Comprehensive Introduction and Patho-Epidemiology
The reconstruction of soft tissue defects in the hand and upper extremity represents one of the most formidable challenges in operative orthopaedics and plastic surgery. The fundamental objective transcends mere wound closure; it demands the meticulous restoration of form, durable coverage, sensate interaction with the environment, and the preservation of intricate biomechanical glide planes. When primary closure is impossible and skin grafting is contraindicated—typically due to the exposure of avascular structures such as denuded bone, joints, cartilage, or tendons devoid of their nourishing paratenon—the reconstructive surgeon must ascend the reconstructive elevator. In this context, pedicled and regional flap coverage becomes not merely an option, but an absolute mandate to salvage the limb and restore function.
The patho-epidemiology of hand defects is broad, encompassing high-energy industrial crush injuries, thermal and chemical burns, severe avulsions, and post-oncologic extirpative defects. Industrial machinery accidents frequently result in volar digital tissue loss, exposing the flexor tendon sheath and neurovascular bundles. In such localized scenarios, the Cross Finger Flap (CFF) has stood for decades as a highly reliable, workhorse technique. Originally popularized in the mid-20th century, the CFF provides robust, matched, glabrous-like tissue capable of withstanding the sheer forces of daily prehension. Its enduring relevance in modern hand surgery is a testament to its reliability, straightforward geometry, and excellent functional outcomes when executed with precision.
Conversely, high-velocity trauma, blast injuries, or extensive tumor resections often yield massive, complex composite defects of the hand and wrist that far exceed the reconstructive capacity of local digital flaps. For these extensive wounds, regional fascial or fasciocutaneous flaps are required. The Radial Forearm Flap (RFF), colloquially known as the "Chinese Flap" due to its pioneering development at the Shenyang Military Hospital in 1981, revolutionized upper extremity reconstruction. As a pedicled, reverse-flow flap, it offers a massive territory of pliable, well-vascularized tissue that can reach the distal digits, dorsum of the hand, and first web space without the need for microvascular anastomosis.
Both the Cross Finger Flap and the Radial Forearm Flap demand an encyclopedic understanding of upper extremity vascular anatomy, precise atraumatic tissue handling, and rigorous adherence to structured postoperative rehabilitation protocols. The surgeon must balance the imperative of recipient site coverage against the inevitable cost of donor site morbidity. This chapter provides an exhaustive, step-by-step technical exposition of these two indispensable reconstructive techniques, designed to equip the advanced orthopedic and hand surgeon with the critical nuances required for flawless execution and optimal patient outcomes.
Detailed Surgical Anatomy and Biomechanics
The successful execution of a Cross Finger Flap relies on a profound understanding of the microvascular anatomy of the digits. The flap is traditionally designed as a random-pattern flap, though it is anatomically supported by a rich subdermal plexus fed by the dorsal branches of the proper digital arteries. These dorsal branches arborize extensively over the middle and proximal phalanges. The skin of the dorsum of the finger is highly mobile and pliable, making it an ideal donor tissue. Crucially, the dissection plane must remain strictly superficial to the extensor peritenon. The peritenon is a thin, highly vascularized areolar tissue layer overlying the extensor mechanism; its preservation is non-negotiable, as it provides the sole vascular bed for the subsequent split-thickness skin graft (STSG) or full-thickness skin graft (FTSG) applied to the donor site.
Biomechanically, the Cross Finger Flap requires the temporary syndactylization of two adjacent digits. This creates a non-physiologic tethering that alters the kinematic chain of the hand. The surgeon must be acutely aware of the ligamentous anatomy, specifically Cleland’s and Grayson’s ligaments. Cleland’s ligaments are robust, dorsally situated fascial bands that stabilize the digital skin during flexion and extension, whereas Grayson’s ligaments are volar and more delicate. During the mobilization of the CFF base, selective release of Cleland’s ligaments is often required to achieve adequate rotation and reach without placing tension on the subdermal vascular plexus. Failure to understand this tethering effect will result in either inadequate flap reach or catastrophic vascular compromise due to excessive tension.
