Comprehensive Introduction and Patho-Epidemiology
In the realm of operative orthopaedics, the successful management of complex musculoskeletal trauma, aggressive oncologic tumor resections, and severe deep-space infections is inextricably linked to the quality and viability of the overlying soft tissue envelope. A perfectly executed osteosynthesis, a meticulously balanced arthroplasty, or an anatomically reduced articular fracture will ultimately succumb to catastrophic failure if the soft tissue coverage is compromised. The historical paradigm of the "reconstructive ladder" dictates that surgeons should employ the simplest, most reliable method of coverage that fulfills the functional, biomechanical, and aesthetic requirements of the defect. However, modern orthopaedic and plastic surgery principles have evolved toward the "reconstructive elevator," advocating for the immediate selection of the optimal reconstructive modality based on the specific anatomical and physiological needs of the wound bed, rather than strictly progressing from simple to complex.
The patho-epidemiology of orthopaedic soft tissue defects is predominantly driven by high-energy blunt trauma, penetrating injuries, and the subsequent surgical debridement required to achieve a clean wound bed. In the context of open fractures, particularly those classified as Gustilo-Anderson Type IIIB and IIIC, the zone of injury extends far beyond the macroscopic wound margins. High-velocity impacts induce widespread microvascular thrombosis, diffuse tissue contusion, and progressive ischemia in the surrounding skin and musculature. This dynamic pathophysiological cascade means that a wound that appears viable on the day of injury may exhibit extensive necrosis by day three, necessitating serial debridement and delayed, definitive soft tissue reconstruction.
When primary closure is rendered impossible due to excessive tension, profound tissue loss, or severe edema, orthopaedic surgeons must be highly proficient in the application of split-thickness skin grafts (STSGs), free full-thickness skin grafts (FTSGs), and the precise geometric design of local random-pattern flaps. Understanding the complex biomechanics of tissue transfer, the microscopic physiology of graft incorporation, and the precise mathematical principles governing local flaps is mandatory for the practicing orthopaedic consultant. The failure to achieve durable, sensate, and mechanically stable coverage over weight-bearing areas or joints inevitably leads to chronic ulceration, hardware exposure, osteomyelitis, and, in recalcitrant cases, the necessity for major limb amputation.
Furthermore, the demographic shift toward an aging population with multiple medical comorbidities—such as poorly controlled diabetes mellitus, peripheral arterial disease, and chronic venous insufficiency—has exponentially increased the complexity of soft tissue reconstruction. These systemic conditions severely impair the microcirculatory capacity required for graft take and flap survival. Consequently, the orthopaedic surgeon must approach soft tissue reconstruction not merely as a mechanical exercise in wound closure, but as a comprehensive physiological intervention requiring meticulous preoperative optimization, precise intraoperative execution, and rigorous postoperative physiological support.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the microvascular anatomy and biomechanical properties of the integumentary system is the absolute foundation of successful soft tissue reconstruction. The skin is a complex, bi-layered organ consisting of the avascular epidermis and the highly vascularized dermis, supported by the underlying subcutaneous adipose tissue. The epidermis provides a critical barrier against microbial invasion and desiccation, while the dermis—composed of the superficial papillary layer and the deep reticular layer—confers tensile strength, elasticity, and houses the critical adnexal structures (hair follicles, sebaceous glands, and sweat glands). The thickness of these layers varies dramatically across the human body, dictating the selection of donor sites and the anticipated durability of the reconstructed area.
The vascular supply to the skin is organized into a sophisticated, multi-tiered network. Musculocutaneous and septocutaneous perforating arteries traverse the deep fascia to form the deep dermal (subdermal) plexus. This plexus subsequently gives rise to vertical arterioles that supply the superficial papillary plexus. When harvesting a split-thickness skin graft, the surgeon transects these vertical arterioles, relying on the recipient bed to re-establish the vascular connection. In contrast, local random-pattern flaps rely entirely on the horizontal arborization of the subdermal plexus for their survival. The length-to-width ratio of these local flaps is strictly limited by the perfusion pressure within this subdermal network; exceeding the vascular territory of the pedicle invariably leads to ischemic necrosis at the distal tip of the flap.
