ATLANTOOCCIPITAL FUSION (OCCIPITALIZATION OF THE ATLAS)
Atlantooccipital fusion, commonly referred to as occipitalization of the atlas, represents a spectrum of congenital anomalies characterized by partial or complete fusion between the first cervical vertebra (atlas) and the base of the occiput. The morphological presentation is highly variable, ranging from complete osseous assimilation to a rudimentary bony bridge or a constricting fibrous band uniting a focal area of the atlas to the occiput.
This condition fundamentally alters the biomechanics of the craniocervical junction (CCJ), predisposing the patient to chronic atlantoaxial instability, basilar invagination, and profound neurological sequelae secondary to spinal cord impingement and vascular compromise of the vertebral arteries.
Embryology and Pathoanatomy
Embryologically, occipitalization results from a failure of segmentation between the fourth occipital sclerotome (which forms the proatlas) and the first spinal sclerotome. Normally, the proatlas divides to form the anterior margin of the foramen magnum, the occipital condyles, and the apical and alar ligaments, while the first spinal sclerotome forms the atlas. Failure of this intricate separation leads to the assimilation of the atlas into the cranial base.
The incidence of atlantooccipital fusion is estimated at 1.4 to 2.5 per 1,000 live births, affecting males and females equally. While the anomaly is present at birth, clinical symptoms typically manifest insidiously during the third and fourth decades of life. This delayed presentation is attributed to the progressive loss of ligamentous elasticity, age-related degenerative changes, and the cumulative biomechanical stress placed on the adjacent C1-C2 articulation.
Clinical Pearl: The C0-C1 articulation normally accounts for approximately 50% of the total flexion and extension of the cervical spine. When this motion segment is congenitally fused, the physiological load is entirely transferred to the C1-C2 joint. Over time, this hypermobility leads to attenuation of the transverse atlantal ligament, resulting in atlantoaxial instability in approximately 50% of affected patients.
Associated Congenital Anomalies
Atlantooccipital fusion is rarely an isolated entity. It is frequently associated with Klippel-Feil syndrome and other segmentation defects. A congenital fusion between C2 and C3 is observed in up to 70% of patients with occipitalization.
Systemic and structural anomalies occur in approximately 20% of patients and include:
* Spinal Deformities: Kyphosis and scoliosis.
* Craniofacial Anomalies: Jaw malformations, incomplete cleft of the nasal cartilage, cleft palate, and external ear deformities.
* Musculoskeletal Anomalies: Cervical ribs, syndactyly, and torticollis.
* Genitourinary Anomalies: Renal agenesis or structural urinary tract defects.
CLINICAL PRESENTATION
Patients with atlantooccipital fusion classically present with a triad of physical signs: a low posterior hairline, congenital torticollis, and a visibly shortened neck with restricted range of motion. Spillane et al. noted that virtually no patient with symptomatic atlantooccipital fusion possesses a normal-appearing neck.
The onset of symptoms may be spontaneous or precipitated by minor cervical trauma or upper respiratory tract infections (which can cause retropharyngeal hyperemia and secondary ligamentous laxity, akin to Grisel's syndrome).
Neurological and Vascular Syndromes
Symptoms are dictated by the specific anatomical region of neural or vascular impingement at the craniocervical junction:
- Pain: The most common initial complaint is a dull, aching suboccipital pain radiating to the posterior neck, often accompanied by episodic nuchal rigidity.
- Anterior Cord Compression: Impingement by a hypermobile or posteriorly angulated odontoid process leads to pyramidal tract irritation. Clinical signs include muscle weakness, atrophy, ataxia, spasticity, hyperreflexia, and the presence of pathological reflexes (Babinski and Hoffmann signs).
- Posterior Cord Compression: Compression from the assimilated posterior arch of the atlas or a thickened dural/fibrous band results in posterior column dysfunction. Patients exhibit a loss of proprioception, vibratory sensation, deep pain, and light touch.
- Cranial Nerve Involvement: Lower cranial nerve dysfunction can manifest as diplopia, dysphagia, dysarthria, and auditory disturbances. Nystagmus (often downbeat) is a frequent clinical finding.
