Introduction & Epidemiology
The femur, the longest and strongest bone in the human body, is frequently subjected to high-energy trauma, resulting in a wide spectrum of fractures, from simple non-displaced patterns to complex, comminuted, and open injuries. Beyond trauma, the femur is also the site for elective surgical interventions including tumor resections, osteotomies for deformity correction, and arthroplasty procedures. Mastery of surgical approaches to the femur is paramount for orthopedic surgeons, residents, and medical students alike, enabling optimal exposure, meticulous reduction, and stable fixation while minimizing iatrogenic soft tissue and neurovascular injury.
Femoral fractures represent a significant public health burden. Proximal femur fractures, including femoral neck and intertrochanteric fractures, are particularly prevalent in the elderly osteoporotic population, with an incidence projected to rise globally due to demographic shifts. Femoral shaft fractures typically occur in younger individuals due to high-energy mechanisms (e.g., motor vehicle collisions) and are often associated with polytrauma. Distal femur fractures, including supracondylar and intercondylar types, occur in both young, high-energy trauma patients and elderly individuals with osteoporotic bone following low-energy falls. The epidemiological landscape underscores the necessity for a comprehensive understanding of surgical approaches to address these diverse presentations effectively.
Surgical Anatomy & Biomechanics
A profound understanding of femoral surgical anatomy and biomechanics is foundational to successful outcomes.
Femoral Anatomy
The femur is broadly divided into three regions:
*
Proximal Femur:
Comprises the femoral head, neck, greater trochanter, lesser trochanter, and intertrochanteric line/crest. Key landmarks include the piriformis fossa (common entry point for antegrade intramedullary nailing) and the trochanteric fossa. The blood supply to the femoral head, critical in femoral neck fractures, primarily derives from the medial and lateral circumflex femoral arteries via the retinacular vessels, with a contribution from the artery of the ligamentum teres in children.
*
Femoral Shaft:
The diaphysis, extending from just distal to the lesser trochanter to the flare of the condyles. It has a triangular cross-section proximally, becoming more cylindrical mid-shaft, and then more rectangular distally. The linea aspera, a prominent longitudinal ridge on the posterior aspect, serves as the attachment for vastus medialis, lateralis, and adductor muscles. The nutrient artery enters mid-shaft, often through the linea aspera, emphasizing the importance of preserving the periosteum during exposure.
*
Distal Femur:
Characterized by the medial and lateral femoral condyles, intercondylar notch, patellar trochlea, and medial and lateral epicondyles. The supracondylar region is the metaphyseal-diaphyseal junction. The posterior aspect features the popliteal surface and adductor tubercle. The articular cartilage of the condyles is crucial for knee joint function.
Neurovascular Structures
Understanding the relative position of neurovascular bundles to the femur is critical to avoid iatrogenic injury during surgical exposure:
*
Femoral Nerve:
Lies lateral to the femoral artery in the femoral triangle, innervating the quadriceps femoris. At risk during anterior and anteromedial approaches to the proximal and mid-femur.
*
Sciatic Nerve:
Exits the pelvis through the greater sciatic foramen, runs deep to the gluteus maximus, and descends posteromedially in the thigh. Divides into tibial and common peroneal nerves in the distal thigh. At risk during posterior and posterolateral approaches, particularly to the proximal and mid-femur.
*
Lateral Femoral Cutaneous Nerve (LFCN):
Crosses the iliac crest medial to the ASIS, often passing through or under the inguinal ligament. Supplies sensation to the lateral thigh. Highly variable course and very susceptible to injury or compression during anterior approaches to the hip/proximal femur.
*
Common Peroneal Nerve:
A branch of the sciatic nerve, courses laterally around the fibular neck. At risk during posterolateral and lateral approaches to the distal femur and knee.
*
Saphenous Nerve:
A terminal sensory branch of the femoral nerve, descends through the adductor canal with the femoral artery and vein. At risk during medial and anteromedial approaches to the distal femur.
*
Femoral Artery/Vein:
Traverse the femoral triangle and adductor canal. Profunda femoris artery branches supply the majority of the femoral diaphysis via perforating arteries. At risk during anteromedial and medial approaches.
*
Popliteal Artery/Vein:
Continuation of the femoral vessels, lying deep in the popliteal fossa. At significant risk during posterior approaches to the distal femur and knee, especially with fracture displacement.
Musculature & Internervous Planes
Optimal surgical approaches exploit internervous planes to minimize muscle damage and preserve function.
*
Proximal Femur:
*
Anterior:
Between tensor fasciae latae (superior gluteal nerve) and sartorius/rectus femoris (femoral nerve).
*
Anterolateral (Modified Hardinge/Watson-Jones):
Between gluteus medius/minimus (superior gluteal nerve) and vastus lateralis (femoral nerve).
*
Femoral Shaft:
*
Lateral:
Vastus lateralis muscle splitting approach, no true internervous plane.
*
Posteromedial:
Between adductor magnus (obturator and sciatic nerves) and vastus medialis (femoral nerve).