The physiological survival and incorporation of a free skin graft—a process collectively termed "graft take"—occurs in three distinct, sequential phases. The initial phase, plasmatic imbibition, occurs during the first 24 to 48 hours. During this period, the ischemic graft passively absorbs a transudate of nutrients and oxygen from the recipient bed, causing the graft to become edematous and cyanotic. The second phase, inosculation, begins around 48 to 72 hours post-grafting. This is characterized by the critical alignment and anastomosis of the severed capillary networks of the graft with the proliferating capillary buds of the recipient bed. The final phase, angiogenesis (or neovascularization), involves the active ingrowth of new blood vessels into the graft dermis, establishing a permanent and robust vascular supply by the fifth to seventh postoperative day.
Biomechanically, the skin is an anisotropic and viscoelastic material, meaning its response to mechanical stress is highly dependent on the direction and duration of the applied force. The inherent tension within the skin is organized along Relaxed Skin Tension Lines (RSTLs), commonly referred to as Langer's lines. Surgical incisions and the central limbs of Z-plasties should ideally be oriented parallel to these lines to minimize wound tension and optimize scar maturation. Furthermore, the phenomenon of secondary graft contraction—the tendency of a healed graft to shrink over time due to myofibroblast activity—is inversely proportional to the amount of dermis included in the graft. Therefore, STSGs (which contain less dermis) exhibit significantly more secondary contraction than FTSGs, making the latter biomechanically superior for coverage over highly mobile joints and flexion creases.
Exhaustive Indications and Contraindications
The decision to utilize a split-thickness skin graft, a full-thickness skin graft, or a local flap is dictated by a complex interplay of variables, including the size and depth of the defect, the anatomic location, the quality of the recipient bed, and the physiological status of the patient. STSGs remain the workhorse for large, superficial defects with robust vascular beds, such as those resulting from extensive fasciotomies, massive degloving injuries, or large benign tumor excisions. Because STSGs require less metabolic support, they have a higher probability of primary take in marginal beds compared to FTSGs.
Conversely, FTSGs are specifically indicated for smaller defects in anatomically critical areas where secondary contraction must be minimized, and superior durability, pliability, and aesthetic match are paramount. Common orthopaedic indications include defects on the palmar surface of the hand, the volar aspect of the digits, and the flexion creases of major joints. Local flaps are reserved for scenarios where the recipient bed is entirely devoid of vascularity—such as bare cortical bone denuded of periosteum, exposed tendons lacking paratenon, or exposed orthopaedic implants—or when substantial bulk and padding are required to withstand weight-bearing forces, such as on the plantar aspect of the foot or the ischial tuberosity.
Contraindications to skin grafting are primarily related to the inadequacy of the recipient bed. A skin graft will universally fail if placed over grossly infected tissue, necrotic debris, or heavy eschar. Furthermore, active bleeding or inadequate hemostasis is an absolute contraindication, as the formation of a hematoma physically separates the graft from the vascular bed, preventing plasmatic imbibition and leading to rapid graft necrosis. Systemic contraindications include severe malnutrition, profound immunosuppression, and uncorrected coagulopathies, all of which must be aggressively medically optimized prior to surgical intervention.
| Reconstructive Modality | Primary Orthopaedic Indications | Absolute Contraindications | Recipient Bed Requirements | Biomechanical Characteristics |
|---|---|---|---|---|
| Split-Thickness Skin Graft (STSG) | Large superficial defects, fasciotomy closures, burns, massive degloving injuries. | Bare bone, bare tendon, exposed hardware, active infection, uncontrolled bleeding. | Highly vascularized, clean, granulating bed or healthy muscle/fascia. | High secondary contraction, low durability, poor shear resistance. |
| Full-Thickness Skin Graft (FTSG) | Small defects over joints, palmar/plantar surfaces, fingertip amputations, aesthetic areas. | Large defects, heavily contaminated beds, poor vascularity, hematoma risk. | Pristine, highly vascularized bed, meticulous hemostasis. | Minimal secondary contraction, excellent durability, high pliability. |
| Local Random Pattern Flap | Exposed bone/tendon/hardware, small defects requiring bulk/padding, joint coverage. | Defect larger than flap vascular territory, severe peripheral arterial disease. | Can cover avascular structures; does not rely on recipient bed for initial survival. | Provides native tissue bulk, excellent durability, minimal contraction. |
| Z-Plasty / Tissue Rearrangement | Linear scar contractures crossing joints, web space deepening, realigning tension lines. | Active infection, inadequate lateral skin laxity, severe vascular compromise. | Requires healthy adjacent skin with adequate subdermal vascular plexus. | Lengthens tissue along the central axis, redistributes tension vectors. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of any orthopaedic soft tissue reconstructive procedure is largely determined before the first incision is made. Pre-operative planning begins with a meticulous assessment and optimization of the recipient wound bed. The absolute prerequisite for a successful graft is a highly vascularized bed entirely free of active bleeding, necrotic debris, and gross infection. If the recipient area is unsuitable, the surgeon must commit to a rigorous preparatory phase. This frequently involves the deployment of Negative Pressure Wound Therapy (NPWT), which serves to decrease interstitial edema, remove inhibitory exudates, reduce bacterial bioburden, and rapidly promote the formation of robust granulation tissue.
