Comprehensive Introduction and Patho-Epidemiology
The primary objective of soft tissue reconstruction in the hand is the restoration of durable, sensate coverage that permits unrestricted tendon gliding and joint mobility. The hand is an exquisitely complex biomechanical organ where form and function are inextricably linked; even minor soft tissue deficits can lead to profound functional impairment if not managed with precision. Historically, the reconstructive ladder dictated that surgeons should employ the simplest method that effectively satisfies the functional requirements of the defect. However, modern orthopedic and hand surgery has shifted toward the concept of the "reconstructive elevator," wherein the surgeon immediately selects the optimal reconstructive modality—regardless of its complexity—to maximize functional recovery and minimize morbidity. While secondary intention and primary closure remain appropriate for simple, superficial wounds, complex defects involving the palmar surface, web spaces, or exposed avascular structures (such as bare bone, denuded cartilage, or tendon devoid of paratenon) unequivocally necessitate the use of full-thickness skin grafts (FTSGs) or vascularized flaps.
The patho-epidemiology of hand soft tissue defects is vast, encompassing a wide spectrum of etiologies including industrial crush injuries, thermal and chemical burns, high-energy ballistic trauma, and oncologic resections. Industrial accidents involving saws, presses, and heavy machinery frequently result in composite tissue loss, where skin, subcutaneous fat, nerves, and vascular structures are simultaneously compromised. In these high-energy scenarios, the zone of injury often extends far beyond the macroscopic wound margins, complicating local tissue rearrangement and necessitating careful debridement and delayed reconstruction. Conversely, thermal injuries often present with deep dermal or full-thickness necrosis that, if allowed to heal by secondary intention, results in severe flexion contractures due to the unyielding nature of hypertrophic scarring over the volar flexion creases.
Understanding the physiological requirements of the hand's soft tissue envelope is paramount. The volar skin of the hand is uniquely specialized; it is thick, highly innervated, glabrous, and anchored to the underlying palmar aponeurosis by robust vertical fibrous septa (Cleland’s and Grayson’s ligaments). This anatomical arrangement prevents shearing during prehension and power grip. When this specialized tissue is lost, replacing it with functionally analogous tissue is incredibly challenging. The scarring beneath a simple split-thickness skin graft (STSG) can severely interfere with function in areas where a flexible, mobile bed is required for tendon excursion and joint kinematics. In such instances, FTSGs or skin flaps—which bring their own subcutaneous tissue, inherent vascular supply, and gliding planes—are absolutely mandatory to restore the hand's sophisticated biomechanics.
Furthermore, the epidemiological burden of hand injuries dictates that surgeons must be proficient in a wide array of reconstructive techniques. Hand injuries account for approximately 10% to 20% of all emergency department visits globally, with a significant proportion requiring operative intervention for soft tissue management. The economic impact of these injuries is staggering, primarily due to lost wages and prolonged rehabilitation. Therefore, the timely and appropriate application of FTSGs and local flaps is not merely a matter of aesthetic restoration, but a critical intervention designed to expedite the patient's return to the workforce and restore their quality of life. The mastery of these techniques requires an intimate understanding of vascular anatomy, precise surgical execution, and rigorous postoperative rehabilitation.
