Full Question & Answer Text (for Search Engines)
Question 1:
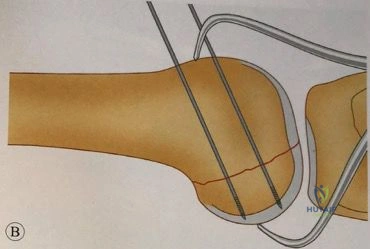
A 6-year-old boy falls on an outstretched hand and sustains an ulnar diaphyseal fracture associated with a radial neck fracture. According to the Bado classification equivalents, what type of Monteggia lesion does this represent?
Options:
- Type I equivalent
- Type II equivalent
- Type III equivalent
- Type IV equivalent
- Type V equivalent
Correct Answer: Type I equivalent
Explanation:
A Bado Type I equivalent involves an anterior dislocation of the radial head or a fracture of the radial neck combined with an ulnar diaphyseal fracture. Type I Bado injuries are the most common Monteggia lesions in children, traditionally characterized by anterior apex ulnar bowing or fracture combined with an anterior radial head dislocation.
Question 2:
A 65-year-old man who underwent total hip arthroplasty 5 years ago presents with groin pain and a palpable anterior thigh mass. Plain radiographs show a well-fixed cementless implant without osteolysis. Joint aspiration yields cloudy, sterile fluid. Serum cobalt levels are markedly elevated, while chromium is normal. What is the most likely underlying pathophysiological mechanism?
Options:
- Galvanic corrosion at the stem-sleeve junction
- Mechanically assisted crevice corrosion at the head-neck junction
- Aseptic loosening secondary to polyethylene wear debris
- Delayed-onset periprosthetic joint infection
- Adverse local tissue reaction from a metal-on-metal bearing
Correct Answer: Mechanically assisted crevice corrosion at the head-neck junction
Explanation:
The presentation is classic for trunnionosis, which refers to mechanically assisted crevice corrosion at the modular head-neck junction (the trunnion). It typically presents with elevated serum cobalt (often discordant with chromium) and an adverse local tissue reaction (ALTR) resulting in a pseudotumor, even in patients with metal-on-polyethylene bearings.
Question 3:
Bone morphogenetic protein-2 (BMP-2) is heavily utilized in spine surgery for its potent osteoinductive properties. Through which of the following intracellular signaling pathways does BMP-2 primarily exert its osteogenic effect?
Options:
- Activation of the Wnt/beta-catenin pathway
- Phosphorylation of SMAD 1, 5, and 8
- Inhibition of RANKL expression
- Activation of the JAK/STAT signaling cascade
- Stimulation of fibroblast growth factor receptor 3 (FGFR3)
Correct Answer: Phosphorylation of SMAD 1, 5, and 8
Explanation:
BMP-2 binds to a heterodimeric serine/threonine kinase receptor on the cell surface. This binding leads to the intracellular phosphorylation of receptor-regulated SMADs (SMAD 1, 5, and 8). These form a complex with the common-mediator SMAD 4, which then translocates to the nucleus to regulate the transcription of osteogenic genes such as Runx2.
Question 4:
In the evaluation of a patient with suspected pyogenic flexor tenosynovitis, which of Kanavel's four classic signs is generally considered the earliest and most sensitive indicator of the condition?
Options:
- Fusiform swelling of the entire digit
- Flexed resting posture of the digit
- Tenderness localized to the flexor tendon sheath
- Severe pain with passive extension of the digit
- Erythema extending to the palmar crease
Correct Answer: Severe pain with passive extension of the digit
Explanation:
Kanavel's four signs of pyogenic flexor tenosynovitis are: 1) fusiform swelling (sausage digit), 2) flexed resting posture, 3) tenderness along the flexor tendon sheath, and 4) excruciating pain with passive extension. Pain with passive extension is widely recognized as the earliest and most sensitive clinical sign of a flexor sheath infection.
Question 5:
A 25-year-old soccer player sustains a twisting injury to his knee. On physical examination, the dial test reveals 15 degrees of increased external rotation on the injured side compared to the contralateral normal knee at 30 degrees of knee flexion. However, at 90 degrees of knee flexion, the external rotation is equal bilaterally. Which anatomic structure(s) is/are injured?
Options:
- Isolated posterior cruciate ligament (PCL)
- Isolated posterolateral corner (PLC)
- Combined PCL and PLC
- Combined ACL and PLC
- Isolated medial patellofemoral ligament (MPFL)
Correct Answer: Isolated posterolateral corner (PLC)
Explanation:
The dial test is used to differentiate isolated posterolateral corner (PLC) injuries from combined PLC and PCL injuries. An increase in external rotation of >10 degrees at 30 degrees of flexion, but not at 90 degrees, indicates an isolated PLC injury. If the asymmetry is present at both 30 and 90 degrees, it suggests a combined PCL and PLC injury.
Question 6:
A 35-year-old male presents with chronic shoulder pain and a lytic lesion in the proximal humeral epiphysis. Radiographs show a well-defined geographic lytic lesion with central punctate calcifications. Histological examination reveals sheets of cells with abundant clear cytoplasm, distinct cell membranes, and areas of malignant hyaline cartilage intermixed with woven bone. What is the most likely diagnosis?
Options:
- Chondroblastoma
- Giant Cell Tumor
- Clear cell chondrosarcoma
- Ewing sarcoma
- Osteoblastoma
Correct Answer: Clear cell chondrosarcoma
Explanation:
Clear cell chondrosarcoma is a rare, low-grade variant of chondrosarcoma that characteristically occurs in the epiphysis of long bones (typically proximal femur or humerus) in adults (third to fifth decade). It often mimics chondroblastoma radiographically (which also occurs in the epiphysis but usually in younger patients prior to physeal closure), but histologically features cells with clear cytoplasm and malignant hyaline cartilage.
Question 7:
During the surgical approach to the posteromedial aspect of the tibial plateau for internal fixation of a Schatzker IV fracture, the primary internervous/intermuscular plane is utilized. Which structures define the borders of this interval?
Options:
- Semimembranosus and the medial head of the gastrocnemius
- Pes anserinus and the medial head of the gastrocnemius
- Tibialis posterior and flexor digitorum longus
- Medial head of the gastrocnemius and the soleus
- Semitendinosus and semimembranosus
Correct Answer: Pes anserinus and the medial head of the gastrocnemius
Explanation:
The posteromedial approach to the tibial plateau utilizes an interval between the medial head of the gastrocnemius (innervated by the tibial nerve) posteriorly, and the pes anserinus (innervated by the femoral and sciatic nerves) anteriorly. Retracting the gastrocnemius posteriorly and laterally protects the popliteal neurovascular bundle.
Question 8:
According to the modified Hawkins classification, a Hawkins Type III fracture of the talar neck involves subluxation or dislocation of which of the following joints?
Options:
- Subtalar joint only
- Subtalar and tibiotalar joints
- Subtalar, tibiotalar, and talonavicular joints
- Tibiotalar joint only
- Talonavicular and calcaneocuboid joints
Correct Answer: Subtalar and tibiotalar joints
Explanation:
The Hawkins classification for talar neck fractures is: Type I: Nondisplaced. Type II: Displaced with subluxation/dislocation of the subtalar joint. Type III: Displaced with subluxation/dislocation of both the subtalar and tibiotalar joints. Type IV: Displaced with subluxation/dislocation of the subtalar, tibiotalar, and talonavicular joints.
Question 9:
In articular cartilage, which zone has the highest concentration of proteoglycans, the lowest water content, and collagen fibers oriented strictly perpendicular to the articular surface?
Options:
- Superficial (tangential) zone
- Middle (transitional) zone
- Deep (radial) zone
- Calcified cartilage zone
- Tidemark
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone of articular cartilage represents about 30% of the cartilage volume. It provides the greatest resistance to compressive forces, possesses the highest proteoglycan concentration, the lowest water content, and features large diameter Type II collagen fibrils arranged perpendicular to the joint surface to anchor the cartilage to the underlying bone.
Question 10:
A 6-week-old female infant is being treated with a Pavlik harness for developmental dysplasia of the hip (DDH). She has been strictly in the harness for 4 weeks, but a repeat ultrasound demonstrates that the hip remains persistently dislocated. What is the most appropriate next step in management?
Options:
- Continue the Pavlik harness for an additional 3 weeks
- Discontinue the Pavlik harness and transition to a rigid abduction orthosis or schedule closed reduction
- Perform an immediate open reduction and spica casting
- Switch to double-diapering
- Perform a varus derotational osteotomy (VDRO)
Correct Answer: Discontinue the Pavlik harness and transition to a rigid abduction orthosis or schedule closed reduction
Explanation:
Prolonged use of a Pavlik harness in a persistently dislocated hip leads to 'Pavlik harness disease', characterized by erosion of the posterior acetabular wall, which makes future reduction significantly more difficult. If a hip remains dislocated after 3 to 4 weeks of strict Pavlik harness wear, the harness must be discontinued. The accepted next step is transitioning to a rigid abduction brace (e.g., Ilfeld) or proceeding to closed reduction and spica casting.
Question 11:
A 45-year-old cyclist presents with isolated weakness of finger abduction and adduction, and an inability to cross his fingers. Sensation over the volar aspect of his small finger and the ulnar half of the ring finger is completely intact. Where is the most likely site of ulnar nerve compression?
Options:
- Cubital tunnel
- Guyon's canal - Zone 1
- Guyon's canal - Zone 2
- Guyon's canal - Zone 3
- Arcade of Struthers
Correct Answer: Guyon's canal - Zone 2
Explanation:
Guyon's canal is divided into three zones. Zone 1 is proximal to the nerve bifurcation and contains both motor and sensory fibers; compression here causes mixed deficits. Zone 2 surrounds the deep motor branch; compression here causes isolated motor deficits of the ulnar-innervated intrinsic hand muscles. Zone 3 contains the superficial sensory branch; compression here causes isolated sensory deficits. 'Cyclist's palsy' frequently presents as an isolated motor deficit due to Zone 2 compression.
Question 12:
A 68-year-old female presents with catching and a painful 'pop' at the anterior aspect of her knee when extending her leg from a flexed position. She underwent a posterior-stabilized (PS) total knee arthroplasty 18 months ago. Which implant design factor is most strongly associated with the development of this specific complication?
Options:
- A decreased patellar component thickness
- A lowered joint line
- A high intercondylar box ratio
- Internal rotation of the tibial component
- A thick tibial polyethylene insert
Correct Answer: A high intercondylar box ratio
Explanation:
The patient is presenting with 'patellar clunk syndrome', characterized by the formation of a fibrous nodule at the superior pole of the patella that catches in the intercondylar notch of the femoral component during active extension. It is classically associated with early posterior-stabilized (PS) knee designs that featured a high, anteriorly placed intercondylar box ratio, leading to impingement of the quadriceps tendon.
Question 13:
A 40-year-old male sustains an isolated thoracolumbar fracture at T12 following a fall. Neurological examination is completely normal. CT imaging demonstrates a burst fracture of T12 with 30% loss of anterior vertebral body height and splaying of the pedicles. MRI reveals the posterior ligamentous complex (PLC) is intact. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is his total score and the generally recommended treatment pathway?
Options:
- Score 2; nonoperative management
- Score 3; surgical management
- Score 4; surgeon's choice
- Score 5; surgical management
- Score 7; surgical management
Correct Answer: Score 2; nonoperative management
Explanation:
The TLICS scoring system considers three parameters: injury morphology, neurological status, and integrity of the posterior ligamentous complex (PLC). Morphology: burst fracture = 2 points. Neurological status: intact = 0 points. PLC: intact = 0 points. Total score = 2. A score of less than 4 implies nonoperative management is indicated.
Question 14:
A 28-year-old male presents with a slow-growing, painful mass in his left tibial diaphysis. Radiographs show a distinct, multi-loculated, expansile osteolytic 'soap-bubble' lesion within the anterior cortex of the tibia. Biopsy demonstrates a biphasic tumor with nests of basaloid epithelial cells dispersed within a fibrous stroma. What is the most appropriate definitive management for this lesion?
Options:
- Curettage and bone grafting
- Preoperative chemotherapy followed by wide resection
- Wide surgical resection
- Radiation therapy
- Radiofrequency ablation
Correct Answer: Wide surgical resection
Explanation:
The clinical, radiographic, and histologic presentation is classic for adamantinoma. Adamantinoma is a rare, low-grade malignant bone tumor that almost exclusively occurs in the anterior diaphyseal cortex of the tibia. It is biphasic, displaying both epithelial and osteofibrous components. It is notoriously resistant to both chemotherapy and radiation. The standard of care is wide surgical resection.
Question 15:
During an anterior intrapelvic (modified Stoppa) approach to the acetabulum, severe hemorrhage is encountered just superior to the superior pubic ramus. This bleeding is most likely originating from the corona mortis, which is an anastomotic connection between which two vascular systems?
Options:
- Internal iliac artery and internal pudendal artery
- External iliac (or inferior epigastric) vessels and the obturator vessels
- Femoral artery and external iliac artery
- Superior gluteal artery and inferior gluteal artery
- Deep circumflex iliac artery and the external iliac vein
Correct Answer: External iliac (or inferior epigastric) vessels and the obturator vessels
Explanation:
The corona mortis ('crown of death') is an anatomical variant representing a vascular anastomosis between the external iliac (or its inferior epigastric branch) and the obturator vessels (a branch of the internal iliac). It crosses the superior pubic ramus at an average distance of 5-6 cm from the pubic symphysis and is at high risk of iatrogenic injury during anterior pelvic exposures.
Question 16:
In the context of preparing polymethylmethacrylate (PMMA) bone cement, which of the following modifications significantly decreases the mechanical strength and fatigue life of the cement mantle?
Options:
- Adding antibiotics in powder form rather than liquid form
- Vacuum mixing the cement
- Centrifuging the cement prior to application
- Adding liquid antibiotics or excessive fluid
- Pre-chilling the monomer
Correct Answer: Adding liquid antibiotics or excessive fluid
Explanation:
Adding aqueous/liquid substances (like liquid antibiotics) or excessive fluid significantly increases porosity and radically decreases the ultimate mechanical strength and fatigue life of PMMA bone cement. Antibiotics should only be added in fine powder form. Vacuum mixing and centrifugation both decrease porosity and thereby increase fatigue life. Pre-chilling the monomer prolongs the working time but does not weaken the cement.
Question 17:
A 13-year-old obese male presents to the emergency department complaining of right hip and thigh pain after slipping on ice. He is completely unable to bear weight on the right leg, even with crutches. Radiographs demonstrate a displaced Slipped Capital Femoral Epiphysis (SCFE) of the right hip. Based on the Loder classification, what is his primary risk regarding the natural history of this specific injury pattern?
Options:
- Chondrolysis
- Avascular necrosis (AVN) of the femoral head
- Coxa magna
- Femoroacetabular impingement (FAI)
- Premature physeal closure
Correct Answer: Avascular necrosis (AVN) of the femoral head
Explanation:
According to the Loder classification, SCFE is divided into stable and unstable. 'Unstable' is defined clinically as the inability to ambulate, even with assistive devices (crutches). The incidence of avascular necrosis (AVN) in unstable SCFE is extremely high (up to 47%), whereas it is nearly 0% in stable SCFE.
Question 18:
The Lisfranc ligament is a critical stabilizing structure of the midfoot. What are the precise anatomic attachments of the primary Lisfranc ligament?
Options:
- From the lateral aspect of the medial cuneiform to the medial base of the second metatarsal
- From the intermediate cuneiform to the base of the second metatarsal
- From the lateral cuneiform to the cuboid
- From the navicular to the medial cuneiform
- From the medial cuneiform to the base of the first metatarsal
Correct Answer: From the lateral aspect of the medial cuneiform to the medial base of the second metatarsal
Explanation:
The Lisfranc ligament is an oblique, stout plantar interosseous ligament that spans from the lateral aspect of the medial cuneiform to the medial aspect of the base of the second metatarsal. There is no direct ligamentous connection between the bases of the first and second metatarsals, making this region uniquely vulnerable to disruption.
Question 19:
A 55-year-old male sustains a traumatic anterior shoulder dislocation. After a successful closed reduction, he complains of profound weakness in shoulder abduction and external rotation. Electromyography (EMG) at 6 weeks confirms an isolated peripheral nerve injury. Which of the following nerve roots primarily contribute to the affected nerve?
Options:
- C5, C6
- C6, C7
- C7, C8
- C8, T1
- C5, C6, C7
Correct Answer: C5, C6
Explanation:
Anterior shoulder dislocations are frequently associated with axillary nerve palsy. The axillary nerve innervates the deltoid (shoulder abduction) and teres minor (external rotation). The axillary nerve arises from the posterior cord of the brachial plexus and carries nerve fibers primarily from the C5 and C6 nerve roots.
Question 20:
In the setting of massive posterosuperior rotator cuff tears, which muscle uniquely demonstrates a high degree of rapid fat accumulation and atrophy due to suprascapular nerve retraction and compression via the 'sling effect' at the spinoglenoid notch?
Options:
- Subscapularis
- Infraspinatus
- Supraspinatus
- Teres minor
- Teres major
Correct Answer: Infraspinatus
Explanation:
While both the supraspinatus and infraspinatus are innervated by the suprascapular nerve, massive posterosuperior rotator cuff tears lead to severe medial retraction. The suprascapular nerve takes a sharp turn at the spinoglenoid notch to reach the infraspinatus. Medial retraction of the cuff causes traction on the nerve at this unyielding notch (the 'sling effect'), disproportionately causing profound denervation and rapid fatty infiltration in the infraspinatus compared to the supraspinatus.
Question 21:
What is the most frequently injured nerve in an extension-type supracondylar fracture of the humerus in a pediatric patient?
Options:
- Ulnar nerve
- Anterior interosseous nerve
- Posterior interosseous nerve
- Axillary nerve
- Musculocutaneous nerve
Correct Answer: Anterior interosseous nerve
Explanation:
The anterior interosseous nerve (AIN), a branch of the median nerve, is the most frequently injured nerve in extension-type supracondylar fractures of the humerus. This is typically due to traction over the proximal fragment. AIN palsy presents with the inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger (loss of the 'OK' sign).
Question 22:
Which of the following is the most significant adverse prognostic factor for overall survival in a patient with conventional high-grade osteosarcoma?
Options:
- High alkaline phosphatase at presentation
- Male gender
- Presence of skip metastases
- Tumor size greater than 8 cm
- Proximal tibial location
Correct Answer: Presence of skip metastases
Explanation:
While high serum alkaline phosphatase and large tumor size are poor prognostic factors, the presence of macroscopic metastases (including skip lesions within the same bone or distant pulmonary metastases) is the most significant adverse prognostic indicator for overall survival in osteosarcoma.
Question 23:
During an anterior cruciate ligament (ACL) reconstruction, the surgeon inadvertently places the femoral tunnel too anteriorly in the intercondylar notch. Which of the following kinematic abnormalities will most likely result?
Options:
- The graft is tight in flexion and loose in extension
- The graft is tight in extension and loose in flexion
- The graft is tight throughout the entire range of motion
- The graft is loose throughout the entire range of motion
- The graft impinges in the intercondylar notch in extension
Correct Answer: The graft is tight in flexion and loose in extension
Explanation:
Placing the femoral tunnel too anteriorly in the intercondylar notch causes the ACL graft to be tight in knee flexion and loose in extension. This error restricts full knee flexion and may cause early graft failure or stretching.
Question 24:
A 65-year-old female with adult degenerative scoliosis presents with intractable neurogenic claudication and low back pain. Corrective surgery is planned. Which of the following is the primary indication for extending a spinal fusion down to the pelvis rather than stopping at L5?
Options:
- Cobb angle greater than 30 degrees
- L5-S1 fractional curve greater than 15 degrees
- Previous microdiscectomy at L4-L5
- Flexible coronal curve on lateral bending films
- Normal sagittal balance
Correct Answer: L5-S1 fractional curve greater than 15 degrees
Explanation:
Extending a long spinal fusion to the pelvis in adult spinal deformity is indicated when there is significant L5-S1 pathology, such as a fractional curve > 15 degrees, advanced L5-S1 disc degeneration, spondylolisthesis at L5-S1, or previous laminectomy at L5-S1. Stopping at L5 in the presence of these conditions often leads to rapid adjacent segment failure and pseudoarthrosis.
Question 25:
The Pauwels classification for femoral neck fractures categorizes fractures based on which of the following parameters?
Options:
- The degree of comminution of the posterior neck
- The anatomical location of the fracture line (subcapital vs transcervical)
- The angle of the fracture line relative to the horizontal plane
- The amount of displacement on the anteroposterior radiograph
- The severity of associated varus collapse
Correct Answer: The angle of the fracture line relative to the horizontal plane
Explanation:
The Pauwels classification is based on the angle of the fracture line relative to the horizontal plane. Type I is <30 degrees, Type II is 30-50 degrees, and Type III is >50 degrees. Higher angles indicate increased shear forces across the fracture site, which correlates with higher rates of nonunion and fixation failure.
Question 26:
During an open carpal tunnel release, the transverse carpal ligament is systematically divided. Which of the following bony structures form the ulnar attachment of the transverse carpal ligament?
Options:
- Scaphoid tuberosity and trapezium ridge
- Hook of the hamate and pisiform
- Triquetrum and lunate
- Trapezoid and capitate
- Styloid process of the ulna
Correct Answer: Hook of the hamate and pisiform
Explanation:
The transverse carpal ligament (flexor retinaculum) forms the roof of the carpal tunnel. It attaches radially to the scaphoid tuberosity and the crest of the trapezium, and ulnarly to the pisiform and the hook of the hamate.
Question 27:
Primary bone healing (contact healing via osteonal reconstruction) is achieved under which of the following mechanical and biological conditions?
Options:
- Absolute stability with a gap less than 0.01 mm
- Relative stability with a gap of 2 mm
- Cast immobilization allowing micro-motion
- Intramedullary nailing of a diaphyseal fracture
- External fixation with dynamic axial loading
Correct Answer: Absolute stability with a gap less than 0.01 mm
Explanation:
Primary bone healing requires absolute mechanical stability and precise anatomical reduction with a fracture gap of less than 0.01 mm. It occurs via direct Haversian remodeling (cutting cones advancing across the fracture site) without intermediate callus formation.
Question 28:
According to modern Level I evidence regarding the management of acute Achilles tendon ruptures, which of the following statements is true when an accelerated functional rehabilitation protocol is employed?
Options:
- Operative treatment has a significantly lower re-rupture rate than non-operative treatment
- Non-operative treatment carries a higher risk of deep venous thrombosis compared to surgery
- There is no clinically important difference in re-rupture rates between operative and non-operative treatment
- Operative treatment provides significantly greater plantar flexion strength at 1 year
- Non-operative treatment requires a minimum of 12 weeks of strict cast immobilization
Correct Answer: There is no clinically important difference in re-rupture rates between operative and non-operative treatment
Explanation:
Recent high-quality Level I studies (such as the Willits trial) demonstrate that when an accelerated functional rehabilitation protocol (early weight-bearing and early mobilization) is used, there is no clinically important difference in re-rupture rates between operative and non-operative management. Operative treatment is, however, associated with higher risks of wound complications and nerve injury.
Question 29:
In total hip arthroplasty, the use of highly cross-linked polyethylene (HXLPE) compared to conventional ultra-high molecular weight polyethylene (UHMWPE) results in which of the following material property changes?
Options:
- Increased ultimate tensile strength
- Increased resistance to abrasive wear
- Increased fatigue crack propagation resistance
- Increased oxidation resistance post-gamma irradiation in air
- Increased risk of osteolysis at 10 years
Correct Answer: Increased resistance to abrasive wear
Explanation:
Highly cross-linked polyethylene (HXLPE) is manufactured to significantly increase resistance to adhesive and abrasive wear, thereby reducing wear debris and subsequent osteolysis. However, the cross-linking process and subsequent thermal treatments decrease mechanical properties such as ultimate tensile strength, yield strength, and fatigue crack propagation resistance.
Question 30:
What is the most devastating and rapid complication specifically associated with the surgical pinning of an unstable Slipped Capital Femoral Epiphysis (SCFE)?
Options:
- Chondrolysis
- Osteonecrosis (Avascular Necrosis) of the femoral head
- Femoroacetabular impingement
- Progressive leg length discrepancy
- Premature osteoarthritis
Correct Answer: Osteonecrosis (Avascular Necrosis) of the femoral head
Explanation:
Osteonecrosis (AVN) is the most devastating complication of SCFE, occurring at a significantly higher rate in unstable SCFE (reported up to 47%) compared to stable SCFE (almost 0%). It is typically caused by disruption of the retinacular vessels, which can be exacerbated by forceful closed reduction or hematoma accumulation.
Question 31:
In the Young-Burgess classification of pelvic ring injuries, an anteroposterior compression (APC) Type II injury is characterized by the rupture of which ligaments?
Options:
- Anterior sacroiliac, sacrotuberous, and sacrospinous ligaments with an intact posterior sacroiliac ligament
- Anterior and posterior sacroiliac ligaments
- Sacrotuberous ligament only
- Posterior sacroiliac ligament only
- Iliolumbar ligament only
Correct Answer: Anterior sacroiliac, sacrotuberous, and sacrospinous ligaments with an intact posterior sacroiliac ligament
Explanation:
An APC II injury involves symphyseal diastasis (usually >2.5 cm) with disruption of the anterior sacroiliac, sacrotuberous, and sacrospinous ligaments. The critical posterior sacroiliac ligament remains intact, making the pelvis rotationally unstable ('open book') but vertically stable.
Question 32:
Denosumab is highly effective in the treatment of unresectable or metastatic Giant Cell Tumor of bone (GCTB). What is the specific molecular target of this medication?
Options:
- Vascular Endothelial Growth Factor (VEGF)
- Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL)
- Tumor Necrosis Factor alpha (TNF-alpha)
- Osteoprotegerin (OPG)
- Sclerostin
Correct Answer: Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL)
Explanation:
Denosumab is a fully human monoclonal antibody that binds to and inhibits RANK Ligand (RANKL). In GCTB, the neoplastic mononuclear stromal cells express high levels of RANKL, which recruits and activates the reactive multinucleated giant cells (osteoclast-like cells) that cause extensive bone osteolysis.
Question 33:
During the physical examination of a patient with suspected cervical radiculopathy, the examiner applies downward axial compression to the patient's head while the neck is extended and laterally flexed to the symptomatic side. This provocative maneuver is known as:
Options:
- Hoffman's sign
- Lhermitte's sign
- Spurling's test
- Babinski reflex
- Adson's test
Correct Answer: Spurling's test
Explanation:
Spurling's test (foraminal compression test) is performed by extending and laterally bending the neck to the symptomatic side while applying axial compression. A positive test is the reproduction of radicular arm pain, indicating cervical nerve root compression within the neural foramen.
Question 34:
Six months after open reduction and internal fixation of a distal radius fracture with a volar locking plate, the patient develops a sudden inability to actively extend the interphalangeal joint of the thumb. Which tendon is most likely injured, and what is the primary mechanism?
Options:
- Extensor pollicis longus (EPL); attritional rupture due to prominent dorsal screws
- Extensor pollicis brevis (EPB); impingement from the volar plate
- Flexor pollicis longus (FPL); attritional rupture over the watershed line
- Extensor carpi radialis longus (ECRL); iatrogenic transection during surgery
- Extensor pollicis longus (EPL); spontaneous rupture secondary to a previously non-displaced Lister's tubercle fracture
Correct Answer: Extensor pollicis longus (EPL); attritional rupture due to prominent dorsal screws
Explanation:
The inability to actively extend the thumb interphalangeal joint indicates a rupture of the Extensor pollicis longus (EPL) tendon. In the setting of a previously placed volar plate, this complication is classically caused by excessively long screws protruding through the dorsal cortex, leading to attritional wear and eventual rupture of the EPL tendon.
Question 35:
A 22-year-old athlete sustains a longitudinal tear in the peripheral one-third of the medial meniscus. This specific zone has the highest healing potential following a meniscal repair primarily because:
Options:
- It receives nourishment exclusively from synovial fluid diffusion
- It is directly supplied by the middle genicular artery
- It has a rich blood supply from the perimeniscal capillary plexus
- It contains type II collagen organized in a radial pattern
- It is completely devoid of neurovascular structures
Correct Answer: It has a rich blood supply from the perimeniscal capillary plexus
Explanation:
The peripheral one-third of the meniscus (the 'red-red' zone) is highly vascularized by the perimeniscal capillary plexus, which arises from branches of the medial and lateral inferior genicular arteries. This rich blood supply affords this region excellent healing potential. The central zones are avascular and rely on diffusion.
Question 36:
In standard mechanically aligned Total Knee Arthroplasty (TKA), the distal femoral cut is typically made at what angle relative to the anatomical axis of the femur to restore a neutral mechanical axis?
Options:
- 0 degrees
- 3 degrees of valgus
- 5 to 7 degrees of valgus
- 9 to 11 degrees of valgus
- 3 degrees of varus
Correct Answer: 5 to 7 degrees of valgus
Explanation:
The mechanical axis of the femur runs from the center of the femoral head to the center of the knee joint. The anatomical axis runs down the intramedullary canal of the femoral shaft. The angle between them represents the valgus cut angle, which averages 5 to 7 degrees of valgus for most patients to achieve a neutral overall mechanical alignment.
Question 37:
During the descent phase of a squat exercise, the quadriceps muscle actively lengthens while remaining under tension to control knee flexion. What type of muscle contraction does this describe?
Options:
- Concentric
- Isometric
- Eccentric
- Isokinetic
- Plyometric
Correct Answer: Eccentric
Explanation:
An eccentric contraction occurs when the muscle lengthens while actively producing force (e.g., the quadriceps during the descent phase of a squat acting as a brake). Concentric contractions occur when the muscle shortens, and isometric contractions occur when there is no change in muscle length.
Question 38:
When treating an infant for Developmental Dysplasia of the Hip (DDH) using a Pavlik harness, hyperflexion of the hips beyond 120 degrees places the child at significant risk for which specific complication?
Options:
- Femoral nerve palsy
- Sciatic nerve palsy
- Obturator nerve palsy
- Avascular necrosis of the femoral head
- Inferior dislocation of the hip
Correct Answer: Femoral nerve palsy
Explanation:
Excessive hip flexion (typically >120 degrees) in a Pavlik harness can compress the femoral nerve against the inguinal ligament, leading to an iatrogenic femoral nerve palsy. Excessive hip abduction, on the other hand, compromises the medial circumflex femoral artery and leads to avascular necrosis.
Question 39:
A 30-year-old man with a comminuted tibial shaft fracture presents with severe pain out of proportion to the injury. Clinical suspicion for acute compartment syndrome is high. Which of the following pressure measurements strongly supports the need for an emergent fasciotomy?
Options:
- Absolute compartment pressure of 20 mmHg
- Absolute compartment pressure of 25 mmHg
- Delta pressure (Diastolic Blood Pressure minus Compartment Pressure) less than 30 mmHg
- Delta pressure (Mean Arterial Pressure minus Compartment Pressure) greater than 40 mmHg
- Compartment pressure equal to central venous pressure
Correct Answer: Delta pressure (Diastolic Blood Pressure minus Compartment Pressure) less than 30 mmHg
Explanation:
The most reliable indicator for diagnosing acute compartment syndrome in a borderline clinical scenario is the delta pressure, calculated as Diastolic Blood Pressure (DBP) minus Intracompartmental Pressure (ICP). A delta pressure of less than 30 mmHg (indicating critically compromised tissue perfusion) is an absolute indication for emergent fasciotomy.
Question 40:
A distal chevron osteotomy is generally considered the most appropriate surgical intervention for a patient with symptomatic hallux valgus possessing which of the following radiographic profiles?
Options:
- Intermetatarsal (IM) angle > 20 degrees
- Hallux valgus angle (HVA) > 40 degrees with a hypermobile first tarsometatarsal joint
- Intermetatarsal (IM) angle < 13 degrees and Hallux valgus angle (HVA) < 30 degrees
- First metatarsophalangeal joint severe osteoarthritis
- Metatarsus adductus with an IM angle > 15 degrees
Correct Answer: Intermetatarsal (IM) angle < 13 degrees and Hallux valgus angle (HVA) < 30 degrees
Explanation:
The distal chevron osteotomy is indicated for mild to moderate hallux valgus deformities. This corresponds to an Intermetatarsal (IM) angle of less than 13 to 15 degrees and a Hallux Valgus Angle (HVA) of less than 30 to 35 degrees. Severe deformities (IM > 15) or hypermobility typically require a proximal osteotomy or Lapidus procedure, and advanced MTP arthritis is a contraindication.
Question 41:
A 24-year-old gymnast presents with ulnar-sided wrist pain. Examination reveals a positive ballottement test (Reagan test). Radiographs show a volar flexed scaphoid and lunate with a dorsally extended triquetrum. What is the most likely diagnosis?
Options:
- Scapholunate dissociation (DISI)
- Lunotriquetral dissociation (VISI)
- Midcarpal instability
- Triangular fibrocartilage complex (TFCC) tear
- Perilunate dislocation
Correct Answer: Lunotriquetral dissociation (VISI)
Explanation:
Lunotriquetral (LT) ligament tears lead to Volar Intercalated Segment Instability (VISI). The lunate flexes with the scaphoid while the triquetrum extends. The Reagan test (LT ballottement) is positive. Scapholunate tears lead to DISI (Dorsal Intercalated Segment Instability).
Question 42:
A 15-year-old boy presents with progressive thoracic kyphosis. Lateral spine radiographs are obtained. According to Sorensen's criteria, which of the following is required for the definitive radiographic diagnosis of Scheuermann's disease?
Options:
- Anterior wedging of at least 5 degrees in one vertebra
- Anterior wedging of at least 5 degrees in three adjacent vertebrae
- Schmorl's nodes in at least two adjacent vertebrae
- A Cobb angle greater than 40 degrees with rigid apex
- Endplate irregularities in the lumbar spine only
Correct Answer: Anterior wedging of at least 5 degrees in three adjacent vertebrae
Explanation:
Sorensen's criteria for the diagnosis of Scheuermann's kyphosis require the presence of anterior wedging of >5 degrees in at least three consecutive (adjacent) vertebrae. Schmorl's nodes and endplate irregularities are commonly seen but are not the primary defining criteria.
Question 43:
In Posterior Cruciate Ligament (PCL) anatomy, which of the following statements accurately describes the biomechanical function of its bundles?
Options:
- The anterolateral bundle is tight in extension and lax in flexion.
- The posteromedial bundle is tight in flexion and lax in extension.
- The anterolateral bundle is the primary restraint to posterior tibial translation at 90 degrees of flexion.
- The posteromedial bundle is the primary restraint to posterior tibial translation at 90 degrees of flexion.
- Both bundles maintain constant tension throughout the arc of motion.
Correct Answer: The anterolateral bundle is the primary restraint to posterior tibial translation at 90 degrees of flexion.
Explanation:
The PCL has two main bundles: the larger anterolateral (AL) bundle and the smaller posteromedial (PM) bundle. The AL bundle is tight in flexion and lax in extension, serving as the primary restraint to posterior tibial translation at 90 degrees of flexion. The PM bundle is tight in extension and lax in flexion.
Question 44:
A 60-year-old patient undergoes revision of a metal-on-metal total hip arthroplasty due to an adverse local tissue reaction (ALTR). Which of the following histological findings is most characteristic of this specific implant-related failure?
Options:
- Extensive polymorphonuclear leukocyte infiltration
- Abundant polyethylene wear debris with macrophage reaction
- Aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL)
- Malignant transformation to synovial sarcoma
- Granulomatous inflammation with caseating necrosis
Correct Answer: Aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL)
Explanation:
Adverse local tissue reactions (ALTR) or adverse reactions to metal debris (ARMD) in metal-on-metal hips are characteristically associated with an Aseptic Lymphocyte-dominated Vasculitis-Associated Lesion (ALVAL), which represents a Type IV delayed hypersensitivity reaction to metal ions.
Question 45:
During the evaluation of a suspected Lisfranc injury, a 'fleck sign' is noted on the AP radiograph of the foot. This radiographic sign represents an avulsion of the Lisfranc ligament from which of the following osseous structures?
Options:
- Medial aspect of the second metatarsal base
- Lateral aspect of the medial cuneiform
- Plantar aspect of the navicular
- Dorsal aspect of the middle cuneiform
- Medial aspect of the cuboid
Correct Answer: Medial aspect of the second metatarsal base
Explanation:
The 'fleck sign' is an avulsion fracture at the attachment of the Lisfranc ligament. The Lisfranc ligament connects the lateral aspect of the medial cuneiform to the medial base of the second metatarsal. The avulsion fragment most commonly originates from the medial aspect of the second metatarsal base.
Question 46:
A 6-week-old female infant is undergoing an ultrasound evaluation for Developmental Dysplasia of the Hip (DDH). According to the Graf classification, what does the alpha angle measure and what is considered a normal value (Type I hip)?
Options:
- Measures the cartilaginous roof; normal is > 60 degrees
- Measures the cartilaginous roof; normal is < 55 degrees
- Measures the bony acetabular roof; normal is > 60 degrees
- Measures the bony acetabular roof; normal is < 55 degrees
- Measures the femoral head coverage; normal is > 50%
Correct Answer: Measures the bony acetabular roof; normal is > 60 degrees
Explanation:
In the Graf classification for DDH ultrasound, the alpha angle measures the bony roof of the acetabulum (formed by the ilium). A normal alpha angle (Graf Type I) is > 60 degrees. The beta angle measures the cartilaginous roof.
Question 47:
A 45-year-old patient presents with a painful cartilaginous lesion in the proximal femur. Which of the following histological features most reliably differentiates a low-grade (Grade 1) chondrosarcoma from a benign enchondroma?
Options:
- Presence of a cartilaginous matrix
- Binucleated chondrocytes
- Permeation and entrapment of host trabecular bone
- Myxoid degeneration of the stroma
- Lobular growth pattern
Correct Answer: Permeation and entrapment of host trabecular bone
Explanation:
Distinguishing enchondroma from low-grade chondrosarcoma can be challenging. The most reliable histological feature of low-grade chondrosarcoma is its infiltrative growth pattern, demonstrating permeation of the marrow space and entrapment of pre-existing host lamellar bone trabeculae.
Question 48:
In the pathogenesis of periprosthetic joint infection (PJI), bacteria establish a biofilm on the implant surface. Which molecular mechanism allows these bacteria to communicate and coordinate the gene expression necessary for biofilm maturation?
Options:
- Phagocytosis
- Chemotaxis
- Quorum sensing
- Opsonization
- Transduction
Correct Answer: Quorum sensing
Explanation:
Quorum sensing is a cell-to-cell communication mechanism used by bacteria to regulate gene expression in response to fluctuations in cell-population density. It is essential for the coordination and maturation of biofilms in periprosthetic joint infections.
Question 49:
A 35-year-old man sustains a 'terrible triad' injury of the elbow following a fall. When performing surgical stabilization, what is the generally accepted and most biomechanically sound sequence of repair?
Options:
- MCL repair, coronoid fixation, radial head fixation
- Coronoid fixation, radial head fixation/replacement, LCL repair
- LCL repair, MCL repair, radial head excision
- Radial head fixation, LCL repair, coronoid excision
- Coronoid fixation, MCL repair, LCL repair
Correct Answer: Coronoid fixation, radial head fixation/replacement, LCL repair
Explanation:
The standard surgical algorithm for a terrible triad injury (elbow dislocation, radial head fracture, coronoid fracture) works from deep to superficial and typically from medial to lateral: 1) Coronoid repair or fixation, 2) Radial head repair or replacement, 3) Lateral collateral ligament (LCL) repair. If the elbow remains unstable, MCL repair or an external fixator may be considered.
Question 50:
Adult acquired flatfoot deformity is often initiated by posterior tibial tendon dysfunction, leading to attenuation of the spring ligament complex. Which component of the spring ligament is the thickest, most clinically significant, and provides the primary static support to the talar head?
Options:
- Inferomedial calcaneonavicular ligament
- Plantar calcaneocuboid ligament
- Superomedial calcaneonavicular ligament
- Bifurcate ligament
- Long plantar ligament
Correct Answer: Superomedial calcaneonavicular ligament
Explanation:
The spring ligament complex consists of three main bands. The superomedial calcaneonavicular ligament is the thickest and most crucial component, providing primary static support to the talar head. Its attenuation allows plantar and medial migration of the talar head in adult acquired flatfoot deformity.
Question 51:
A 16-year-old gymnast with an L5-S1 isthmic spondylolisthesis develops progressively worsening radicular leg pain. Imaging reveals an L5 pars defect with a Grade II slip and significant foraminal stenosis. Which nerve root is most likely compressed, and where does the compression occur?
Options:
- L4 root, in the lateral recess
- L5 root, in the neural foramen
- S1 root, in the lateral recess
- S1 root, in the neural foramen
- S2 root, centrally
Correct Answer: L5 root, in the neural foramen
Explanation:
In L5-S1 isthmic spondylolisthesis, the exiting L5 nerve root is most commonly compressed within the neural foramen. The compression is typically caused by the hypertrophic fibrocartilaginous mass at the pars interarticularis defect (the 'Gill lesion').
Question 52:
During a total knee arthroplasty, after making standard bony cuts and inserting trial components, the surgeon notes that the joint is tight in full extension but perfectly balanced in 90 degrees of flexion. Which of the following is the most appropriate corrective action?
Options:
- Release the superficial medial collateral ligament
- Downsize the femoral component
- Increase the posterior slope of the tibial cut
- Resect additional bone from the distal femur
- Resect additional bone from the posterior femoral condyles
Correct Answer: Resect additional bone from the distal femur
Explanation:
A knee that is tight in extension but balanced in flexion indicates an asymmetric extension gap. To increase the extension gap without affecting the flexion gap, the surgeon should resect more distal femur or release the posterior capsule.
Question 53:
A 6-year-old boy sustains a completely displaced, extension-type supracondylar humerus fracture with posterolateral displacement of the distal fragment. On examination, he is unable to make an 'OK' sign. Which nerve is most likely injured?
Options:
- Radial nerve
- Ulnar nerve
- Anterior interosseous nerve (AIN)
- Musculocutaneous nerve
- Axillary nerve
Correct Answer: Anterior interosseous nerve (AIN)
Explanation:
The anterior interosseous nerve (AIN), a branch of the median nerve, is the most commonly injured nerve in extension-type supracondylar humerus fractures, particularly those with posterolateral displacement. The inability to flex the IP joint of the thumb and DIP joint of the index finger (the 'OK' sign) indicates AIN palsy.
Question 54:
According to the Young-Burgess classification of pelvic ring injuries, which of the following ligamentous disruptions distinguishes an Anteroposterior Compression III (APC III) injury from an APC II injury?
Options:
- Symphysis pubis
- Sacrospinous ligament
- Sacrotuberous ligament
- Anterior sacroiliac ligament
- Posterior sacroiliac ligament
Correct Answer: Posterior sacroiliac ligament
Explanation:
In the Young-Burgess classification, an APC II injury involves disruption of the pubic symphysis, anterior sacroiliac (SI) ligaments, and the sacrotuberous/sacrospinous ligaments, but the posterior SI ligaments remain intact. An APC III injury involves complete disruption of both the anterior and posterior SI ligaments, resulting in complete spinopelvic dissociation.
Question 55:
A 42-year-old female presents with volar forearm pain and numbness in her thumb, index, and middle fingers. The physician suspects Pronator Syndrome rather than Carpal Tunnel Syndrome (CTS). Which clinical finding strongly supports a diagnosis of Pronator Syndrome over CTS?
Options:
- A positive Tinel's sign at the wrist
- Atrophy of the thenar eminence
- Decreased sensation over the thenar eminence
- Worsening of symptoms at night
- Positive Phalen's test
Correct Answer: Decreased sensation over the thenar eminence
Explanation:
The palmar cutaneous branch of the median nerve provides sensation to the thenar eminence and branches off proximal to the carpal tunnel. Sensation over the thenar eminence is preserved in Carpal Tunnel Syndrome but is decreased in proximal median nerve entrapment neuropathies like Pronator Syndrome.
Question 56:
A 20-year-old man presents with nocturnal thigh pain that is completely relieved by ibuprofen. Imaging shows a 1 cm radiolucent nidus with surrounding sclerosis in the femoral diaphysis. What is the primary biochemical mechanism underlying the effectiveness of NSAIDs for this specific lesion?
Options:
- Reduction of interleukin-6 production
- Inhibition of excessive cyclooxygenase-2 (COX-2) expression by the nidus
- Direct suppression of osteoclast activity
- Inhibition of vascular endothelial growth factor (VEGF)
- Blockade of substance P release in the periosteum
Correct Answer: Inhibition of excessive cyclooxygenase-2 (COX-2) expression by the nidus
Explanation:
Osteoid osteomas characteristically cause severe nocturnal pain that is relieved by NSAIDs. This is because the nidus cells produce high levels of prostaglandins (specifically PGE2) due to marked expression of cyclooxygenase-2 (COX-2) enzymes. NSAIDs inhibit this COX-2 activity, directly eliminating the source of the pain.
Question 57:
During biomechanical testing of a tendon graft, the graft is rapidly stretched to a specific length and held at that constant length. Over time, the force required to maintain that length progressively decreases. This viscoelastic property is termed:
Options:
- Creep
- Stress relaxation
- Hysteresis
- Fatigue failure
- Isotropy
Correct Answer: Stress relaxation
Explanation:
Stress relaxation is the decrease in stress (force) over time when a viscoelastic material is held at a constant strain (length). Creep is the progressive increase in strain (length) over time when the material is held at a constant stress (load).
Question 58:
In the Snyder classification of Superior Labrum Anterior and Posterior (SLAP) lesions, a Type II tear is defined by which of the following characteristics?
Options:
- Fraying of the superior labrum with an intact biceps anchor
- Detachment of the superior labrum and biceps anchor from the superior glenoid
- A bucket-handle tear of the superior labrum with an intact biceps anchor
- A bucket-handle tear of the superior labrum with detachment of the biceps anchor
- An anterior labral tear extending into the middle glenohumeral ligament
Correct Answer: Detachment of the superior labrum and biceps anchor from the superior glenoid
Explanation:
The Snyder classification describes SLAP tears: Type I is fraying of the superior labrum with an intact anchor. Type II is detachment of the superior labrum and biceps anchor from the glenoid. Type III is a bucket-handle tear of the labrum with an intact anchor. Type IV is a bucket-handle tear extending into the biceps tendon.
Question 59:
According to the American Society for Bone and Mineral Research (ASBMR) criteria, which of the following is a REQUIRED major radiographic feature for the diagnosis of an atypical femur fracture (AFF) associated with prolonged bisphosphonate use?
Options:
- Fracture line originates at the medial cortex
- Spiral fracture morphology
- Location exclusively in the femoral neck
- Transverse or short oblique configuration originating at the lateral cortex
- Extensive comminution
Correct Answer: Transverse or short oblique configuration originating at the lateral cortex
Explanation:
ASBMR major criteria for an atypical femur fracture include: location along the femoral diaphysis from just distal to the lesser trochanter to just proximal to the supracondylar flare, a transverse or short oblique fracture line originating at the lateral cortex, noncomminuted or minimally comminuted, and often a localized periosteal reaction of the lateral cortex ('beaking').
Question 60:
A 35-year-old recreational athlete sustains an acute Achilles tendon rupture. The injury most commonly occurs in a hypovascular 'watershed' region. Where is this region anatomically located relative to the calcaneal insertion?
Options:
- 0 to 1 cm proximal
- 2 to 6 cm proximal
- 7 to 10 cm proximal
- At the musculotendinous junction
- At the calcaneal tuberosity
Correct Answer: 2 to 6 cm proximal
Explanation:
The Achilles tendon receives its blood supply from the paratenon and osseous insertions, but it has a relatively hypovascular 'watershed' zone located approximately 2 to 6 cm proximal to its insertion on the calcaneus. This is the most common site for degenerative changes and acute ruptures.