ATLANTOAXIAL ROTATORY SUBLUXATION
Atlantoaxial rotatory subluxation (AARS) represents a spectrum of rotational abnormalities at the C1-C2 articulation. It is a well-recognized and common cause of childhood torticollis. In the vast majority of pediatric cases, the subluxation and resultant torticollis are transient. However, in rare instances, the deformity persists, transitioning into a rigid state best described as atlantoaxial rotatory "fixation."
AARS occurs when the normal, highly mobile articulation between the atlas (C1) and the axis (C2) becomes mechanically limited or rigidly fixed. The etiology is multifactorial; it can occur spontaneously, secondary to minor or major cervical trauma, or following an upper respiratory tract infection (URI) or head and neck surgery. When associated with a URI or retropharyngeal inflammation, the condition is classically termed Grisel’s syndrome.
Clinical Pearl: Watson-Jones originally postulated that hyperemic decalcification of the anterior atlas ring and laxity of the transverse ligament, driven by the rich anastomotic pharyngovertebral venous plexus draining the nasopharynx into the periodontoid venous plexus, is the primary pathophysiological driver of Grisel's syndrome.
Pathoanatomy and Biomechanics
To fully grasp the implications of AARS, a thorough understanding of C1-C2 kinematics is mandatory. The atlantoaxial joint is responsible for approximately 50% of total cervical spine rotation. This hypermobility is permitted by the biconvex nature of the C1-C2 facet joints and the absence of interlocking bony constraints.
Stability is entirely dependent on the ligamentous complex:
* Transverse Ligament: The primary restraint preventing anterior translation of C1 on C2.
* Alar Ligaments: Secondary restraints connecting the odontoid process to the medial aspect of the occipital condyles. They limit axial rotation and lateral bending.
* Facet Capsules: Provide secondary rotational stability.
In AARS, unilateral or bilateral facet capsular distension, combined with alar ligament laxity or rupture, alters the instantaneous axis of rotation. The C1 lateral mass subluxates anteriorly or posteriorly over the C2 superior articular facet, eventually locking into a fixed position due to muscle spasm or capsular contracture.
Fielding and Hawkins Classification
The widely accepted classification system for rotatory displacement was established by Fielding and Hawkins. It is based on the direction of displacement and the integrity of the transverse ligament, which directly correlates with the risk of neurological compromise.
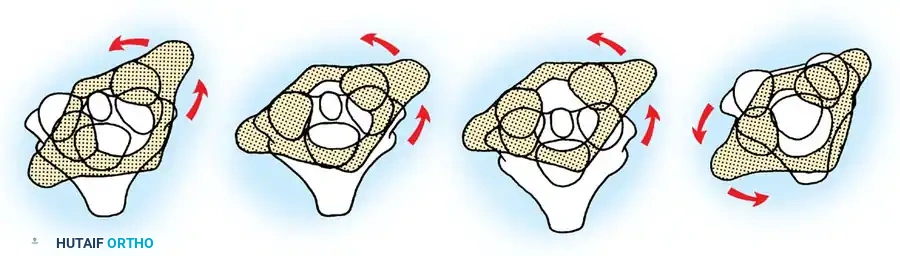
- Type I: Simple rotatory displacement without anterior shift (atlanto-dens interval [ADI] ≤ 3 mm). The odontoid acts as the intact pivot point. This is the most common type and occurs primarily in children. It implies that the transverse ligament is intact.
- Type II: Rotatory displacement with an anterior displacement of 3 to 5 mm. One lateral articular process acts as the pivot point, while the contralateral mass displaces anteriorly. This indicates a deficiency or stretching of the transverse ligament.
- Type III: Rotatory displacement with an anterior displacement of more than 5 mm. Both lateral masses are displaced anteriorly. This indicates complete incompetence of the transverse ligament and secondary restraints (alar ligaments), carrying a high potential for neurological damage.
- Type IV: Rotatory displacement with a posterior shift of the atlas on the axis. This is exceedingly rare, typically requiring a deficient odontoid (e.g., os odontoideum or severe hypoplasia) and carries a severe risk of spinal cord compression.