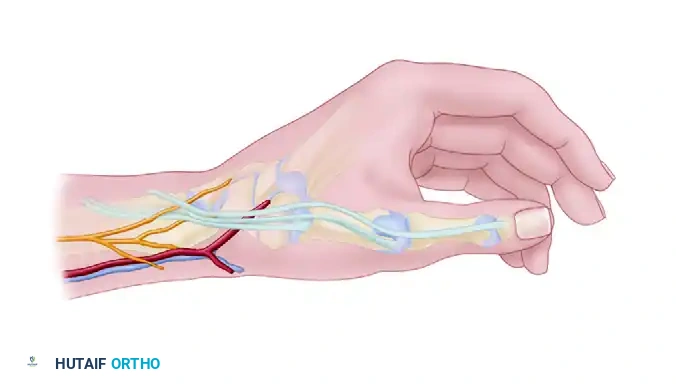
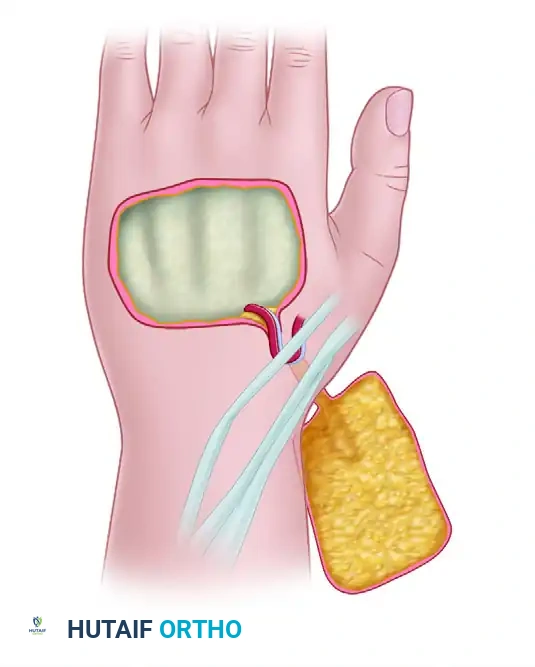
The Radial Forearm Flap is predicated on the constant and robust anatomy of the radial artery and its associated venae comitantes. The radial artery courses distally in the forearm between the brachioradialis and the flexor carpi radialis (FCR) muscles, giving off a dense, continuous septocutaneous perforator system that supplies the overlying fascia and skin. This vascular territory spans from the antecubital fossa to the radial styloid, encompassing an area up to 16 cm by 8 cm. The primary perforators are concentrated in the distal half of the forearm, particularly around 7 cm proximal to the radial styloid. When harvested as a reverse-flow pedicled flap, the biomechanics of perfusion are entirely altered. Arterial inflow is driven retrogradely from the ulnar artery via the deep and superficial palmar arches into the distal radial artery stump.
Venous drainage in the reverse Radial Forearm Flap is a complex hemodynamic phenomenon. Because the flap relies on retrograde flow, the venous blood must overcome the proximally directed venous valves within the venae comitantes. This is achieved through two primary mechanisms: the inherent arterial pressure driving blood through collateral crossover channels (communicating branches) that bypass the valves, and the eventual incompetence of these delicate valves under sustained reverse pressure. Additionally, the superficial sensory innervation of the flap is supplied by the lateral antebrachial cutaneous nerve and the medial antebrachial cutaneous nerve. The surgeon must meticulously navigate around the superficial branch of the radial nerve, which emerges from beneath the brachioradialis in the distal third of the forearm, ensuring it is neither transected nor compressed during fascial closure or grafting, which would result in debilitating neuromas or paresthesias.
Exhaustive Indications and Contraindications
The decision to utilize a Cross Finger Flap versus a Radial Forearm Flap—or to pursue alternative reconstructive options such as homodigital island flaps, thenar flaps, or free tissue transfer—requires a sophisticated algorithmic approach. The surgeon must evaluate the size, depth, and location of the defect, the status of the surrounding vascular axes, the patient's physiological age, and their capacity to comply with demanding postoperative rehabilitation. Flap selection is never a generic prescription; it is a highly individualized tactical decision.