Detailed Surgical Anatomy and Biomechanics
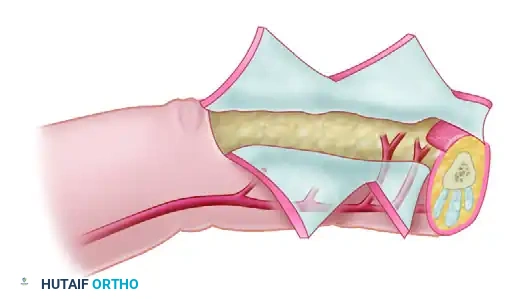
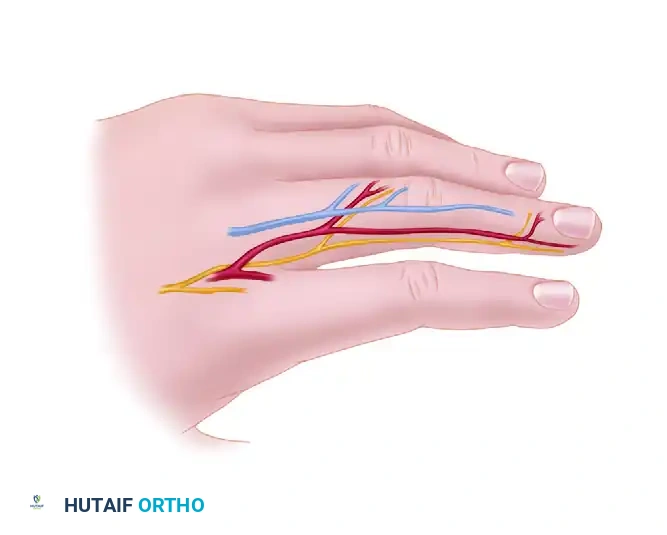
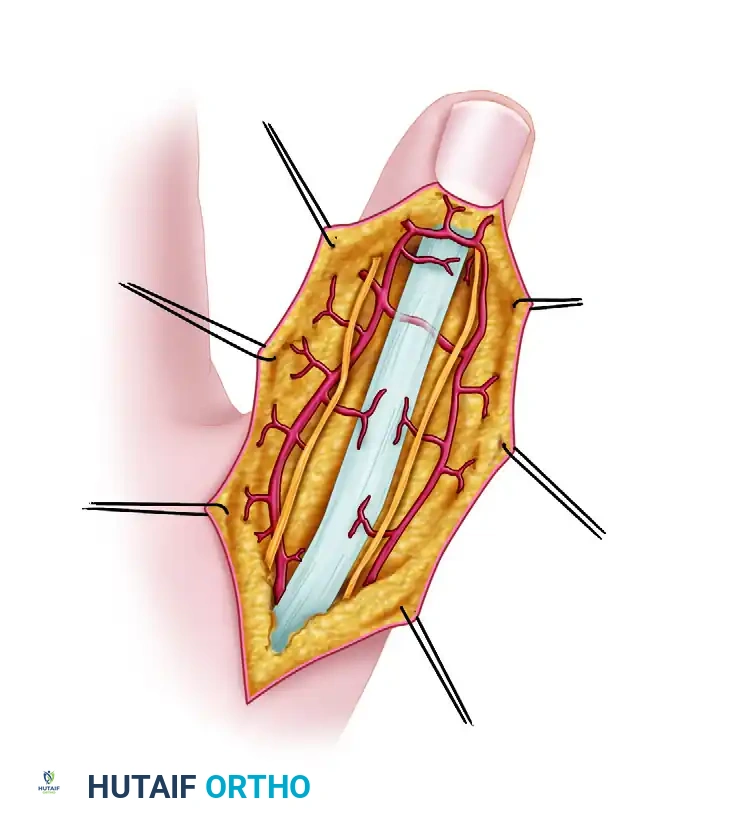
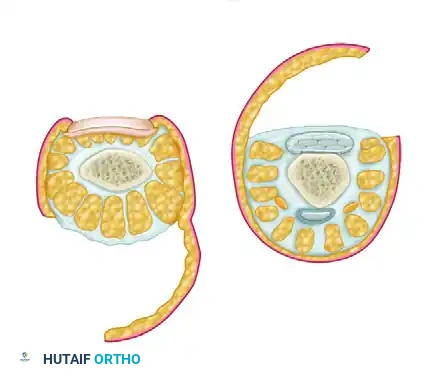
The successful execution of local flaps and full-thickness grafts relies entirely on a profound understanding of the hand's intricate vascular anatomy and the biomechanical properties of its soft tissue envelope. The arterial supply to the hand is derived from the complex anastomotic networks of the superficial and deep palmar arches, which give rise to the common digital arteries and, subsequently, the proper digital arteries. These proper digital arteries travel volar to the transverse metacarpal ligament and give off critical dorsal branches that supply the skin over the proximal and middle phalanges. On the dorsum of the hand, the dorsal metacarpal arteries (DMCAs)—arising from the dorsal carpal arch—travel superficial to the dorsal interosseous fascia. These vessels are the anatomical basis for a multitude of highly reliable regional flaps, including the extended dorsal phalangeal island flap and the reverse DMCA flap.
Equally important to the macroscopic arterial supply is the microscopic architecture of the skin's vascularity, specifically the subdermal plexus. In the context of full-thickness skin grafting, the survival of the graft is entirely dependent on the rapid re-establishment of circulation from the recipient bed. This process occurs in three distinct physiological phases: plasmatic imbibition, inosculation, and angiogenesis. During the first 24 to 48 hours (plasmatic imbibition), the graft survives by absorbing a plasma-like transudate from the recipient bed, which causes the graft to appear edematous and pale. By days 3 to 5 (inosculation), the severed capillary networks of the graft align and connect with those of the recipient bed, restoring true blood flow. Finally, angiogenesis involves the ingrowth of new host vessels into the graft dermis. Any barrier to this process—such as hematoma, seroma, necrotic tissue, or residual adipose tissue on the graft's undersurface—will inevitably result in graft failure.
From a biomechanical perspective, the soft tissue envelope of the hand must accommodate massive ranges of motion without tethering the underlying musculotendinous units. The dorsal skin is exceptionally thin, pliable, and loosely attached to the underlying extensor paratenon via a delicate layer of areolar tissue. This redundancy allows the skin to stretch significantly during full composite flexion of the digits. When reconstructing dorsal defects, the preservation of the extensor paratenon is non-negotiable if a skin graft is to be utilized; without it, the graft will adhere directly to the avascular tendon, completely obliterating the gliding plane and resulting in severe extensor lag. If the paratenon is destroyed, the surgeon is forced to ascend the reconstructive elevator and utilize a flap containing subcutaneous fat (e.g., a reverse adipofascial flap) to recreate this essential gliding interface.
Sensibility is another critical anatomical consideration in hand reconstruction. The volar glabrous skin is densely populated with mechanoreceptors, including Meissner corpuscles (mediating low-frequency vibration and light touch) and Pacinian corpuscles (mediating high-frequency vibration and deep pressure). While full-thickness skin grafts can recover a rudimentary degree of protective sensation through the ingrowth of host nerve fibers (neurotization), they rarely achieve the two-point discrimination required for fine motor tasks. Therefore, for critical contact surfaces—such as the ulnar aspect of the thumb or the radial aspect of the index finger—surgeons must often rely on innervated local flaps, such as the neurovascular island flap. These flaps transfer not only durable skin and subcutaneous padding but also an intact proper digital nerve, maintaining cortical representation and providing immediate, high-quality sensibility to the reconstructed area.
Exhaustive Indications and Contraindications
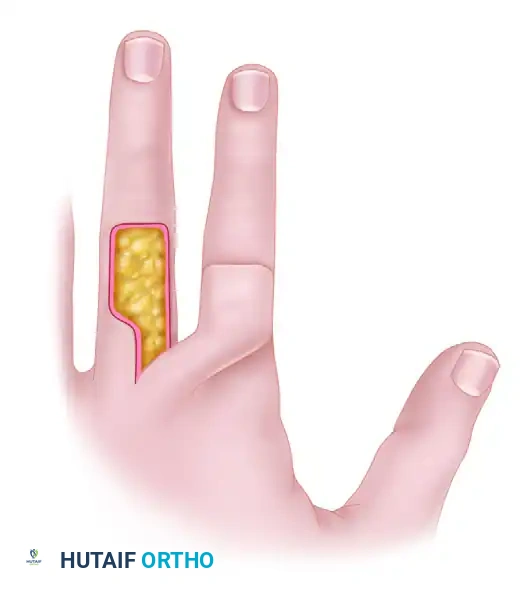
The decision-making process in hand soft tissue reconstruction hinges on a meticulous assessment of the wound bed, the anatomical location of the defect, and the patient's overall physiological status. Full-thickness skin grafts (FTSGs) are highly favored for palmar defects, volar digital wounds, and flexion crease contracture releases (such as in syndactyly reconstruction or Dupuytren's fasciectomy). Because FTSGs contain the entire dermis, they possess a higher concentration of elastin fibers compared to split-thickness grafts. This structural composition translates to minimal secondary contracture, superior durability against shearing forces, and enhanced sensory recovery. FTSGs are indicated whenever a well-vascularized wound bed is present—such as healthy muscle, viable fascia, or intact paratenon/epitenon—and when the defect is not subjected to massive, repetitive friction immediately postoperatively.