*
Distal Femur:
*
Lateral Subvastus:
Retracts vastus lateralis (femoral nerve) anteriorly. No true internervous plane.
*
Medial Subvastus:
Retracts vastus medialis (femoral nerve) anteriorly. No true internervous plane.
*
Anteromedial:
Between sartorius (femoral nerve) and vastus medialis (femoral nerve) or adductor magnus (obturator nerve).
*
Posterior:
Between hamstrings (sciatic nerve) and vastus lateralis/medialis (femoral nerve).
*
Posterolateral:
Between biceps femoris (sciatic nerve - common peroneal component) and vastus lateralis (femoral nerve).
Biomechanics
The femur withstands substantial compressive, tensile, and torsional forces.
*
Load Bearing:
Under physiological loading, the femoral shaft experiences compressive forces medially and tensile forces laterally.
*
Fracture Patterns:
The bone's biomechanical properties influence fracture patterns (transverse, oblique, spiral, comminuted, segmental).
*
Fixation Principles:
Understanding stress distribution guides implant selection and placement (e.g., tension banding, bridging, absolute stability). For example, intramedullary nails are load-sharing devices, while plates can be load-bearing or load-sharing depending on construct.
Indications & Contraindications
The decision-making process for surgical intervention on the femur involves a thorough assessment of the patient's overall health, fracture characteristics, and anticipated functional demands.
Indications for Operative Management
- Femoral Neck Fractures: Displaced fractures (Garden III/IV), young patients, pathological fractures.
- Intertrochanteric Fractures: Most displaced intertrochanteric fractures, unstable patterns (reverse obliquity, subtrochanteric extension).
- Subtrochanteric Fractures: All displaced subtrochanteric fractures due to high muscular forces causing instability.
- Femoral Shaft Fractures: All displaced adult femoral shaft fractures, open fractures, multiple trauma patients (damage control orthopedics), pathological fractures.
- Distal Femur Fractures: Displaced supracondylar and intercondylar fractures, open fractures, fractures with articular involvement.
- Periprosthetic Fractures: Many require surgical stabilization depending on fracture pattern and implant stability (Vancouver classification).
- Non-unions/Malunions: Symptomatic non-unions or malunions requiring revision fixation or corrective osteotomy.
- Tumors/Lesions: Biopsy, resection, and reconstruction for primary or metastatic bone tumors.
- Deformity Correction: Corrective osteotomies for limb length discrepancy or angular deformities.
Contraindications for Operative Management
Contraindications are often relative and depend on the specific surgical context, patient comorbidities, and anticipated benefits versus risks.
*
Absolute Contraindications (rare for necessary trauma surgery):
* Uncontrolled systemic infection (sepsis).
* Severe, uncorrectable coagulopathy.
* Patient not medically stable for anesthesia and surgery (e.g., uncontrolled cardiac failure, severe respiratory distress).
*
Relative Contraindications:
* Extreme medical comorbidities (ASA III/IV) that significantly increase anesthetic and surgical risk, where non-operative management might be safer (e.g., highly frail, terminally ill patient with minimal functional demands).
* Severe local soft tissue compromise (e.g., extensive degloving, devitalized tissue, severe contamination) which may necessitate staged management or external fixation.
* Active local infection (cellulitis, osteomyelitis) which may require treatment prior to definitive internal fixation.
* Non-displaced, stable fractures in very low-demand patients (e.g., some non-displaced distal femur fractures or stable intertrochanteric fractures).
* Poor bone quality (severe osteoporosis) that may preclude stable fixation with standard implants; may require cement augmentation or different fixation strategies.
* Patient refusal.
Operative vs. Non-Operative Indications
| Fracture Type | Primary Operative Indication | Primary Non-Operative Indication |
|---|---|---|
| Femoral Neck Fx | Displaced (Garden III/IV), Young Patient, Pathological | Non-displaced, Impacted (Garden I/II), Stable Elderly Patient (rare) |
| Intertrochanteric Fx | Unstable patterns (reverse obliquity), Displaced | Stable, non-displaced (rarely, e.g., in non-ambulators) |
| Subtrochanteric Fx | All displaced fractures | Rarely, if ever |
| Femoral Shaft Fx (Adult) | All displaced fractures, Open fractures, Polytrauma | Rarely, if ever (e.g., stress fracture, stable incomplete) |
| Distal Femur Fx | Displaced supracondylar/intercondylar, Articular involvement | Stable, non-displaced, extra-articular (e.g., cast/brace in select cases) |
| Periprosthetic Fx | Displaced, Unstable implant, Fracture around implant | Stable, non-displaced, implant stable (Vancouver A or C, B1 stable) |
| Pathological Fx | Displaced, impending fracture (prophylactic fixation) | Non-displaced, stable, non-impending (often with radiation) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for successful outcomes, minimizing operative time, reducing complications, and ensuring optimal implant placement.
Pre-Operative Planning
- Clinical Assessment: Thorough history and physical examination, focusing on neurovascular status, soft tissue integrity, comorbidities, and functional baseline.
-
Imaging Review:
- Standard Radiographs: AP and lateral views of the entire femur, including hip and knee joints. Traction views, if appropriate, can aid in assessing fracture reducibility.