The Cross Finger Flap is the definitive indication for volar soft tissue defects of the middle and proximal phalanges where exposed flexor tendon (devoid of paratenon), exposed bone, or exposed neurovascular bundles preclude the use of skin grafts. It is particularly valuable when local advancement flaps, such as the Atasoy V-Y advancement or Moberg volar advancement, cannot provide sufficient distal reach or would result in unacceptable flexion contractures. The CFF provides durable coverage that, while initially insensate, reliably regains protective sensation through peripheral nerve ingrowth over 6 to 12 months. However, it is absolutely contraindicated in the presence of severe crush injuries that compromise the microvasculature of the proposed donor digit.
The reverse Radial Forearm Flap is indicated for massive, composite defects of the hand and wrist that require immediate, robust vascularized coverage. Classic indications include extensive dorsal hand avulsions, severe first web space contractures requiring release and resurfacing, and complex volar wrist defects exposing the median nerve and flexor tendons. Its ability to incorporate vascularized bone (a segment of the distal radius) or vascularized tendon (palmaris longus or brachioradialis) makes it a versatile osteofasciocutaneous or tendofasciocutaneous option. The absolute contraindication for a reverse RFF is an incomplete superficial or deep palmar arch, which renders the hand entirely dependent on the radial artery for perfusion. Harvesting the radial artery in such patients will precipitate catastrophic ischemic necrosis of the hand.
| Feature / Parameter | Cross Finger Flap (CFF) | Reverse Radial Forearm Flap (RFF) |
|---|---|---|
| Primary Indication | Volar defects of proximal/middle phalanges with exposed bone/tendon. | Large composite defects of the hand, wrist, or first web space. |
| Tissue Type | Random-pattern (or axially based dorsal branch) fasciocutaneous. | Septocutaneous / Fasciocutaneous (can be osteocutaneous). |
| Vascular Supply | Dorsal digital arterial plexus. | Retrograde flow via deep palmar arch to radial artery. |
| Absolute Contraindications | Crush injury to donor digit; severe pre-existing joint stiffness/OA. | Incomplete palmar arch; abnormal Allen test; active arterial disease. |
| Relative Contraindications | Rheumatoid arthritis; non-compliant patient (requires 2-stage division). | Severe venous insufficiency; prior radial arterial line placement. |
| Donor Site Morbidity | STSG/FTSG on donor finger dorsum; risk of PIP joint stiffness. | Significant aesthetic deformity; risk of FCR paratenon loss; radial nerve injury. |
Special considerations must be given to patients with systemic microvascular disease. Chronic tobacco use, poorly controlled diabetes mellitus, and severe vasospastic disorders (such as Raynaud's phenomenon) significantly increase the risk of flap necrosis, particularly in the random-pattern distal margins of the CFF and the venous outflow of the reverse RFF. In such populations, a mandatory smoking cessation period of at least 4 weeks preoperatively and postoperatively is strongly advised, and alternative reconstructive strategies, such as secondary intention healing or negative pressure wound therapy (if no vital structures are exposed), should be exhaustively considered.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful flap surgery; errors made in the design phase cannot be easily salvaged in the operating theater. For the Cross Finger Flap, planning begins with a thorough debridement of the recipient site. The defect must be converted into a precise geometric shape, typically a rectangle, with its longitudinal borders running parallel to the long axis of the finger. This prevents the formation of oblique scars that cross the volar flexion creases, which inevitably lead to severe flexion contractures. A template of the defect is created using the sterile foil from a suture packet or a piece of Esmarch bandage. This template is then transposed onto the dorsum of the adjacent donor finger. The surgeon must design the flap to be 4 to 6 mm wider and longer than the actual defect to account for the primary contraction of the skin once elevated, and to ensure a tension-free pedicle bridge.
For the reverse Radial Forearm Flap, preoperative vascular assessment is an absolute, non-negotiable mandate. A clinical Allen test must be performed to confirm dual arterial supply to the hand. If the clinical Allen test is equivocal, objective confirmation via Doppler ultrasound mapping or formal digital subtraction angiography is required. The surgeon must map the course of the radial artery and identify the major perforators using a handheld Doppler. Templating for the RFF involves measuring the exact dimensions of the recipient defect and transferring this pattern to the volar forearm. The pivot point of the pedicle—usually located just proximal to the anatomical snuffbox—must be precisely marked. The distance from the pivot point to the distal edge of the defect represents the required pedicle length, which dictates the proximal extent of the flap design on the forearm.