Donor site selection is a critical component of pre-operative templating. For STSGs, the anterolateral thigh is the preferred donor site due to its broad, flat surface, ease of access, and relatively inconspicuous location. However, in cases of extensive trauma, alternative sites such as the buttocks, back, or scalp may be required. For FTSGs, donor sites are selected based on tissue match and the ability to close the secondary defect primarily. The groin crease, the medial aspect of the arm, and the hypothenar eminence (for palmar defects) are highly favored. The surgeon must carefully template the primary defect using sterile Esmarch bandage material, a foil wrapper from a suture packet, or specialized surgical templating film, ensuring that the exact dimensions are transferred to the donor site to avoid harvesting insufficient or excessive tissue.
Patient positioning must be meticulously planned to allow simultaneous, unhindered access to both the primary defect and the chosen donor site. This often requires the use of specialized orthopaedic tables, radiolucent extensions, or the strategic placement of gel bumps and sandbags. The surgical team must ensure that all pressure points are heavily padded, particularly during prolonged reconstructive cases. Furthermore, the use of a pneumatic tourniquet is highly advantageous during the preparation of the recipient bed and the elevation of local flaps to minimize blood loss and maintain a pristine surgical field. However, the tourniquet must be deflated, and absolute, meticulous hemostasis achieved prior to the application of any skin graft, as hematoma formation is the nemesis of graft survival.
In the context of local flaps and Z-plasties, precise geometric templating on the skin using a sterile surgical marker is mandatory before any local anesthetic with epinephrine is injected, as tissue distortion from the tumescence can severely alter the planned geometry. The surgeon must mathematically calculate the required angles for a Z-plasty—strictly adhering to the 45 to 60-degree rule—to ensure the desired biomechanical yield is achieved without compromising the vascular integrity of the flap tips. The anticipated lines of tension and the vectors of rotation or transposition must be visually confirmed to ensure that the primary defect can be closed without excessive tension that would lead to ischemia or wound dehiscence.
Step-by-Step Surgical Approach and Fixation Technique
Recipient Bed Preparation and Excisional Debridement
The surgical approach begins with the aggressive and systematic preparation of the recipient bed. The surgeon must perform radical sharp debridement, sequentially excising all fibrotic, devitalized, and infected tissue until healthy, punctate bleeding is observed uniformly across the wound bed. This process often requires the use of a scalpel, sharp curettes, or a motorized hydrosurgery system (e.g., Versajet). Grafts will absolutely not survive on bare cortical bone without periosteum, bare tendon without paratenon, or bare articular cartilage, as these tissues lack the capillary network necessary to initiate plasmatic imbibition. Once the bed is optimized, meticulous hemostasis is achieved using bipolar electrocautery, warm saline compresses, and topical hemostatic agents, ensuring no active bleeding remains.
STSG Harvest, Meshing, and Application
For the harvest of a split-thickness skin graft, the donor site is lubricated with sterile mineral oil. A powered dermatome is set to the desired thickness—typically between 0.012 and 0.018 inches (0.3 to 0.45 mm) for orthopaedic applications. The surgeon applies firm, downward pressure and advances the dermatome at a steady, continuous speed, while an assistant applies counter-traction to the skin to maintain a taut, flat surface.
For extensive orthopaedic defects, applying a mesh to the harvested graft is highly advantageous. Meshing serves two critical biomechanical and physiological functions: it allows a smaller donor graft to cover a significantly larger surface area (commonly utilizing expansion ratios of 1:1.5 to 1:3), and it provides fenestrations that allow the free drainage of serum, blood, and exudate from beneath the graft, thereby mitigating the risk of hematoma formation.