Surgical Warning: Types II, III, and IV represent progressive ligamentous incompetence. While Type I is often managed conservatively, Types II-IV require rigorous neurological monitoring and have a significantly lower threshold for surgical stabilization due to the compromised space available for the cord (SAC).
Clinical Presentation
AARS typically presents in the pediatric population following a URI, minor trauma, or spontaneously. The hallmark clinical sign is the "cock robin" position:
* The head is tilted to one side.
* The head is rotated to the opposite side.
* The neck is held in slight flexion.
The sternocleidomastoid (SCM) muscle on the long side (the side contralateral to the chin direction) is frequently in severe spasm. This spasm is a compensatory attempt by the body to correct the deformity, distinguishing it from congenital muscular torticollis, where the spasm/contracture is on the short side.
In the acute phase, any attempt to passively or actively move the head elicits severe pain. Patients may be able to voluntarily increase the deformity but are mechanically unable to correct the rotation past the midline. Over weeks to months, the acute muscle spasms may subside, rendering the torticollis less painful, but the rigid deformity persists. A meticulous neurological examination is paramount to rule out spinal cord compression or vertebral artery compromise, particularly in Type II-IV displacements.
Radiographic Findings and Diagnosis
Obtaining adequate cervical spine radiographs in a child with painful torticollis is notoriously difficult but essential.
Plain Radiography
Initial evaluation must include anteroposterior (AP), lateral, and open-mouth odontoid views.
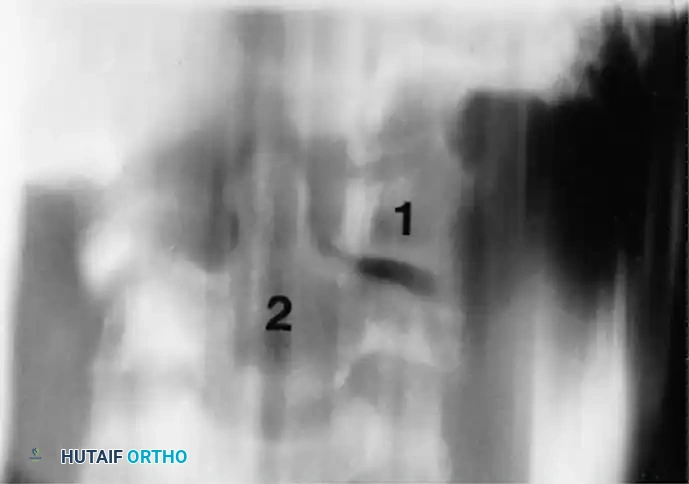
* Open-Mouth Odontoid View: The lateral mass of C1 that is rotated forward (anteriorly) appears wider and closer to the midline (odontoid). Conversely, the opposite lateral mass appears narrower and further away from the midline. Apparent overlapping may obscure one of the C1-C2 facet joints.
* Lateral View: The anteriorly rotated lateral mass appears wedge-shaped and is superimposed in front of the odontoid process. Due to the head tilt, the posterior arch of the atlas may falsely appear assimilated into the occiput.
Lateral flexion and extension views should be obtained (if tolerated) to document any anterior-posterior atlantoaxial instability (assessing the ADI). If standard radiographs are inconclusive due to positioning difficulties, a lateral radiograph of the skull can sometimes delineate the relative C1-C2 position more clearly.
Advanced Imaging
- Dynamic Computed Tomography (DCTS): CT is the gold standard for confirming AARS. Scans are performed with the head rotated maximally to the left and right. This confirms the loss of normal rotation at the atlantoaxial joint.
- McGuire et al. Classification of DCTS:
- Stage 0: Torticollis is present clinically, but DCTS is normal (normal C1-C2 excursion).
- Stage 1: Limitation of motion (< 15 degrees difference between C1 and C2), but C1 is still able to cross the midline of C2.
- Stage 2: Fixed deformity. C1 does not cross the midline of C2 regardless of active or passive effort.