Patient positioning is critical for optimal surgical ergonomics and access. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. For the Cross Finger Flap, the hand is secured in a pronated or supinated position depending on the phase of the operation, often utilizing a lead hand splint for stabilization. For the RFF, the entire arm from the axilla to the fingertips must be meticulously prepped and draped to allow for full visualization of the forearm and hand. The donor site for the necessary skin graft (typically the ipsilateral proximal forearm, medial arm, or anterior thigh) must also be prepped and draped in the sterile field.
Anesthetic considerations play a vital role in flap survival. While general anesthesia is frequently employed, regional anesthesia (such as an axillary or supraclavicular brachial plexus block) offers distinct advantages. Regional blocks induce a profound sympathectomy, resulting in maximal vasodilation and optimized peripheral perfusion, which is highly beneficial for both the CFF and the RFF. The anesthesia team must be explicitly instructed to avoid the use of systemic vasoconstrictors and to maintain normothermia and normovolemia throughout the procedure, as peripheral hypoperfusion can easily precipitate venous congestion or arterial thrombosis in the delicate microvasculature of the flaps.
Step-by-Step Surgical Approach and Fixation Technique
Cross Finger Flap Technique
1. Defect Preparation and Flap Design:
The operation commences with radical debridement of the recipient defect under tourniquet control. All non-viable tissue is excised until healthy, bleeding margins are obtained. The defect is squared off. The template is placed on the dorsum of the adjacent donor finger, ensuring the base of the flap hinges precisely at the midlateral line adjacent to the recipient digit.
2. Flap Elevation:
Incision begins on the dorsal aspect of the donor finger. The flap is elevated from distal to proximal (or dorsal to lateral) utilizing meticulous sharp dissection.
The cleavage plane is strictly within the loose areolar tissue of the subcutaneous fat. It is an absolute imperative to leave the glistening, white paratenon overlying the extensor mechanism completely intact.
Violation of this layer will result in failure of the subsequent skin graft, leading to desiccation and rupture of the extensor tendon.
3. Mobilization of the Base:
To ensure a tension-free span across the interdigital web, the base of the flap must be mobilized. This requires the careful identification and sharp division of Cleland’s ligaments—the oblique fascial bands tethering the skin to the periosteum.
During this release, the surgeon must maintain direct visualization of the volar digital artery and nerve, which lie immediately volar to the midlateral line, ensuring they are not injured.
4. Hemostasis and Grafting:
The tourniquet is deflated to confirm robust perfusion of the flap and to achieve meticulous hemostasis of the donor bed using bipolar electrocautery. A full-thickness or thick split-thickness skin graft is harvested and sutured into the donor defect. The graft must also cover the undersurface of the bridging pedicle to prevent raw surface adherence and subsequent contracture.
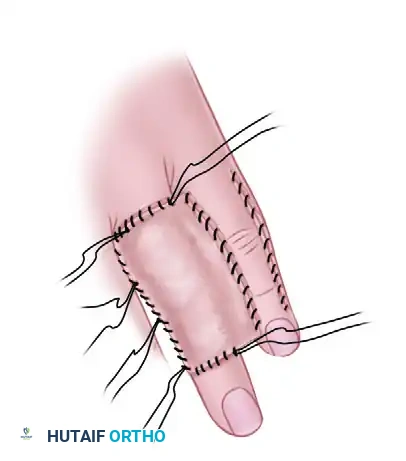
5. Flap Inset and Fixation:
The flap is transposed over the recipient defect and inset using interrupted 5-0 or 6-0 non-absorbable sutures. Tension must be strictly avoided. A tie-over stent dressing is applied over the donor site graft to ensure intimate contact with the paratenon bed.

To protect the delicate pedicle, the two fingers are immobilized, often utilizing a transarticular oblique K-wire through the recipient PIP joint or pinning the adjacent phalanges together, followed by the application of a volar resting splint.
Reverse Radial Forearm Flap Technique
1. Flap Design and Proximal Dissection:
The flap territory is mapped on the volar forearm.
The proximal incision is made first to identify the radial artery and its venae comitantes. The vessels are carefully isolated, ligated, and divided at the proximal margin of the flap.