- Vascular Compromise: Mechanical tethering or compression of the vertebral arteries within the anomalous osseous structures can produce vertebrobasilar insufficiency. Symptoms include syncope, drop attacks, seizures, vertigo, and an unsteady gait.
Surgical Warning: The vertebral artery frequently exhibits an anomalous course in patients with occipitalization. It may course inferior to the C1 arch, enter the dura prematurely, or be entirely encased in bone. Preoperative CT angiography (CTA) is mandatory to map the vertebral artery trajectory and prevent catastrophic intraoperative hemorrhage.
RADIOGRAPHIC EVALUATION
Standard plain radiographs of the craniocervical junction are notoriously difficult to interpret in patients with occipitalization due to overlapping osseous structures and the variable degree of assimilation.

Most commonly, the anterior arch of the atlas is assimilated into the occiput and displaced posteriorly. Approximately 50% of patients exhibit a relative basilar impression caused by the loss of height of the assimilated atlas. The posterior fusion often consists of a small bony fringe or a fibrous band directed caudally into the spinal canal, which may not be visible on plain films but is a primary driver of posterior neurological compression.
Dynamic Imaging and Morphometrics
Flexion and extension lateral cervical spine radiographs are a critical component of the initial evaluation to assess for atlantoaxial instability.
McRae and Barnum established critical morphometric thresholds for predicting neurological deficits. They measured the distance from the posterior aspect of the odontoid to the posterior arch of the atlas (or the posterior lip of the foramen magnum, whichever was closer).
* A distance of ≤ 19 mm was highly correlated with neurological deficits.
* More contemporary literature defines a Space Available for the Cord (SAC) or sagittal canal diameter of ≤ 13 mm as the critical threshold for neurological symptoms. This measurement must be taken on a flexion view, as maximal canal narrowing occurs during cervical flexion.
Basilar Invagination and Clark Stations
The shape and position of the odontoid process are the primary determinants of neurological morbidity. When the odontoid projects above the foramen magnum (violating McRae's line), basilar impression is present. Autopsy studies have demonstrated that an excessively long, posteriorly angulated odontoid directly indents the ventral brainstem.
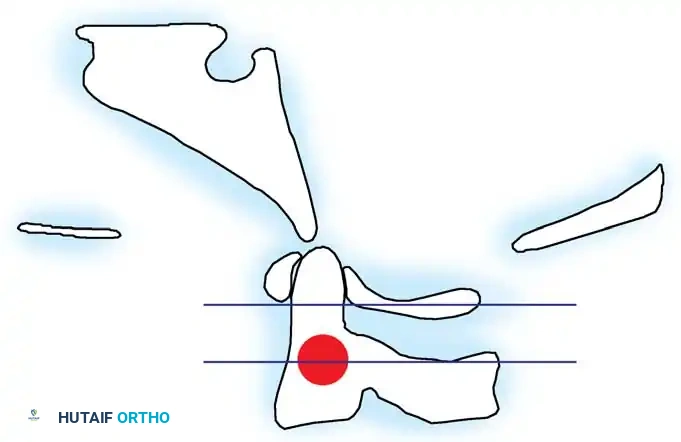
To systematically evaluate the degree of basilar invagination, the Clark Stations are utilized. The odontoid process is divided into three equal parts in the sagittal plane:
* Station I: The anterior ring of the atlas aligns with the cranial third of the odontoid (Normal).
* Station II: The anterior ring of the atlas aligns with the middle third of the odontoid (Indicates basilar impression).
* Station III: The anterior ring of the atlas aligns with the caudal third of the odontoid (Indicates severe basilar impression).
Advanced Neuroimaging
- Computed Tomography (CT): High-resolution CT with 3D reconstructions is the gold standard for defining the complex osseous anatomy, assessing the feasibility of C2 pedicle or pars screws, and evaluating the extent of bony assimilation.