- Note: While McGuire found a correlation between DCTS stage and treatment intensity, authors like Alanay et al. and Hicazi et al. have debated the absolute necessity of DCTS, suggesting that static 3D CT reconstructions often provide sufficient diagnostic clarity without subjecting a child in pain to dynamic maneuvers.
- McGuire et al. Classification of DCTS:
- Magnetic Resonance Imaging (MRI): Indicated if there are any neurological deficits, to evaluate the integrity of the transverse ligament, or to assess for retropharyngeal abscess/phlegmon in cases of Grisel's syndrome.
Nonoperative Management
The treatment algorithm for AARS is heavily dictated by the duration of symptoms and the presence of instability. Phillips and Hensinger established a highly effective, time-dependent treatment protocol.
Phillips and Hensinger Protocol
- Duration < 1 Week:
- Immobilization in a soft cervical collar.
- Aggressive analgesics and muscle relaxants.
- Strict bed rest for 1 week.
- If spontaneous reduction does not occur: Proceed to hospitalization and traction.
- Duration > 1 Week but < 1 Month:
- Hospital admission.
- Cervical traction (typically head-halter traction starting at 3-5 lbs).
- Muscle relaxants (e.g., diazepam) to break the SCM spasm.
- Once clinical and radiographic reduction is achieved, transition to a rigid cervical collar for 4 to 6 weeks.
- Duration > 1 Month:
- Hospital admission.
- Skeletal traction (cranial tongs or halo traction) is usually required, as soft tissue contractures are more rigid.
- Gradual increase in weight with serial radiographic monitoring.
- Following reduction, immobilization in a rigid collar or halo-vest for 4 to 6 weeks.
Pitfall: Nonoperative treatment is strictly contraindicated if radiographic evaluation reveals significant anterior displacement (Fielding Types II, III, IV) with an ADI > 5mm, or if there is any evidence of neurological compromise.
Operative Management
When conservative measures fail, or when the pathoanatomy dictates immediate stabilization, surgical arthrodesis of C1-C2 is required.
Indications for Surgery (Fielding's Criteria)
- Neurological involvement: Any sign of myelopathy or radiculopathy.
- Anterior displacement: Fielding Types II, III, and IV (ADI > 3-5 mm indicating transverse ligament rupture).
- Failure to achieve and maintain correction: If the deformity has existed for longer than 3 months, soft tissue contractures generally preclude stable conservative reduction.
- Recurrence: Relapse of the deformity after an adequate trial of conservative management (at least 6 weeks of rigid immobilization).
Preoperative Planning
Fielding and Hawkins strongly recommend a period of preoperative skeletal traction for 2 to 3 weeks. The goal is to stretch contracted soft tissues, reduce the facet dislocation, and correct the deformity as much as possible prior to positioning on the operating table. Attempting forceful intraoperative reduction of a chronic AARS carries a catastrophic risk of vertebral artery injury or spinal cord contusion.
Surgical Technique: Posterior C1-C2 Arthrodesis
The gold standard surgical intervention is a posterior C1-C2 fusion. While historical techniques relied on sublaminar wiring (Gallie or Brooks-Jenkins techniques), modern constructs utilize rigid screw-rod fixation (Goel-Harms technique), which provides superior biomechanical stability and higher fusion rates without the need for postoperative halo immobilization.
1. Positioning and Neuromonitoring
- The patient is placed prone on a Jackson table or similar radiolucent frame.
- The head is secured in Mayfield tongs or a halo ring. The neck is maintained in a neutral position. Do not force reduction during positioning.
- Somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) are monitored continuously.
2. Surgical Approach
- A standard posterior midline incision is made from the inion to C3.
- Avascular dissection is carried down the ligamentum nuchae.
- Subperiosteal dissection exposes the posterior arch of C1 and the lamina/spinous process of C2.
- Caution: Dissection on the superior aspect of the C1 ring must not extend more than 1.5 cm lateral to the midline to avoid injuring the vertebral artery as it courses through the vertebral groove (sulcus arteriae vertebralis).