- Computed Tomography (CT): Essential for complex intra-articular fractures (femoral head, distal femur), comminuted patterns, bone loss, and pre-operative templating of osteotomies or tumor resections. CT angiography may be necessary for suspected vascular injury.
- Magnetic Resonance Imaging (MRI): Useful for assessing soft tissue injury, ligamentous injury (knee), occult fractures (e.g., stress fractures, osteonecrosis), and tumor staging.
-
Templating:
- Using digital or physical templates, determine appropriate implant length, diameter, and trajectory (e.g., intramedullary nail), or plate length and screw trajectory.
- Anticipate points of maximal bow or deformity correction required.
- For arthroplasty, plan component size, alignment, and leg length.
-
Surgical Strategy:
- Define the most appropriate surgical approach based on fracture location, pattern, and surgeon preference.
- Anticipate reduction maneuvers (indirect vs. direct, use of traction, clamps, joysticks).
- Consider sequence of reduction and fixation steps.
- Plan for bone grafting or augmentation if needed.
- Prepare for potential complications and backup plans.
- Equipment Preparation: Ensure all necessary instruments, implants, fluoroscopy unit, and specialized tables are available and functional.
Patient Positioning
Proper positioning optimizes exposure, facilitates reduction, allows fluoroscopic access, and protects peripheral nerves and soft tissues.
1.
Supine Position:
*
Indications:
Most femoral shaft fractures for antegrade or retrograde intramedullary nailing, distal femur fractures, some proximal femur fractures, direct anterior approach to hip.
*
Setup:
Patient lies on their back. For shaft fractures, often on a fracture table with traction applied to the operative leg, while the contralateral leg is abducted and flexed to allow C-arm access. Careful padding of sacrum, heels, and peroneal nerve at fibular head.
*
Considerations:
Allows for easy C-arm access for AP and lateral views of the hip, shaft, and knee. Requires careful handling of the limb for rotational control.
2.
Lateral Decubitus Position:
*
Indications:
Anterolateral (Modified Hardinge) approach to hip/proximal femur, posterior approaches to hip, some posterolateral approaches to distal femur.
*
Setup:
Patient lies on their side, secured with beanbag or bolsters. Axillary roll placed to protect brachial plexus. Pillows between knees.
*
Considerations:
Offers excellent exposure for the hip, allows for manipulation of the femur. C-arm access may be more challenging than supine, often requiring specific positioning.
3.
Prone Position:
*
Indications:
Posterior approaches to the distal femur, some posterior approaches to hip/proximal femur, or challenging antegrade IMN requiring extreme hip extension/adduction.
*
Setup:
Patient lies face down on chest rolls/bolsters to allow respiratory excursion. Padding for face, elbows, knees, and feet.
*
Considerations:
Provides direct access to the posterior aspect of the femur. C-arm access to the distal femur/knee can be challenging, often requiring oblique views. Significant risk of popliteal neurovascular injury.
4.
Beach Chair Position:
*
Indications:
Primarily for shoulder surgery, but can be adapted for hip arthroscopy; not a primary position for femoral shaft/distal femur approaches.
*
Setup:
Patient semi-recumbent.
5.
Limb Draping:
Ensure sufficient sterile field to allow for manipulation of the entire limb, including hip and knee, to facilitate reduction and C-arm imaging.
Detailed Surgical Approach / Technique
This section will detail the common surgical approaches to the femur, emphasizing step-by-step dissection, internervous planes, and relevant anatomical considerations.
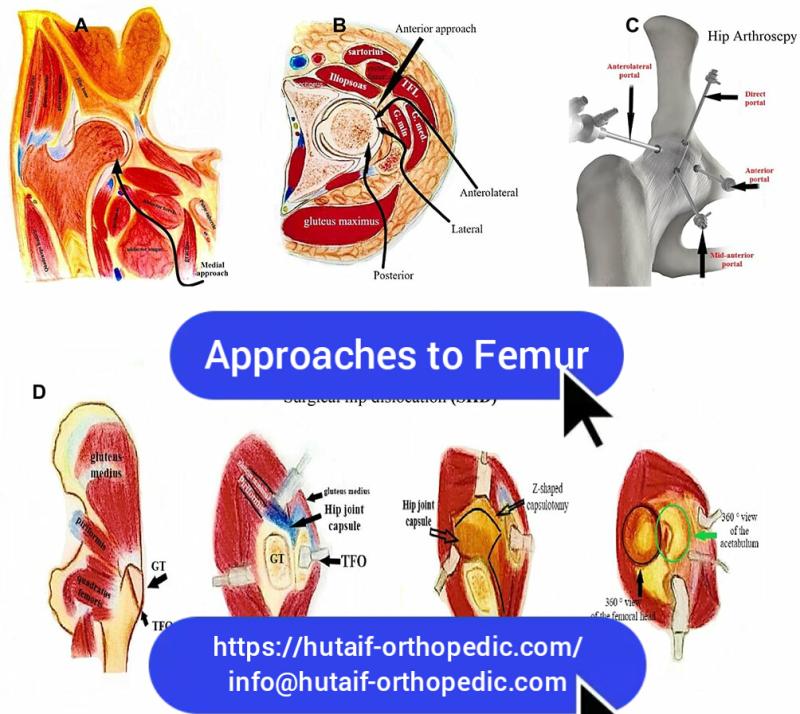
A. Approaches to the Proximal Femur
1. Direct Lateral Approach (for Antegrade Intramedullary Nailing)
- Indications: Femoral shaft fractures, subtrochanteric fractures, intertrochanteric fractures, femoral neck fractures (in conjunction with nailing).
- Positioning: Supine on a fracture table or radiolucent table with the operative leg abducted and internally rotated as needed for nail entry.
- Incision: Longitudinal incision, typically 4-6 cm, centered over the tip of the greater trochanter, extending proximally and distally.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Incise the fascia lata longitudinally in line with the skin incision.
- Palpate the tip of the greater trochanter. Split the underlying gluteus medius and minimus muscles bluntly or sharply. The goal is to reach the piriformis fossa or the tip of the greater trochanter, depending on the chosen nail entry portal.
- Expose the bone. Use an awl or drill to create the entry portal for the intramedullary nail.
- Internervous Plane: Primarily a muscle-splitting approach through the gluteus medius/minimus; no true internervous plane.
- Neurovascular Risk: Minimal. Care should be taken to avoid excessive posterior retraction which could theoretically injure the sciatic nerve.
2. Anterolateral Approach (Modified Hardinge / Watson-Jones)
- Indications: Total hip arthroplasty (THA), femoral neck fractures, intertrochanteric fractures, open reduction of hip dislocations.
- Positioning: Lateral decubitus or supine with the operative hip slightly flexed.
- Incision: Longitudinal curvilinear incision, beginning 3-4 cm distal to the ASIS, extending distally along the anterior aspect of the greater trochanter, then curving slightly posterior over the greater trochanter for approximately 8-10 cm.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Incise the fascia lata in line with the skin incision, exposing the underlying tensor fasciae latae muscle.
- Identify the anterior border of the gluteus medius. Develop the interval between the tensor fasciae latae (supplied by superior gluteal nerve) and the gluteus medius (also superior gluteal nerve). This is a muscle-sparing interval rather than a true internervous plane.
- Retract the gluteus medius superiorly/posteriorly and the tensor fasciae latae/vastus lateralis anteriorly.
- The vastus lateralis can be partially elevated off the greater trochanter and lateral femur or split longitudinally to expose the femoral neck and proximal femur.
- The joint capsule can then be incised to access the femoral head and neck.
- Internervous Plane: Between tensor fasciae latae and gluteus medius (both superior gluteal nerve supply, so not a true internervous plane, but a functional muscle-sparing interval).
- Neurovascular Risk: Superior gluteal nerve (risk of injury to motor branches with excessive posterior retraction or stripping of gluteus medius). Lateral femoral cutaneous nerve (LFCN) is at minimal risk with this incision, but can be damaged with more anterior approaches.
3. Direct Anterior Approach (DAA)
- Indications: THA, internal fixation of some femoral neck fractures.
- Positioning: Supine, often on a specialized table (e.g., fracture table) to facilitate positioning and limb manipulation.
- Incision: Longitudinal incision, typically 8-10 cm, centered on the interval between the ASIS and the lateral aspect of the patella. It starts distal to the ASIS and runs parallel to the axis of the femur.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Identify the interval between the tensor fasciae latae (TFL, superior gluteal nerve) laterally and the sartorius/rectus femoris (femoral nerve) medially. This is the first internervous plane.
- Retract the TFL laterally and sartorius/rectus femoris medially.
- Deep to this, identify the second internervous plane between the gluteus medius/minimus (superior gluteal nerve) laterally and the rectus femoris/iliopsoas (femoral nerve) medially.
- Retract these muscles to expose the anterior hip capsule, which can then be incised.
- Internervous Plane: Between tensor fasciae latae (superior gluteal nerve) and sartorius/rectus femoris (femoral nerve). Deeply, between gluteus medius/minimus (superior gluteal nerve) and rectus femoris/iliopsoas (femoral nerve).
- Neurovascular Risk: Lateral femoral cutaneous nerve (LFCN) is highly vulnerable to injury or traction neuropraxia due to its variable course near the ASIS and incision. Femoral nerve and vessels are medial and deep but can be at risk with excessive medial retraction.
B. Approaches to the Femoral Shaft
1. Lateral Approach to Femoral Shaft
- Indications: Plating of femoral shaft fractures, revision intramedullary nailing (especially for implant removal), tumor resection.
- Positioning: Supine on a standard radiolucent table or fracture table.
- Incision: Longitudinal incision centered over the lateral aspect of the femoral shaft, extending proximally and distally to encompass the fracture site.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Incise the fascia lata in line with the skin incision.
- Identify the vastus lateralis muscle. This approach is typically muscle-splitting through the vastus lateralis, directly down to the lateral femoral cortex. Alternatively, a subvastus approach can be used, elevating the vastus lateralis anteriorly off the lateral intermuscular septum.
- Expose the periosteum of the lateral femur. Subperiosteal dissection is then performed to expose the fracture.
- Internervous Plane: No true internervous plane for the transvastus approach (muscle splitting). For the subvastus approach, the plane is deep to the vastus lateralis.
- Neurovascular Risk: Perforating branches of the profunda femoris artery and vein, which pierce the vastus lateralis to reach the posterior compartment, can be encountered and require ligation. Care to preserve nutrient artery if possible.
2. Minimally Invasive Approaches for Intramedullary Nailing (IMN)
- Indications: The gold standard for most femoral shaft fractures (antegrade IMN) and increasingly for distal femur fractures (retrograde IMN).
-
Antegrade IMN (Proximal Femur Entry):
- Positioning: Supine on a fracture table or radiolucent table. The operative leg is typically adducted and internally rotated for optimal entry portal access to the piriformis fossa or greater trochanter.
- Incision: Small longitudinal incision (2-4 cm) over the tip of the greater trochanter or piriformis fossa, guided by fluoroscopy.
-
Dissection:
- Skin, subcutaneous tissue, and fascia lata are incised.
- A blunt approach is made through the gluteus medius/minimus to the chosen entry portal on the greater trochanter or piriformis fossa.
- An awl or specialized guide pin and drill are used to create the entry portal into the medullary canal.
- Neurovascular Risk: Minimal.
-
Retrograde IMN (Distal Femur Entry):
- Indications: Distal femur fractures (supracondylar/intercondylar), ipsilateral tibia fractures (floating knee), polytrauma.
- Positioning: Supine, with the knee flexed to 90 degrees or more (supported by a bolster or leg holder) to expose the intercondylar notch.
- Incision: A small longitudinal incision (2-4 cm) is made, typically a parapatellar approach (medial or lateral to patellar tendon) or a transpatellar approach (through the patellar tendon).
-
Dissection:
- Skin, subcutaneous tissue are incised.
- A mini-arthrotomy is performed, or the patellar tendon is split.
- The entry portal is created in the intercondylar notch or just anterior to the origin of the PCL, aiming for the intramedullary canal, under fluoroscopic guidance.
- Neurovascular Risk: Popliteal artery and vein (posterior to the knee) are at risk with overly deep or posterior drilling/reaming. Common peroneal nerve (laterally).
C. Approaches to the Distal Femur
1. Lateral Parapatellar Approach / Lateral Subvastus Approach
- Indications: Plating of distal femur fractures (supracondylar, intercondylar), especially for lateral locked plating.
- Positioning: Supine, with the knee slightly flexed over a bolster to relax the quadriceps.
- Incision: Longitudinal incision, typically 15-20 cm, starting 2-3 cm proximal to the lateral epicondyle and extending proximally along the lateral aspect of the thigh.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Incise the fascia lata.
- Lateral Subvastus Approach: Identify the vastus lateralis muscle. Carefully incise its investing fascia and elevate the vastus lateralis muscle anteriorly off the lateral intermuscular septum. This preserves its innervation and blood supply. This exposes the lateral femoral shaft and lateral aspect of the condyle.
- Lateral Parapatellar (Transvastus) Approach: If the subvastus plane is difficult or insufficient, the vastus lateralis can be longitudinally split (transvastus) to expose the lateral femur.
- Internervous Plane: No true internervous plane for subvastus (muscle elevation). For transvastus, it's a muscle-splitting approach.
- Neurovascular Risk: Minimal, but perforating vessels from the profunda femoris require careful ligation or cauterization.
2. Medial Parapatellar Approach / Medial Subvastus Approach
- Indications: Less common for standard distal femur plating, but useful for medial condylar fractures, complex bicondylar fractures (often as a secondary approach), or for specific medial plating.
- Positioning: Supine, knee flexed over a bolster.
- Incision: Longitudinal incision, starting 2-3 cm proximal to the medial epicondyle and extending proximally along the medial aspect of the thigh.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Incise the fascia.
- Medial Subvastus Approach: Identify the vastus medialis muscle. Carefully elevate it anteriorly off the medial intermuscular septum. This exposes the medial femoral shaft and medial aspect of the condyle.
- Internervous Plane: No true internervous plane (muscle elevation).
- Neurovascular Risk: Saphenous nerve (sensory) and saphenous vein, which lie superficial or within the fascia in this region. Femoral artery and vein are more anterior and deep, within the adductor canal, but care is needed with deep dissection.
3. Anteromedial Approach to the Distal Two-thirds of the Femur
- Indications: Used for medial access to the distal femoral shaft and supracondylar region, often for osteotomies, tumor resections, or very specific plating. Can be combined with a lateral approach for bicondylar fractures.
- Positioning: Supine, with the hip slightly flexed and externally rotated, knee flexed over a bolster.
- Incision: Longitudinal incision along the anteromedial aspect of the thigh, extending from the adductor tubercle proximally.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Incise the fascia. Identify the sartorius muscle (femoral nerve) and retract it posteriorly and medially.
- Deep to the sartorius, identify the vastus medialis muscle (femoral nerve). Retract the vastus medialis anteriorly.
- This exposes the adductor canal (containing the femoral artery, vein, and saphenous nerve) lying on the adductor magnus (obturator and sciatic nerve). The neurovascular bundle must be carefully protected and retracted.
- The medial aspect of the distal femur is then exposed.
- Internervous Plane: Between sartorius (femoral nerve) and vastus medialis (femoral nerve) or adductor magnus (obturator/sciatic nerve).
- Neurovascular Risk: Femoral artery and vein, and saphenous nerve in the adductor canal are highly vulnerable. Careful blunt dissection and retraction are paramount.
4. Posterior Approach to the Distal Femur (e.g., Campbell's posterior approach)
- Indications: Posterior condylar fractures, posterior osteotomy, some tumor resections. Less common than anterior/lateral for trauma due to significant neurovascular risk.
- Positioning: Prone, with the knee slightly flexed.
- Incision: Longitudinal incision in the midline of the distal posterior thigh, extending into the popliteal fossa.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Incise the deep fascia.
- Develop the interval between the two heads of the gastrocnemius.
- Carefully dissect through the interval between the hamstrings (medial: semimembranosus/semitendinosus; lateral: biceps femoris) and the vastus lateralis/medialis.
- The popliteal neurovascular bundle (popliteal artery, vein, tibial nerve) lies deep and must be meticulously identified and retracted anteriorly.
- The posterior aspect of the distal femur is then exposed.
- Internervous Plane: Between the hamstrings (sciatic nerve branches) and the vastus muscles (femoral nerve).
- Neurovascular Risk: High risk of injury to the popliteal artery, popliteal vein, and tibial nerve. The common peroneal nerve is also at risk laterally. Requires extensive anatomical knowledge and meticulous dissection.
5. Posterolateral Approach to the Distal Femur
- Indications: Plating of posterolateral condylar fractures, fixation of posterior femoral condyle fragments.
- Positioning: Supine with the leg draped free for manipulation, or lateral decubitus.
- Incision: Longitudinal incision along the posterolateral aspect of the distal thigh, posterior to the iliotibial band.
-
Dissection:
- Incise skin and subcutaneous tissue.
- Incise the fascia lata.
- Identify the interval between the biceps femoris (long head: tibial nerve; short head: common peroneal nerve) posteriorly and the vastus lateralis (femoral nerve) anteriorly.
- Carefully develop this plane, retracting the biceps femoris posteriorly and the vastus lateralis anteriorly.
- The common peroneal nerve is superficial and laterally located in this region; it must be identified and protected.
- Exposure of the posterolateral distal femur.
- Internervous Plane: Between biceps femoris (sciatic nerve branches) and vastus lateralis (femoral nerve).
- Neurovascular Risk: Common peroneal nerve is highly vulnerable. Careful identification and protection are essential.
Complications & Management
Surgical intervention on the femur, while often limb and life-saving, carries inherent risks. A thorough understanding of potential complications and their management is crucial for optimal patient care.
General Surgical Complications
-
Infection (Deep Surgical Site Infection):
Incidence 1-5% for closed fractures, higher for open fractures.
- Management: Prompt surgical debridement, extensive irrigation, deep tissue cultures, systemic broad-spectrum antibiotics, potential implant removal and staged reconstruction for chronic infections. Negative pressure wound therapy.
-
Bleeding / Hematoma:
Significant blood loss can occur, especially in high-energy trauma.
- Management: Meticulous hemostasis, drains, transfusion (if symptomatic anemia), re-exploration for expanding hematoma.
-
Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE):
Incidence 1-5% for PE, higher for DVT.
- Management: Prophylactic anticoagulation (chemical and mechanical), early mobilization. Treatment with therapeutic anticoagulation for confirmed DVT/PE.
-
Nerve Injury:
Direct trauma during dissection, traction injury, compression, or entrapment.
- Management: Prevention through careful anatomical dissection. Observation for neuropraxia. Neurolysis or repair for transection.
-
Vascular Injury:
Laceration or thrombosis of major vessels (e.g., femoral, popliteal).
- Management: Immediate recognition, vascular surgery consultation, repair or grafting.
Approach- and Fracture-Specific Complications
| Complication | Incidence | Salvage/Management Strategy |
|---|---|---|
| Non-union (Femoral Shaft) | 5-15% | Revision fixation (nail exchange with reaming, plate augmentation), bone grafting (autograft/allograft), biologic augmentation (BMPs, PRP), pulsed electromagnetic fields. |
| Malunion (Femoral Shaft) | Up to 30% (rotational, clinical) | Corrective osteotomy (if symptomatic and functional deficit), often with new internal fixation. |
| Avascular Necrosis (Femoral Head) | 10-30% (displaced femoral neck fx) | Early: Core decompression, vascularized fibula graft. Late: Total hip arthroplasty (THA). |
| Trochanteric Pain/Bursitis | 10-20% (post IMN) | Conservative (NSAIDs, PT, steroid injections), implant removal (prominent nail/screws), bursectomy. |
| Superior Gluteal Nerve Injury | <5% (Anterolateral approaches) | Conservative management, physical therapy. Tendon transfer (e.g., gluteus maximus to greater trochanter) for persistent abductor weakness. |
| Lateral Femoral Cutaneous Nerve Injury | 10-20% (DAA) | Conservative (observation for neuropraxia, pain medications). Neurolysis or neurectomy for persistent, debilitating neuropathic pain. |
| Popliteal Artery Injury | <1% (Distal Femur Fx, Retrograde IMN) | Immediate vascular surgery consultation, arterial repair/grafting, fasciotomy for compartment syndrome. Limb salvage. |
| Common Peroneal Nerve Palsy | 2-5% (Distal Femur Fx, traction) | Conservative (foot drop orthosis). Neurolysis or nerve repair if indicated. Tendon transfer for chronic deficits. |
| Knee Stiffness / Arthrofibrosis (Distal Femur) | 20-40% | Aggressive physical therapy, continuous passive motion (CPM), manipulation under anesthesia (MUA), arthroscopic or open arthrolysis. |
| Deep Vein Thrombosis (DVT) | 10-40% (without prophylaxis) | Anticoagulation (LMWH, DOACs). IVC filter for contraindication to anticoagulation. |
| Heterotopic Ossification (HO) | Variable (high in head injuries) | Prophylaxis (NSAIDs, radiation therapy in high-risk patients). Excision if symptomatic and mature. |
| Implant Failure | <5% | Revision surgery with stronger fixation, different implant type, or bone grafting to promote healing. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral component of the overall treatment plan, aiming to restore function, prevent stiffness, and facilitate a safe return to activities. Protocols are individualized based on fracture stability, fixation type, patient comorbidities, and functional goals.
General Principles
- Pain Management: Multimodal analgesia to facilitate early mobility and participation in therapy.
- Wound Care: Meticulous wound management to prevent infection.
- Early Mobilization: As tolerated and dictated by fixation stability. Reduces DVT/PE risk, prevents stiffness, and improves patient morale.
-
Progressive Weight-Bearing (PWB):
Gradual increase in weight through the operative limb.
- Non-weight-bearing (NWB): No weight through the limb.
- Touch-down weight-bearing (TDWB): Foot contacts ground for balance only (5-10 kg).
- Partial weight-bearing (PWB): A specified percentage of body weight, gradually increasing.
- Weight-bearing as tolerated (WBAT): Patient determines comfortable weight-bearing.
- Range of Motion (ROM): Active, active-assisted, and passive exercises to prevent arthrofibrosis.
- Strengthening: Progressive resistance exercises for surrounding musculature.
- Functional Training: Gait training, balance exercises, activities of daily living (ADLs).
Region-Specific Rehabilitation Considerations
1. Proximal Femur (Femoral Neck, Intertrochanteric, Subtrochanteric Fractures)
-
Initial Phase (0-6 weeks):
-
Weight-Bearing:
- Femoral Neck (IFN): Often TDWB to PWB for stable fixation; WBAT for young patients with stable fixation; NWB for unstable fixation or specific arthroplasty protocols.
- Intertrochanteric/Subtrochanteric (IMN/Plate): Often WBAT due to stable intramedullary fixation. PWB for highly comminuted or unstable plate fixation.
- ROM: Gentle active and passive hip flexion, abduction, adduction, and rotation (within pain limits and any hip precautions, especially for arthroplasty).
- Strengthening: Isometric quadriceps and gluteal sets.
-
Weight-Bearing:
-
Intermediate Phase (6-12 weeks):
- Weight-Bearing: Progress to WBAT as radiographic signs of healing appear.
- ROM: Advance ROM exercises.
- Strengthening: Initiate light resistance exercises for hip abductors, adductors, flexors, and extensors.
-
Advanced Phase (12+ weeks):
- Weight-Bearing: Full weight-bearing with normal gait pattern.
- Strengthening: Progress to functional strengthening, balance, proprioception, and sport-specific activities if appropriate.
- Milestones: Independent ambulation without assistive devices, return to prior level of activity.
2. Femoral Shaft Fractures (Intramedullary Nailing)
-
Initial Phase (0-6 weeks):
- Weight-Bearing: Generally WBAT or full weight-bearing immediately for stable IMN (load-sharing construct). Protect for comminuted fractures or specific nail types.
- ROM: Focus on hip and knee ROM exercises (active and passive) to prevent stiffness.
- Strengthening: Isometric quadriceps and gluteal sets, ankle pumps.
-
Intermediate Phase (6-12 weeks):
- Weight-Bearing: Full weight-bearing as tolerated.
- ROM: Continue to improve hip and knee flexibility.
- Strengthening: Progressive resistance exercises for quadriceps, hamstrings, glutes.
-
Advanced Phase (12+ weeks):
- Strengthening: Return to full strength and endurance. Agility and plyometric training as appropriate.
- Milestones: Return to pre-injury activity level.
3. Distal Femur Fractures (Plating, Retrograde Nailing)
-
Initial Phase (0-6 weeks):
- Weight-Bearing: Typically NWB or TDWB. Gradual progression to PWB only with radiographic evidence of healing and stable construct.
- ROM: Gentle active-assisted and passive knee ROM. CPM machine may be used to prevent arthrofibrosis, particularly for intra-articular fractures. Hip ROM as tolerated.
- Strengthening: Isometric quadriceps sets, hamstring sets, ankle pumps.
-
Intermediate Phase (6-12 weeks):
- Weight-Bearing: Progress from PWB to WBAT as radiographic union progresses and pain allows.
- ROM: Aggressively work on achieving functional knee ROM (0-120 degrees flexion).
- Strengthening: Initiate light resistance exercises for quadriceps, hamstrings, and calf muscles.
-
Advanced Phase (12+ weeks):
- Strengthening: Progress to functional exercises, balance, and proprioception.
- Milestones: Achieve full knee and hip ROM. Restore symmetrical gait. Return to recreational or occupational activities.
- Note: Distal femur fractures are often associated with significant knee stiffness; early, controlled ROM is critical.
Throughout rehabilitation, close communication between the surgeon, physical therapist, and patient is essential to adjust the protocol based on individual progress and complications. Radiographic assessment of fracture healing guides progression of weight-bearing.
Summary of Key Literature / Guidelines
The management of femoral pathologies is continuously refined by evidence-based medicine and evolving surgical techniques. Key literature and guidelines from prominent orthopedic organizations provide crucial recommendations.
-
Intramedullary Nailing for Femoral Shaft Fractures:
Considered the gold standard for diaphyseal femur fractures in adults. Multiple studies and meta-analyses consistently demonstrate superior outcomes (union rates, time to union, functional results) compared to plate fixation, particularly for comminuted or segmental patterns.
- Antegrade vs. Retrograde: While antegrade nailing is preferred for most shaft fractures, retrograde nailing offers advantages in specific scenarios like ipsilateral tibia fractures (floating knee), polytrauma patients requiring a less position-intensive approach, or morbidly obese patients where proximal entry is challenging. However, retrograde nailing has a higher risk of knee pain and arthrofibrosis.
-
Proximal Femur Fractures:
- Femoral Neck Fractures: Management varies by patient age and fracture displacement. In younger patients, anatomical reduction and stable internal fixation (cannulated screws or sliding hip screw) is crucial to preserve the femoral head, though AVN remains a significant risk. For displaced fractures in the elderly, arthroplasty (hemiarthroplasty or total hip arthroplasty) often yields better functional outcomes and lower reoperation rates than internal fixation.
- Intertrochanteric Fractures: Intramedullary nails (cephalomedullary nails) have largely supplanted extramedullary devices (e.g., dynamic hip screw, DHS) for unstable intertrochanteric fractures, offering biomechanical advantages, reduced length of hospital stay, and lower implant failure rates. DHS remains a viable option for stable, non-comminuted patterns.
-
Distal Femur Fractures:
- Locked Plating: Modern locked plating systems (e.g., LCPs) applied using minimally invasive percutaneous plate osteosynthesis (MIPPO) techniques have revolutionized distal femur fracture management. They provide stable fixation, preserve soft tissues, and reduce infection rates compared to traditional open techniques.
- Retrograde Nailing: While effective for some supracondylar fractures, particularly extra-articular or simple intra-articular patterns, complex intra-articular fractures often benefit from open reduction and internal fixation with plates to achieve anatomical articular reduction.
- Minimally Invasive Surgery (MIS) & Biological Fixation: The trend towards biological fixation and minimally invasive approaches (e.g., MIPPO, percutaneous techniques for IMN) aims to preserve soft tissue and blood supply, promoting fracture healing and reducing complications like infection and non-union.
- Pre-operative Planning: Evidence strongly supports detailed pre-operative templating and imaging review (including CT for complex fractures) to anticipate challenges and optimize surgical execution.
- Rehabilitation: Early mobilization and progressive weight-bearing, guided by fracture stability and implant choice, are consistently advocated across all femoral fracture types to improve functional outcomes and reduce complications.
Key Organizations and Guidelines:
*
American Academy of Orthopaedic Surgeons (AAOS):
Publishes clinical practice guidelines (CPGs) for various orthopedic conditions, including hip fractures and femoral shaft fractures. These guidelines synthesize evidence to provide recommendations for diagnosis and treatment.
*
Orthopaedic Trauma Association (OTA):
Focuses on advancing musculoskeletal trauma care through education, research, and advocacy. Their publications and courses are central to understanding modern fracture management.
*
AO Foundation (Arbeitsgemeinschaft für Osteosynthesefragen):
A global non-profit organization dedicated to improving patient care in musculoskeletal trauma. Their principles of fracture management (anatomical reduction, stable fixation, preservation of blood supply, early mobilization) are foundational to orthopedic trauma surgery.
The ongoing evolution of implant technology, surgical techniques, and rehabilitation protocols necessitates continuous learning and adherence to evidence-based practices for optimal patient outcomes in managing femoral pathologies.