- Magnetic Resonance Imaging (MRI): MRI is indispensable for evaluating the spinal cord and medulla. It identifies areas of myelomalacia (T2 hyperintensity), evaluates the cervicomedullary angle, and detects constricting posterior fibrous bands or dural thickening that plain films and CT miss.
SURGICAL MANAGEMENT
The primary goals of surgical intervention are the decompression of neural elements and the restoration of craniocervical stability.
Indications for Treatment
- Nonoperative Management: Patients with incidental findings, minor axial neck pain, or transient symptoms following minor trauma can be managed conservatively. Treatment includes rigid cervical orthoses (e.g., Miami J collar), careful observation, and avoidance of contact sports.
- Operative Management: Surgery is strictly indicated for patients with progressive neurological deficits, intractable pain, documented atlantoaxial instability, or significant basilar invagination causing brainstem compression.
Preoperative Planning and Reduction
The surgical strategy depends heavily on whether the craniocervical deformity is reducible or irreducible.
Preoperative cervical traction (using Gardner-Wells tongs or a halo ring) is often employed to attempt reduction of a hypermobile, invaginated odontoid.
* If traction successfully reduces the odontoid and relieves anterior compression, a posterior occipitocervical fusion (OCF) is sufficient.
* If the deformity is irreducible and anterior brainstem compression persists, an anterior decompression (transoral or endoscopic endonasal odontoidectomy) followed by a posterior OCF is required.
Surgical Technique: Posterior Occipitocervical Decompression and Fusion
1. Positioning and Neuromonitoring
The patient is placed prone, typically using a Mayfield skull clamp to maintain rigid cranial fixation. The neck is positioned in a neutral or slightly extended posture to optimize the sagittal alignment. Hyperflexion must be strictly avoided to prevent iatrogenic spinal cord injury. Continuous intraoperative neuromonitoring, including Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), is mandatory.
2. Surgical Exposure
A standard midline posterior approach is utilized, extending from the external occipital protuberance (inion) down to the subaxial cervical spine (typically C3 or C4, depending on the planned construct). Subperiosteal dissection exposes the occiput, the assimilated C1 arch, and the posterior elements of C2 and C3.
Pitfall: Dissection lateral to the facet joints or over the superior aspect of the C1 arch must be performed with extreme caution due to the high risk of encountering an anomalous vertebral artery or a massive epidural venous plexus.
3. Decompression (Suboccipital Craniectomy)
If posterior signs and symptoms are present due to bony or dural compression, a suboccipital craniectomy is performed.
* A high-speed burr and Kerrison rongeurs are used to resect the posterior rim of the foramen magnum and the assimilated posterior arch of the atlas.
* Crucially, any thickened dural bands or constricting fibrous tissues identified on preoperative MRI must be meticulously excised to ensure complete decompression of the cervicomedullary junction. If the dura is inadvertently opened, a watertight primary repair or duraplasty is required.
4. Instrumentation
Rigid internal fixation has largely replaced wiring techniques, offering superior biomechanical stability and higher fusion rates.
* Occipital Fixation: An occipital plate is secured to the skull. Screws should be placed in the thickest bone, which is located at the external occipital protuberance and along the superior nuchal line. A midline keel of bone provides optimal purchase.
* C2 Fixation: Depending on the patient's anatomy (assessed via preoperative CT), C2 pedicle screws or C2 pars screws are placed. C2 pedicle screws offer the highest pull-out strength. The entry point is typically in the cranial and lateral quadrant of the C2 lateral mass, with a trajectory directed 20-30 degrees medially and 20-30 degrees cranially.
* Subaxial Fixation: If C2-C3 congenital fusion is present (as in 70% of cases), the construct must often be extended to C3 or C4 using lateral mass screws to ensure adequate distal fixation.
5. Bone Grafting
Decortication of the occiput and the exposed cervical lamina/facet joints is performed using a high-speed burr. Autologous bone graft (typically harvested from the posterior iliac crest) or high-quality allograft mixed with osteoinductive agents is packed meticulously along the decorticated surfaces to promote a robust arthrodesis.