3. Instrumentation (Goel-Harms Technique)
- C1 Lateral Mass Screws:
- The C2 nerve root is identified and gently retracted caudally (or transected if necessary for exposure and to prevent postoperative occipital neuralgia, though this is debated).
- The venous plexus surrounding the C2 nerve root is meticulously coagulated using bipolar electrocautery and hemostatic agents (e.g., Gelfoam, thrombin).
- The entry point for the C1 lateral mass screw is at the intersection of the posterior arch and the midpoint of the C1 lateral mass.
- The trajectory is 10-15 degrees medial (aiming for the anterior tubercle of C1) and 15 degrees cephalad.
- C2 Pedicle or Pars Screws:
- Pars Screws: Entry point is 3 mm superior and 3 mm lateral to the medial border of the C2-C3 facet joint. Trajectory is parallel to the C2 pars interarticularis (steeply cephalad and slightly medial).
- Pedicle Screws: Entry point is slightly more cranial and lateral. Trajectory is 20-25 degrees medial and 20 degrees cephalad. Preoperative CT navigation or fluoroscopy is critical to ensure the vertebral artery is not violated in the foramen transversarium.
4. Reduction and Rod Placement
- If the joint is still subluxated, the C1-C2 facet joints are decorticated and mobilized.
- Custom-contoured rods are seated into the tulip heads of the C1 and C2 screws.
- Reduction can be achieved by manipulating the rods or using reduction instruments to pull C1 posteriorly and align the lateral masses.
5. Bone Grafting
- Rigid instrumentation must be supplemented with robust biological fusion.
- The posterior arch of C1 and the lamina/spinous process of C2 are decorticated using a high-speed burr.
- Autologous bone graft (typically harvested from the posterior superior iliac spine) is packed over the decorticated surfaces. Structural tricortical grafts can be wedged between the C1 arch and C2 spinous process and secured with a titanium cable (modified Gallie construct) to supplement the screw-rod construct.
Postoperative Protocol
If modern rigid screw-rod instrumentation is utilized, a rigid cervical collar (e.g., Aspen or Miami J) for 6 to 12 weeks is usually sufficient.
If historical wiring techniques are used, or if bone quality is exceptionally poor, Fielding and Hawkins recommended 6 weeks of postoperative traction or the application of a halo-vest to maintain correction until radiographic evidence of solid bony arthrodesis is observed.
Special Considerations: Down Syndrome
Patients with Trisomy 21 (Down syndrome) present a unique challenge regarding atlantoaxial pathology. As noted by Spitzer, Rabinowitch, and Wybar, atlantoaxial instability occurs in approximately 10% to 20% of children with Down syndrome, while atlantooccipital instability can reach an incidence of 60%.
Clinical Pearl: It is critical to distinguish between cervical hypermobility and true cervical instability in the Down syndrome population.
- Hypermobility: Refers to increased ligamentous excursion compared to normal controls, but without the loss of structural integrity of the anatomical restraints. The neural elements remain protected.
- Instability: Implies pathological intersegmental motion that jeopardizes neurological integrity (e.g., an ADI > 5 mm in children, or a Space Available for the Cord [SAC] < 14 mm).
The cervical spine instability in children with Down syndrome is frequently associated with congenital anomalies of the upper cervical spine, including odontoid hypoplasia and os odontoideum. While routine screening radiographs for asymptomatic Down syndrome patients remain a topic of debate among pediatric orthopedic societies, any patient presenting with torticollis, gait changes, or upper motor neuron signs requires immediate advanced imaging and likely surgical stabilization to prevent catastrophic spinal cord injury.
📚 Medical References
- Alanay A, Hicazi A, Acaroglu E, et al: Reliability and necessity of dynamic computerized tomography in diagnosis of atlantoaxial rotatory subluxation, J Pediatr Orthop 22:763, 2002.
- Burkus JK, Deponte RJ: Chronic atlantoaxial rotatory fi xation correction by cervical traction, manipulation, and bracing: case report, J Pediatr Orthop 6:631, 1986.
- Coutts MB: Atlantooccipital subluxations, Arch Surg 29:297, 1934.
- Fielding JW: The cervical spine in the child, Curr Pract Orthop Surg 5:31, 1973.
- Fielding JW, Francis WR, Hawkins RJ, et al: Atlantoaxial rotary deformity, Semin Spine Surg 3:33, 1991.
- Fielding JW, Hawkins RJ: Atlantoaxial rotatory fi xation (fi xed rotatory subluxation of the atlantoaxial joint), J Bone Joint Surg 59A:37, 1977.
- Fielding JW, Hawkins RJ, Ratzan S: Fusion for atlantoaxial instability, J Bone Joint Surg 58A:400, 1976.
- Firrani-Gallotta G, Luzzatti G: Sublussazione laterale e sublussazione rotatorie dell’atlante, Arch Orthop Trauma Surg 70:467, 1957.
- Georgopoulos G, Pizzutillo PD, Lee MS: Occipitoatlantal instability in children: a report of fi ve cases and review of the literature, J Bone Joint Surg 69A:429, 1987.
- Hensinger RN, DeVito PD, Ragsdale CG: Changes in the cervical spine in juvenile rheumatoid arthritis, J Bone Joint Surg 68A:189, 1986.
- Hicazi A, Acaroglu E, Alanay A, et al: Atlantoaxial rotatory fi xation-subluxation revisited: a computed tomography analysis of acute torticollis in pediatric patients, Spine 27:2771, 2002.
- Kawabe N, Hirotani H, Tanaka O: Pathomechanism of atlantoaxial rotatory fi xation in children, J Pediatr Orthop 9:569, 1989.
- McGuire KJ, Silber J, Flynn JM, et al: Torticollis in children: can dynamic computed tomography help determine severity and treatment? J Pediatr Orthop 22:766, 2002.
- Phillips WA, Hensinger RN: The management of rotatory atlantoaxial subluxation in children, J Bone Joint Surg 71A:664, 1989.
- Subach BR, McLaughlin MR, Albright AL, et al: Current management of pediatric atlantoaxial rotatory subluxation, Spine 23:2174, 1998.
- Wackenheim A: Roentgen diagnosis of the craniovertebral region, New York, 1974, Springer-Verlag. Wang J, Vokshoor A, Kim S, et al: Pediatric atlantoaxial instability: management with screw fi xation, Pediatr Neurosurg 30:70, 1999.
- Watson-Jones R: Spontaneous hyperaemic dislocation of the atlas, Proc R Soc Med 25:586, 1931.
- Cervical Instability in Down Syndrome Burke SW, French CHG, Roberts JM, et al: Chronic atlantoaxial instability in Down syndrome, J Bone Joint Surg 67A:1356, 1985.
- Committee on Sports Medicine: Atlantoaxial instability in Down syndrome, Pediatrics 74:152, 1984.
- Dormans JP, Drummond DS, Sutton LN, et al: Occipitocervical arthrodesis in children, J Bone Joint Surg 77A:1234, 1995.
- Gabriel KR, Mason DE, Carango P: Occipitoatlantal translation in Down’s syndrome, Spine 15:997, 1990.
- Loder RT, Hensinger RN: Developmental abnormalities of the cervical spine. In Weinstein SL, ed: The pediatric spine, vol 1, New York, 1994, Raven. Menezes AH, Ryken TC: Craniovertebral abnormalities in Down’s syndrome, Pediatr Neurosurg 18:24, 1992.
- Menezes AH, Ryken TC: Craniovertebral junction abnormalities. In Weinstein SL, ed: The pediatric spine, vol 1, New York, 1994, Raven. Msall M, Rogers B, DiGaudio K, et al: Long-term complications of segmental cervical fusion in Down syndrome, Dev Med Child Neurol 33:5, 1991.
- Nordt JC, Stauffer ES: Sequelae of atlantoaxial stabilization of two patients with Down’s syndrome, Spine 6:437, 1981.
- Parfenchuck TA, Bertrand SL, Powers MJ, et al: Posterior occipitoatlantal hypermobility in Down syndrome: an analysis of 199 patients, J Pediatr Orthop 14:304, 1994.