Conversely, the absolute contraindications for any skin graft include exposed, avascular structures. Grafts will not "take" on bare cortical bone devoid of periosteum, bare tendon devoid of paratenon, denuded articular cartilage, or exposed neurovascular bundles. In these scenarios, the application of a graft will result in complete necrosis and subsequent exposure of the critical underlying structures, leading to desiccation, infection, and catastrophic functional loss. Additionally, FTSGs are relatively contraindicated in heavily contaminated wounds or wounds with a high risk of ongoing exudation, as the thicker dermis serves as a more substantial barrier to plasmatic imbibition, making them slightly more prone to failure from sub-graft fluid accumulation than STSGs.
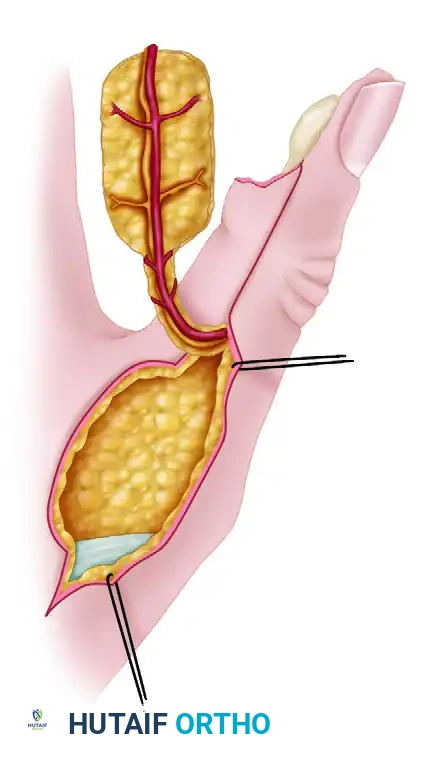
When skin grafts are contraindicated, or when the reconstructive goal requires the restoration of soft tissue bulk and gliding planes, local skin flaps become the standard of care. Flap coverage is utilized in the primary closure of complex hand wounds or in secondary procedures to replace restrictive scars, poor-quality skin, or necrotic tissue. Local flaps provide a robust, vascularized layer of subcutaneous tissue that facilitates a gliding plane for underlying tendons and joints. Indications for local flaps include fingertip amputations with exposed distal phalangeal bone (e.g., V-Y advancement flaps, cross-finger flaps), deep dorsal defects over the interphalangeal joints (e.g., reverse adipofascial flaps), and massive palmar defects requiring durable, padded coverage.
Contraindications for local flaps primarily revolve around the vascular integrity of the donor site and the zone of injury. A local flap must never be designed within a zone of severe crush injury or radiation damage, as the microvascular compromise in these areas will inevitably lead to flap necrosis. Furthermore, patients with severe peripheral vascular disease, uncontrolled diabetes mellitus with microangiopathy, or active tobacco abuse represent high-risk candidates for local flap failure. In such cases, the surgeon must carefully weigh the risks of local tissue transfer against the potential benefits, often opting for more robust distant pedicled flaps or free tissue transfers that bring a completely independent, healthy blood supply to the compromised extremity.
| Modality | Primary Indications | Absolute Contraindications | Advantages | Disadvantages |
|---|---|---|---|---|
| Full-Thickness Skin Graft (FTSG) | Volar digital defects, syndactyly release, palmar wounds with vascular bed (paratenon/muscle). | Bare bone, bare tendon, exposed cartilage, heavily infected/exudative wounds. | Minimal secondary contracture, good durability, better sensory recovery than STSG. | Requires optimal vascular bed, higher risk of non-take than STSG, donor site morbidity. |
| Local Advancement Flaps (e.g., V-Y) | Fingertip amputations with exposed distal phalanx, small volar defects. | Extensive tissue loss precluding tension-free advancement, crushed donor tissue. | Replaces "like with like," maintains normal sensation, simple execution. | Limited advancement distance, risk of tip necrosis if advanced under tension. |
| Regional Flaps (e.g., Cross-Finger) | Volar defects with exposed tendon/bone, failed local flaps. | Injuries to adjacent donor digit, advanced patient age (stiffness risk), rheumatoid arthritis. | Excellent vascularity, provides robust padding and gliding surface. | Requires 2-stage procedure, temporary tethering of digits, risk of joint stiffness. |
| Neurovascular Island Flap | Sensate coverage for critical pinch areas (thumb ulnar aspect, index radial aspect). | Damage to the proper digital artery/nerve of the donor digit, severe vascular disease. | Provides immediate, high-quality sensation and durable glabrous skin. | Technically demanding, risk of cortical misinterpretation, sacrifices sensation in donor digit. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful soft tissue reconstruction in the hand. The process begins with a comprehensive physical examination to accurately define the true zone of injury, which frequently extends beyond the visible wound margins. The surgeon must assess the viability of the surrounding skin, the integrity of the underlying musculotendinous and neurovascular structures, and the presence of any concurrent skeletal instability that may require rigid fixation prior to soft tissue coverage. For complex regional flaps, such as those based on the dorsal metacarpal arteries (DMCA), pre-operative mapping of the perforating vessels using a handheld Doppler ultrasound (8-10 MHz) is highly recommended to confirm the presence and location of the vascular pedicle.
Donor site selection for full-thickness skin grafts is a critical decision that impacts both the aesthetic and functional outcomes of the reconstruction. The ideal donor site provides skin that closely matches the recipient area in terms of thickness, texture, and pigmentation, while allowing for primary closure with minimal morbidity. For small to moderate palmar defects, the hypothenar eminence and the volar wrist crease are excellent donor sites, as they provide glabrous or semi-glabrous skin with an exceptional color match. For larger defects, the medial arm or the groin (specifically the lower abdominal crease) are preferred, as these areas provide an abundance of pliable skin and the resulting scars can be easily concealed beneath clothing. However, groin skin tends to hyperpigment over time and may transfer unwanted hair follicles if not carefully selected.
The process of templating is essential to ensure precise graft or flap dimensions. Once the recipient bed has been thoroughly debrided to healthy, bleeding tissue, a template of the defect is created using a sterile foil wrapper, an Esmarch bandage, or clear sterile tape. This template is then transferred to the selected donor site. A critical surgical pearl in FTSG harvesting is to mark the anticipated graft outline approximately 10% to 15% larger than the template. This deliberate oversizing accommodates the primary shrinkage of the graft—a phenomenon caused by the immediate contraction of dermal elastin fibers upon excision—and provides the necessary margin for tension-free suturing during insetting. For local flaps, the template is used to plan the pivot point and the arc of rotation, ensuring that the pedicle length is sufficient to reach the distal extent of the defect without tension.
Patient positioning and operating room setup must be optimized to facilitate precise microsurgical techniques. The patient is typically positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm to provide a bloodless surgical field, which is absolutely critical for identifying delicate neurovascular structures and ensuring complete hemostasis prior to graft or flap insetting. The surgeon and assistant should be seated comfortably, utilizing loupe magnification (typically 2.5x to 4.5x) and specialized micro-instruments. Proper lighting, ergonomic positioning, and a meticulously organized sterile field are fundamental prerequisites for executing the intricate dissections required in advanced hand reconstruction.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of soft tissue coverage requires absolute adherence to the principles of atraumatic tissue handling, precise plane dissection, and tension-free fixation. Prior to any reconstructive effort, the wound must undergo aggressive surgical debridement. All non-viable tissue, foreign debris, and marginal skin edges must be excised until punctate bleeding is observed from the dermis and underlying tissues. Once the recipient bed is optimized, the surgeon proceeds with the selected reconstructive modality.
Full-Thickness Skin Graft Harvesting and Insetting
Harvesting an FTSG requires precision to ensure the inclusion of the entire dermis while minimizing the harvest of subcutaneous fat. Following templating and marking, the skin is incised sharply along the markings using a #15 scalpel blade. The surgeon applies skin hooks to the edge of the graft, providing upward traction to define the plane between the deep reticular dermis and the underlying subcutaneous adipose tissue. The graft is carefully dissected free.
Defatting the graft is arguably the most critical step in this procedure. Fat acts as an impermeable barrier to plasmatic imbibition and inosculation; any residual adipose tissue will cause localized graft necrosis. The graft is inverted over the surgeon’s non-dominant index finger, and curved tenotomy or Iris scissors are used to meticulously trim away all yellow fat until the white, glistening surface of the deep dermis is uniformly exposed.