Postoperative Protocol and Complications
Postoperatively, patients are typically maintained in a rigid cervical collar for 6 to 12 weeks, depending on the bone quality and the rigidity of the intraoperative construct. Halo vest immobilization is rarely required with modern screw-rod constructs but may be reserved for cases of poor bone quality or revision surgery.
Potential Complications:
1. Vertebral Artery Injury: The most devastating intraoperative complication. Immediate management involves tamponade, packing, and potentially endovascular embolization. Bilateral injury is frequently fatal.
2. Cerebrospinal Fluid (CSF) Leak: Due to the resection of adherent dural bands or inadvertent durotomy during craniectomy. Requires meticulous repair and potentially a lumbar drain.
3. Pseudarthrosis: Nonunion at the occipitocervical junction can lead to hardware failure and recurrent instability. Meticulous decortication and the use of autograft minimize this risk.
4. Dysphagia/Dyspnea: Can occur if the occipitocervical junction is fused in excessive extension, narrowing the oropharyngeal airway. Intraoperative fluoroscopy must confirm a neutral craniocervical angle (O-C2 angle) prior to final rod tightening.
📚 Medical References
- Hensinger RN: Atlantooccipital fusion. In Cervical Spine Research Society: The cervical spine, Philadelphia, 1983, Lippincott. Kalla AK, Khanna S, Singh IP, et al: A genetic and anthropological study of atlanto-occipital fusion, Hum Genet 81:105, 1989.
- McRae DL: Bony abnormalities in the region of the foramen magnum: correlation of the anatomic and neurologic fi ndings, Acta Radiol 40:335, 1953.
- McRae DL: The signifi cance of abnormalities of the cervical spine, AJR Am J Roentgenol 84:3, 1960.
- McRae DL, Barnum AS: Occipitalization of the atlas, AJR Am J Roentgenol 70:23, 1953.
- Sakou T, Kawaida H, Morizono Y, et al: Occipitoatlantoaxial fusion utilizing a rectangular rod, Clin Orthop Relat Res 239:137, 1989.
- Spillane JD, Pallis C, Jones AM: Developmental abnormalities in the region of the foramen magnum, Brain 80:11, 1957.
- Watson AG, Mayhew IG: Familial congenital occipitoatlantoaxial malformation (OAAM) in the Arabian horse, Spine 11:334, 1986.
- Klippel-Feil Syndrome Al-Rajeh S, Chowdhary UM, Al-Freihi H, et al: Thoracic disc protrusion and situs inversus in Klippel-Feil syndrome, Spine 15:1379, 1987.
- Baird PA, Robinson CG, Buckler WSJ: Klippel-Feil syndrome, Am J Dis Child 113:546, 1967.
- Beals RK, Rolfe B: VATER association: a unifying concept of multiple anomalies, J Bone Joint Surg 71A:948, 1989.
- Bhagat R, Pant K, Singh VK, et al: Pulmonary developmental anomaly associated with Klippel-Feil syndrome and anomalous atrioventricular conduction, Chest 101:1157, 1992.
- Bonola A: Surgical treatment of the Klippel-Feil syndrome, J Bone Joint Surg 38B:440, 1956.
- Born CT, Petrik M, Freed M, et al: Cerebrovascular accident complicating Klippel-Feil syndrome: a case report, J Bone Joint Surg 70A:1412, 1988.
- Clarke RA, Catalan G, Diwan AD, et al: Heterogeneity in Klippel-Feil syndrome: a new classifi cation, Pediatr Radiol 28:967, 1998.
- Clarke RA, Davis PJ, Tonkin J: Klippel-Feil syndrome associated with malformed larynx: case report, Ann Otol Rhinol Laryngol 103:201, 1994.
- Clarke RA, Kearsley JH, Walsh DA: Patterned expression in familial Klippel-Feil syndrome, Teratology 53:152, 1996.
- Clarke RA, Singh S, McKenzie H, et al: Familial Klippel-Feil syndrome and paracentric inversion inv(8)(q22.2q23.3), Am J Hum Genet 57:1364, 1995.
- Drvaric DM, Ruderman RJ, Conrad RW, et al:
