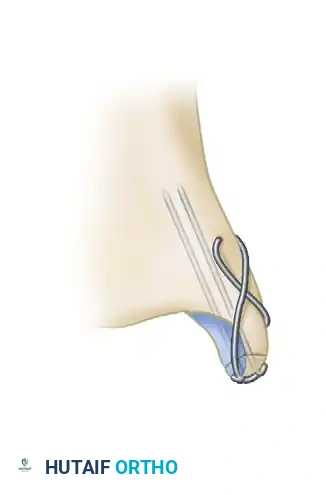
3. Comminuted or Very Small Fragments:
Fragments that are too small, osteopenic, or comminuted for standard screw fixation are best stabilized using a tension band wiring technique. This involves the placement of two parallel K-wires and a figure-of-eight stainless steel wire, which converts the tensile forces of the deltoid ligament into compressive forces across the fracture site.
4. Vertical Fractures:
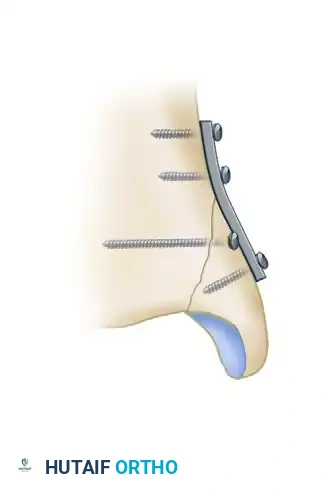
Vertical shear fractures of the medial malleolus (often seen in supination-adduction injuries) require a different biomechanical approach. Standard vertical screws will not provide adequate compression and may cause the fragment to slide. These require horizontally directed screws or antiglide plating techniques.
Biomechanical studies by Dumigan et al. have demonstrated that the fixation of vertical medial malleolar fractures with neutralization plating is biomechanically advantageous, providing superior resistance to shear forces compared to screw fixation alone.
Implant Selection: Stainless Steel vs. Bioabsorbable
While stainless steel and titanium implants remain the gold standard for medial malleolar fixation, the safety and efficacy of bioabsorbable implants have been extensively investigated.
The primary theoretical advantage of bioabsorbable screws (such as polyglycolide or polylactide) is the elimination of late hardware removal. Medial malleolar screws frequently cause persistent prominence or tenderness due to the thin subcutaneous tissue over the medial ankle.
While clinical outcomes (union rates, range of motion) show no significant differences between stainless steel and polyglycolide implants, bioabsorbables carry unique risks:
* Sterile Sinus Formation: Drainage from sterile sinuses has been reported in 5% to 10% of patients. This is directly related to the hydrolytic breakdown of polyglycolide, which can overwhelm the local tissue's clearing capacity.
* Inflammatory Reactions: In a large series of 2,528 patients, a 4.3% occurrence rate of clinically significant local inflammatory tissue reactions was reported.
Due to these localized reactions, the routine use of bioabsorbable implants requires careful patient selection and informed consent regarding the potential for sterile osteolysis and sinus tract formation.
Operative Techniques: Lateral Malleolus
Fractures of the lateral malleolus without significant medial injury are common, but in the context of a bimalleolar fracture, the lateral malleolus must be rigidly fixed to restore the lateral buttress of the ankle mortise.
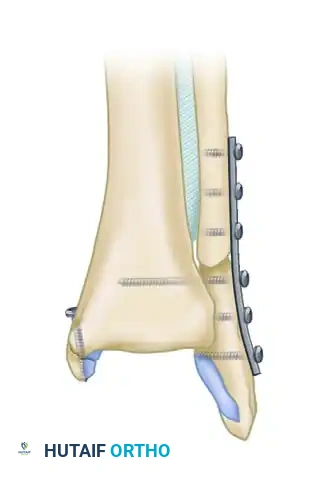
Standard Plate Fixation
The traditional approach utilizes a one-third tubular plate applied in a neutralization or antiglide fashion. Anatomic reduction of the fibula is confirmed visually and fluoroscopically, ensuring the restoration of the Shenton line of the ankle and the proper talocrural angle.
Lag Screw-Only Technique
In highly selected patients, plate fixation may be bypassed in favor of a lag screw-only technique. This is ideal for patients younger than 50 years with a simple oblique lateral malleolar fracture and minimal comminution. The fracture geometry must allow for the placement of at least two lag screws positioned a minimum of 1 cm apart.
Proponents of this technique report excellent outcomes with no nonunions, no loss of reduction, and a significant decrease in soft tissue complications. Furthermore, patients experience less hardware prominence and pain compared to those who undergo standard plate fixation.