For fixation and insetting, the FTSG is transferred to the recipient bed and secured using simple interrupted or running non-absorbable monofilament sutures (e.g., 5-0 or 6-0 nylon). The graft must lie perfectly flat; redundant edges should be trimmed to prevent wrinkling, which can lead to focal necrosis. To ensure intimate contact between the graft and the bed, and to prevent shearing forces, a tie-over bolster (stent dressing) is mandatory. Long suture tails are left at intervals around the graft, a non-adherent interface layer (e.g., Xeroform or Adaptic) is applied, and a bolus of saline-soaked cotton, fluffed gauze, or a specialized surgical sponge is placed over the graft. The long suture tails are then tied tightly over the bolster, compressing the graft into the bed and obliterating any dead space where hematomas could form.
Fundamental Local Flap Techniques: Z-Plasty and Transposition
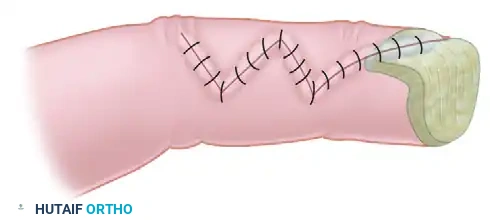
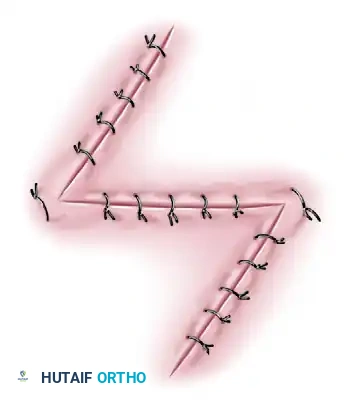
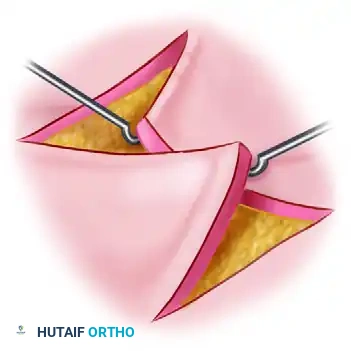
The Z-plasty is a workhorse transposition flap technique utilized to lengthen linear contractures, redirect scars, or deepen web spaces. The classic Z-plasty consists of a central limb (the contracture line) and two lateral limbs of equal length, oriented at 60-degree angles to the central limb. This 60-degree configuration theoretically provides a 73% increase in length along the central axis. The flaps are elevated in the subcutaneous plane, preserving the subdermal plexus, and then transposed.

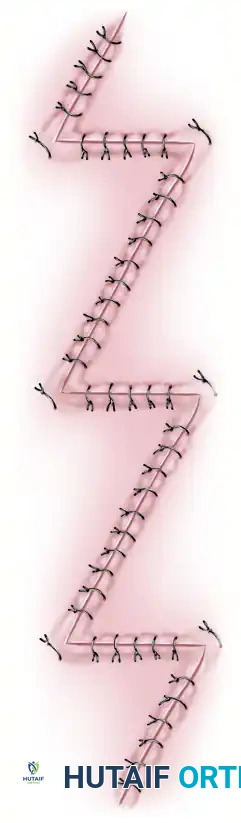
For long, narrow contractures crossing multiple flexion creases (such as severe burn syndactyly), a single massive Z-plasty is often insufficient and may result in tip necrosis. In these cases, multiple continuous Z-plasties (e.g., four-flap or five-flap Z-plasties) are designed to distribute tension and maximize lengthening.
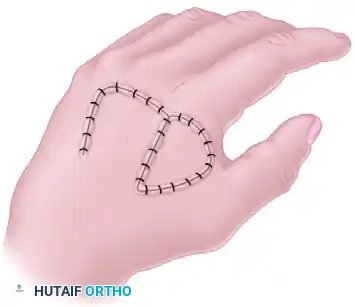
Translation and transposition flaps involve moving tissue laterally across an adjacent area of intact skin to close a defect. A critical pitfall in designing a transposition flap is underestimating the required length. The fixed point of pivot is at the border of the base opposite the defect; if the flap is too short, the line of maximum tension will restrict vascular inflow, leading to distal tip ischemia. The donor site of a transposition flap invariably requires closure with a skin graft.