- Pizzutillo PD, Herman MJ: Cervical spine issues in Down syndrome, J Pediatr Orthop 25:253, 2005.
- Pueschel SM: Should children with Down syndrome be screened for atlantoaxial instability? Arch Pediatr Adolesc Med 152:123, 1998.
- Pueschel SM, Findley TW, Furia J, et al: Atlantoaxial instability in Down syndrome: radiographic, neurologic, and somatosensory-evoked potential studies, J Pediatr 110:515, 1987.
- Pueschel SM, Herndon JH, Gelch MM, et al: Symptomatic atlantoaxial subluxation in persons with Down syndrome, J Pediatr Orthop 4:682, 1984.
- Pueschel SM, Scola FH, Perry CD, et al: Atlantoaxial instability in children with Down syndrome, Pediatr Radiol 10:129, 1981.
- Pueschel SM, Scola FH, Pezzullo JC: A longitudinal study of atlantodens relationships in asymptomatic individuals with Down syndrome, Pediatrics 89:1194, 1992.
- Pueschel SM, Scola FH, Tupper TB, et al: Skeletal anomalies of the upper cervical spine in children with Down syndrome, J Pediatr Orthop 10:607, 1990.
- Segal LS, Drummond DS, Zanotti RM, et al: Complications of posterior arthrodesis of the cervical spine in patients who have Down syndrome, J Bone Joint Surg 73A:1547, 1991.
- Smith MD, Phillips WA, Hensinger RN: Complications of fusion to the upper cervical spine, Spine 16:702, 1991.
- Smith MD, Phillips WA, Hensinger RN: Fusion of the upper cervical spine in children and adolescents: an analysis of 17 patients, Spine 16:695, 1991.
- Spitzer R, Rabinowitch JY, Wybar KC: A study of the abnormalities of the skull, teeth, and lenses in mongolism, Can Med Assoc J 84:567, 1961.
- Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome, J Pediatr Orthop 10:602, 1990.
- Van Dyke DC, Gahagan CA: Down syndrome, cervical spine abnormalities, and problems, Clin Pediatr 27:415, 1988.
- Wiesel SW, Rothman RH: Occipitoatlantal hypermobility, Spine 4:187, 1979.
- Familial Cervical Dysplasia Saltzman CL, Hensinger RN, Blane CE, et al: Familial cervical dysplasia, J Bone Joint Surg 73A:163, 1991.
- Congenital Anomalies of Atlas Dubousset J: Torticollis in children caused by congenital anomalies of the atlas, J Bone Joint Surg 68A:178, 1986.
- Winter RB, Lonstein JE, Leonard AS: Congenital deformities of the spine , New York, 1983, Thieme-Stratton. Intervertebral Disc Calcifi cation Dai LY, Ye H, Qian QR: The natural history of cervical disc calcifi cation in children, J Bone Joint Surg 86A:1467, 2004.
- Ginalski JM, Landry M, Gudinchet F, et al: Is tomography of intervertebral disc calcifi cation useful in children? Pediatr Radiol 22:59, 1992.
- Hahn YS, McLone DG, Uden D: Cervical intervertebral disc calcifi cation in children, Childs Nerv Syst 3:274, 1987.
- Herring JA, Hensinger RN: Cervical disc calcifi cation, J Pediatr Orthop 8:613, 1988.
- Oda J, Tanaka H, Tsuzuki N: Intervertebral disc changes with aging of human cervical vertebra from the neonate to the eighties, Spine 13:1205, 1988.
- Pattisapu JV, Evans OB, Blumenthal BI: Intervertebral disc calcifi cation in children, Pediatr Neurol 3:108, 1987.
- Sonnabend DH, Taylor TKF, Chapman GK: Intervertebral disc calcifi cation syndromes in children, J Bone Joint Surg 64B:25, 1982.
- Wong CC, Pereira B, Pho RW: Cervical disc calcifi cation in children: a long-term review, Spine 17:139, 1992.