The application of the graft requires meticulous tissue handling. The graft is transferred to the recipient area directly from the mesher, ensuring the dermal side faces the wound bed. The graft border must be meticulously attached to the surrounding native skin to secure it in its new position and prevent shear forces. When suturing the graft in place, the trajectory of the needle is critical. It is mechanically much easier—and safer for the graft—to insert a small curved needle first through the graft edge and then through the native skin around the recipient area. Doing the reverse tends to lift the graft off the bed, risking tearing of the fragile split-thickness tissue.
Once the graft is adequately secured at multiple cardinal points using fine non-absorbable sutures (e.g., 4-0 or 5-0 nylon) or surgical skin staples, the redundant edges are carefully trimmed. Overlapping edges will become necrotic and can serve as a nidus for superficial infection.

FTSG Harvest, Defatting, and Salvage Techniques
The harvest of a full-thickness skin graft involves incising the pre-templated elliptical design down to the subcutaneous fat. The graft is elevated using skin hooks, and sharp dissection is used to separate the dermis from the underlying adipose tissue. A critical step in FTSG preparation is the complete and meticulous removal of all residual subcutaneous fat from the dermal undersurface using curved tenotomy scissors. Adipose tissue is poorly vascularized and acts as an impermeable barrier to the diffusion of nutrients from the recipient bed; failure to defat the graft will result in uniform necrosis.
Occasionally, an associated severe orthopaedic injury (e.g., a massive degloving injury or traumatic amputation) makes a detached piece of native skin and underlying fat available. In this salvage scenario, the avulsed skin can be stabilized on a dermatome drum, and a precise full-thickness graft can be excised directly from the underlying traumatized fat, successfully converting discarded tissue into a highly valuable reconstructive graft.
Local Flaps and Z-Plasty Execution
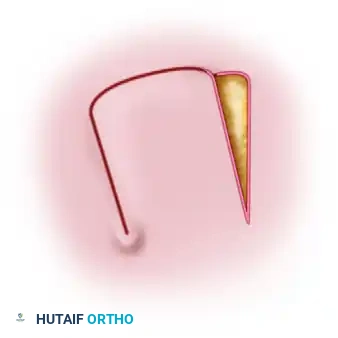
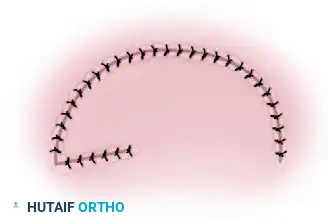
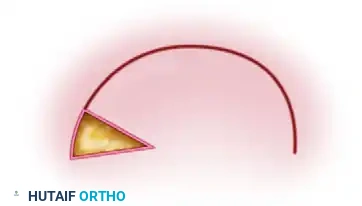
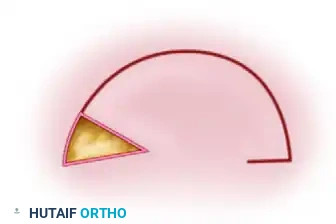
When local flaps are indicated, the primary defect is typically converted into a geometric shape, most commonly a triangle. A rotation flap involves incising a semicircular flap of skin and subcutaneous tissue that is rotated about a pivot point into the adjacent defect. A transposition flap involves lifting and moving a rectangular flap laterally across an intervening bridge of intact skin. In cases where the flap cannot reach the distal extent of the defect, a "back-cut" may be employed at the base of the flap. This significantly decreases the mechanical tension on the flap, allowing greater reach, but simultaneously narrows the pedicle, directly decreasing the blood supply.

For Z-plasty techniques, the central limb is incised along the line of the scar contracture, and two parallel peripheral limbs are created. For optimal results in orthopaedic applications, these angles should be designed strictly between 45 and 60 degrees. A 45-degree angle yields a 50% increase in length with an excellent balance of vascularity, while a 60-degree angle yields a 75% increase in length but requires significant lateral skin laxity. The resulting triangular flaps are deeply elevated, transposed around each other, and meticulously sutured into their new positions using a combination of deep dermal absorbable sutures and superficial non-absorbable sutures to minimize tension on the tips.