Advanced Digital Coverage: Dorsal Metacarpal Artery and Reverse Adipofascial Flaps
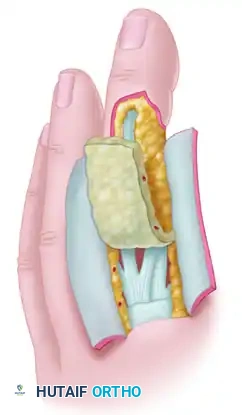
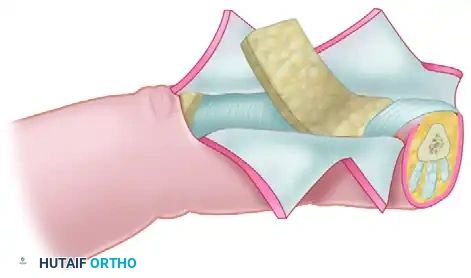
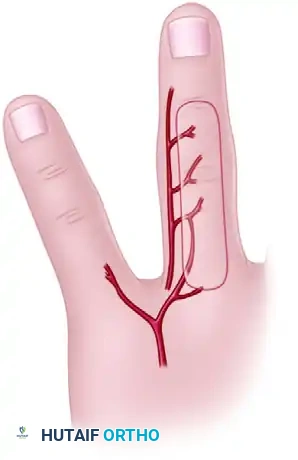
For complex dorsal defects or palmar wounds requiring vascularized bulk, Dorsal Metacarpal Artery (DMCA) flaps provide robust coverage. These flaps are based on the anastomoses between the palmar digital artery and the DMCA. The flap is raised in the subfascial plane, including the deep fascia over the interosseous muscles to protect the delicate vascular pedicle.

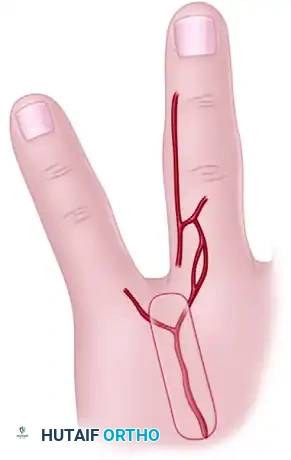




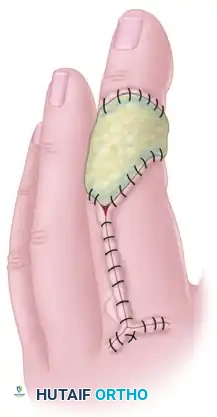
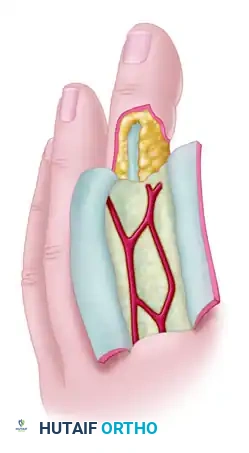
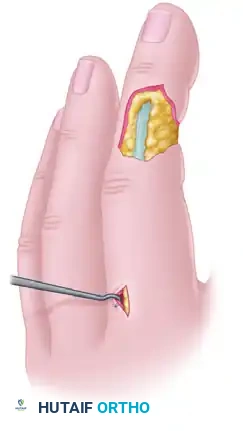
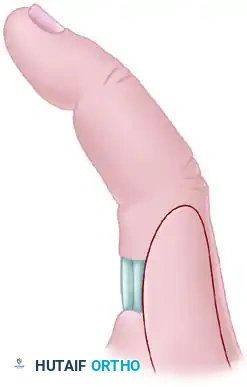
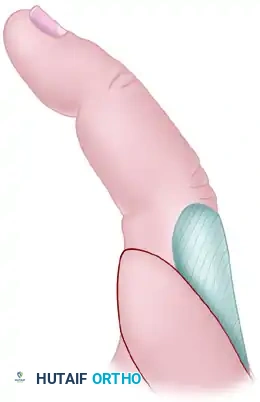
When dorsal defects involve exposed distal interphalangeal (DIP) joints or amputations at the nail fold, a reverse adipofascial flap is an elegant solution. This proximally based "turnover flap" relies on the dorsal branches of the digital arteries. The skin is incised via an H
Clinical & Radiographic Imaging Archive