Management of the Osteopenic Fibula
Fixation in elderly patients with osteopenic bone presents a significant challenge, as standard screws may lack adequate purchase, leading to construct failure.
Augmenting standard plate fixation with intramedullary Kirschner wires in osteopenic fibular fractures is highly recommended. Clinical studies show that 89% of patients treated with this augmented technique report minimal or no pain at final follow-up. Biomechanically, plates supplemented by intramedullary K-wires demonstrate an 81% greater resistance to bending forces than plates alone, and twice the resistance to motion during torsional testing.
Stress Fractures of the Medial Malleolus
While acute traumatic bimalleolar fractures are the primary focus of operative ankle trauma, stress fractures of the medial malleolus warrant special academic consideration due to their insidious onset and high complication rates.
Clinical Presentation and Diagnosis
Stress fractures of the medial malleolus typically present in athletes or military recruits as localized pain, swelling, and point tenderness directly over the medial ankle.
Initially, these fractures may not be apparent on standard orthogonal radiographs. If clinical suspicion is high, advanced imaging—such as a triple-phase bone scan, Computed Tomography (CT), or Magnetic Resonance Imaging (MRI)—is required to demonstrate the lesion. Often, the fracture only becomes radiographically apparent on follow-up X-rays weeks later as periosteal reaction and bone resorption occur.
Treatment Algorithm
The medial malleolus is subjected to significant tensile forces from the deltoid ligament during the gait cycle. Consequently, stress fractures in this region have a notoriously high risk of progression to complete fracture, delayed union, or frank nonunion. Aggressive treatment is frequently necessary.
Shelbourne et al. established a widely accepted treatment algorithm:
* Immediate Radiographic Visibility: If the stress fracture is immediately apparent on initial plain radiographs, internal fixation (ORIF) is strongly recommended to prevent displacement and ensure union.
* Visible Only on Advanced Imaging: If the fracture is only apparent on a bone scan or MRI (with negative plain films), a trial of strict cast immobilization and non-weight-bearing is appropriate.
Pitfall: Underestimating a medial malleolar stress fracture can lead to a catastrophic completion of the fracture during athletic activity. If treated operatively, patients must be counseled that a 4- to 5-month period of strictly restricted activity is necessary to achieve robust clinical and radiographic union.
Postoperative Protocol and Rehabilitation
The postoperative management of bimalleolar fractures is tailored to the stability of the fixation and the quality of the patient's bone.
- Phase I (0-2 Weeks): The ankle is immobilized in a bulky Jones dressing or a posterior splint. The patient is strictly non-weight-bearing. Elevation is critical to manage postoperative edema and protect the surgical incisions.
- Phase II (2-6 Weeks): Sutures are removed at 14 days. If fixation is rigid, the patient may be transitioned to a removable fracture boot to initiate early active range of motion (dorsiflexion and plantarflexion). Weight-bearing status remains restricted, though touch-down weight-bearing may be permitted depending on surgeon preference and radiographic appearance.
- Phase III (6-12 Weeks): Progressive weight-bearing is initiated once clinical and radiographic signs of early union are present. Physical therapy focuses on restoring proprioception, peroneal strength, and Achilles tendon flexibility.
Conclusion
The successful management of bimalleolar ankle fractures requires a profound understanding of ankle biomechanics, meticulous soft tissue management, and precise surgical execution. Whether utilizing traditional stainless steel plating, bioabsorbable implants, or augmented constructs for osteopenic bone, the ultimate goal remains the anatomic restoration of the tibiotalar joint to prevent early-onset osteoarthritis and restore full functional capacity to the patient.
📚 Medical References
- bimalleolar ankle fractures, Instr Course Lect 39:85, 1990.
- DeCoster TA, Willis MC, Marsh JL, et al: Rank order analysis of tibial plafond fractures: does injury or reduction predict outcome? Foot Ankle Int 20:44, 1999.
- Dickson KF, Montgomery S, Field J: High energy plafond fractures treated by a spanning external fi xator initially and followed by a second stage open reduction internal fi xation of the articular surface—preliminary report, Injury 32(suppl D):92, 2001.
- Donatto KC: Ankle fractures and syndesmosis injuries, Orthop Clin North Am 32:79, 2001.
- Ebraheim NA, Mekhail AO, Haman SP: External rotation-lateral view of the ankle in the assessment of the posterior malleolus, Foot Ankle Int 20:379, 1999.
- Egol KA, Weisz R, Hiebert R, et al: Does fi bular plating improve alignment after