Dressing Application and Immobilization
The dressing is as critical as the surgical application itself. The goal is to maintain uniform, gentle pressure to keep the graft intimately apposed to the vascular bed while preventing any shear forces. A finely meshed, nonadherent gauze (e.g., Xeroform or Adaptic) is applied directly over the graft. A stent dressing (tie-over bolus) or a bulky, absorptive dressing is applied over the nonadherent layer and secured with circumferential conforming gauze. If the graft crosses a joint or is in an area subject to movement, the dressing must be covered with a thin layer of plaster or fiberglass for rigid splinting. Shear forces will instantly shear the fragile neovascular network during the inosculation phase, leading to rapid and total graft failure.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and rigorous preoperative optimization, complications following orthopaedic soft tissue reconstruction remain a significant clinical challenge. The most frequent and devastating complication of skin grafting is graft failure, which is most commonly precipitated by hematoma or seroma formation beneath the graft. A hematoma physically isolates the ischemic graft from the underlying capillary bed, preventing the critical initial phase of plasmatic imbibition and leading to rapid full-thickness necrosis. The incidence of hematoma-induced failure can be dramatically reduced through the use of meshed grafts, rigorous intraoperative hemostasis, and the application of compressive tie-over bolus dressings or concurrent NPWT over the graft.
Infection represents another profound threat to both skin grafts and local flaps. Beta-hemolytic Streptococcus and Pseudomonas aeruginosa are particularly notorious for producing proteolytic enzymes that rapidly dissolve the delicate fibrin bonds anchoring the graft to the recipient bed, resulting in catastrophic graft loss. Clinical signs of infection—such as excessive purulent exudate, foul odor, advancing erythema, and systemic toxicity—mandate immediate intervention. Early superficial infections may be managed with targeted systemic antimicrobial therapy and meticulous local wound care, whereas deep or necrotizing infections require emergent return to the operating theater for aggressive surgical debridement and removal of all infected graft material.
Local random-pattern flaps are uniquely susceptible to vascular compromise, which manifests as either arterial insufficiency or venous congestion. Arterial ischemia typically presents as a pale, cool, and pulseless flap tip, often resulting from excessive mechanical tension, an overly narrow pedicle (e.g., an aggressive back-cut), or underlying systemic peripheral arterial disease. Venous congestion, conversely, presents as a swollen, cyanotic, and rapidly blistering flap, caused by inadequate venous outflow despite continuous arterial inflow. Venous congestion is generally more common and equally destructive, as the engorged capillary beds eventually undergo thrombosis, leading to secondary arterial failure and full-thickness necrosis.
Donor site morbidity is an often-underappreciated complication that can cause significant distress to the patient. STSG donor sites are essentially iatrogenic second-degree burns and are frequently more painful than the primary recipient site. Complications include delayed epithelialization, hypertrophic scarring, dyspigmentation, and localized infection. Management involves the use of occlusive, moisture-retentive dressings (e.g., hydrocolloids or transparent films) to promote rapid re-epithelialization and minimize pain.
| Complication | Estimated Incidence | Pathophysiology & Etiology | Salvage Management & Prevention |
|---|---|---|---|
| Hematoma / Seroma | 5% - 15% | Inadequate hemostasis; fluid accumulation physically blocks plasmatic imbibition and inosculation. | Prevention: Meshing, strict hemostasis, tie-over bolus. Salvage: Immediate evacuation via small incision or rolling out fluid; re-securing graft. |
| Graft / Flap Infection | 2% - 10% | Bacterial colonization (e.g., Pseudomonas, Streptococcus) producing proteolytic enzymes that lyse fibrin bonds. | Prevention: Bed optimization, prophylactic antibiotics. Salvage: Systemic IV antibiotics, targeted enzymatic or sharp debridement of necrotic areas, delayed re-grafting. |
| Shear Force Necrosis | 5% - 12% | Mechanical disruption of the fragile neovascular capillary buds during the inosculation phase. | Prevention: Rigid joint immobilization (plaster/fiberglass splinting), absolute bed rest. Salvage: Excision of sheared, necrotic graft; re-preparation of bed and secondary grafting. |
| Flap Venous Congestion | 3% - 8% | Inadequate venous outflow leading to capillary engorgement, thrombosis, and secondary ischemia. | Prevention: Avoid excessive tension or twisting of pedicle. Salvage: Removal of tight sutures, medicinal leeches (Hirudo medicinalis), topical vasodilators. |
| Arterial Ischemia (Flap) | 1% - 5% | Inadequate arterial inflow due to narrow pedicle, excessive back-cut, or systemic vascular disease. | Prevention: Respect length-to-width ratios, avoid narrow angles (<45°). Salvage: Release tension, hyperbaric oxygen therapy (HBOT), conversion to free tissue transfer if viable. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following orthopaedic soft tissue reconstruction must be carefully phased to balance the absolute necessity of graft and flap protection with the orthopaedic imperative to restore joint mobility and prevent profound functional stiffness. The rehabilitation protocol is generally divided into three distinct chronological phases, heavily dependent on the physiological stages of tissue healing and graft incorporation.
Phase 1: Absolute Immobilization and Protection (Days 0 to 7)
During the initial week post-surgery, the graft is undergoing the fragile processes of plasmatic imbibition and early inosculation. Any mechanical shear force during this period will instantly rupture the nascent capillary buds, leading to irreversible graft failure. Therefore, absolute immobilization of the involved extremity is mandatory. If the graft or flap crosses a joint, a rigid plaster or fiberglass splint must be applied in a functional position. The extremity should be continuously elevated above the level of the heart to minimize interstitial edema and venous congestion. The initial surgical dressing is typically left undisturbed for 5 to 7 days unless there are systemic signs of sepsis, intractable pain, or excessive, foul-smelling strike-through exudate.
Phase 2: Gradual Mobilization and Graft Maturation (Weeks 2 to 4)
Upon removal of the initial dressing and clinical confirmation of successful graft take or flap viability (evidenced by a pink, adherent, and blanching tissue bed), the rigid immobilization can be cautiously transitioned to a removable orthosis. Active range of motion (AROM) exercises are initiated under the strict supervision of a specialized physical or occupational therapist. Passive range of motion (PROM) is generally avoided during this early phase, as it can inadvertently generate excessive tension across the newly healed tissue interfaces. The reconstructed area must be aggressively lubricated with non-perfumed, water-based emollients to prevent desiccation and cracking of the fragile new epidermis, which lacks functional sebaceous glands.
Phase 3: Functional Restoration and Scar Management (Weeks 4 and Beyond)
As the reconstructed soft tissue envelope gains tensile strength and the neovascular network matures, the focus of rehabilitation shifts toward full functional restoration and the mitigation of hypertrophic scarring and secondary contracture. Progressive resistance exercises and full weight-bearing protocols are instituted based on the underlying orthopaedic pathology (e.g., fracture consolidation status). Vigorous scar massage, utilizing deep friction techniques, is implemented to break down restrictive subdermal adhesions and realign collagen fibers along the lines of mechanical stress. Furthermore, the application of custom-fitted, gradient compression garments is highly recommended to suppress hypertrophic scar formation, control chronic dependent edema, and support the maturing vascular network of the reconstructed limb.
Summary of Landmark Literature and Clinical Guidelines
The evolution of orthopaedic soft tissue reconstruction is deeply rooted in landmark clinical research and the progressive refinement of surgical guidelines. The foundational principles of managing open fractures and their associated soft tissue defects were codified by Gustilo and Anderson in 1976, and subsequently modified by Gustilo, Mendoza, and Williams in 1984. Their classification system remains the universal standard for predicting the risk of infection and guiding the necessity for complex soft tissue coverage in high-energy trauma.
A paradigm-shifting contribution to the field was made by Marko Godina in 1986, whose seminal retrospective analysis of 532 patients with complex extremity trauma demonstrated that early microsurgical reconstruction (within 72 hours of injury) resulted in dramatically lower rates of flap failure, deep infection, and nonunion compared to delayed reconstruction. While the strict 72-hour window is heavily debated in modern practice—with many major trauma centers advocating for a "fix and flap" approach within 3 to 7 days once the zone of injury has fully demarcated and the patient is physiologically optimized—Godina's work permanently established the critical importance of aggressive, early soft tissue management.
Furthermore, the conceptual shift from the traditional "reconstructive ladder" to the modern "reconstructive elevator," as articulated by Gottlieb and Krieger, has fundamentally altered clinical guidelines. This modern approach dictates that orthopaedic