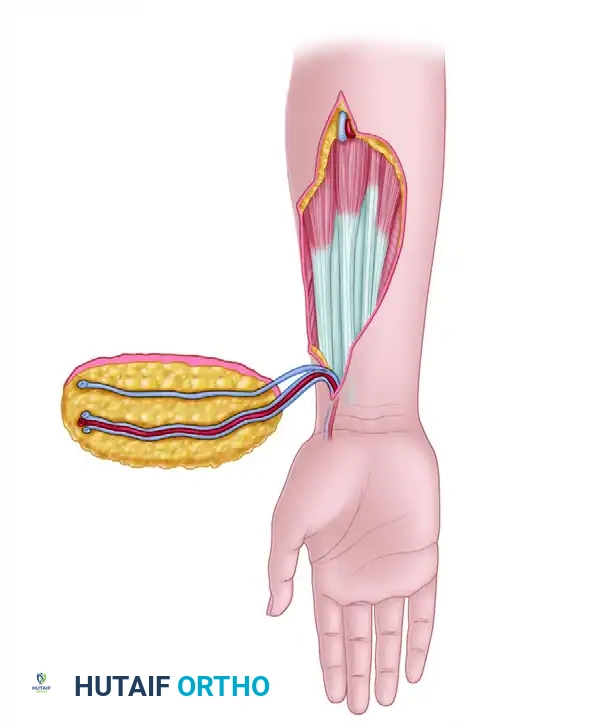
2. Fascial Elevation and Perforator Preservation:
The flap is elevated in a subfascial plane, proceeding from proximal to distal and ulnar to radial. The deep fascia is incised, and the flap is lifted off the underlying flexor muscles.
Extreme care is taken to preserve the intermuscular septum between the brachioradialis and the FCR, as this septum contains the critical fasciocutaneous perforators supplying the flap. The superficial branch of the radial nerve is identified and rigorously protected.
3. Pedicle Skeletonization and Reverse Flow Verification:
The pedicle is dissected distally toward the pivot point. The brachioradialis tendon is mobilized radially to expose the distal radial artery. Once the island flap is completely isolated on its distal pedicle, the tourniquet is deflated.
The surgeon observes the flap for robust arterial inflow and adequate venous outflow. If venous congestion is noted, an additional superficial vein (e.g., cephalic vein) may be preserved and tunneled for a supercharged microvascular anastomosis at the recipient site.
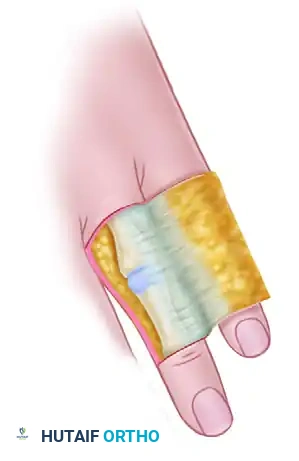
4. Flap Inset and Donor Site Management:
The flap is rotated 180 degrees to reach the hand defect.
It is passed either through a wide subcutaneous tunnel or via an open incision to prevent pedicle compression. The flap is inset with minimal tension. The donor site is meticulously managed; the paratenon over the FCR and brachioradialis must be preserved to accept a split-thickness skin graft. A negative pressure wound therapy (NPWT) dressing or a robust tie-over bolster is applied to the donor site to ensure graft take.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, both the Cross Finger Flap and the Radial Forearm Flap carry inherent risks of complications. Flap failure is broadly categorized into arterial insufficiency and venous congestion. Arterial insufficiency typically presents intraoperatively or within the first 24 hours as a pale, cool flap with absent capillary refill. It is most often caused by excessive tension on the pedicle, a tight subcutaneous tunnel, or unrecognized arterial thrombosis. Venous congestion, conversely, presents as a swollen, violaceous, or blue flap with brisk, dark capillary refill. It is the most common cause of failure in reverse-flow flaps like the RFF, resulting from inadequate venous bypass of the competent valves within the venae comitantes.
For the Cross Finger Flap, the most significant complications involve the donor digit. Loss of the skin graft over the donor site occurs in approximately 5-10% of cases, almost exclusively due to iatrogenic violation of the extensor peritenon or inadequate bolster pressure leading to hematoma formation. If the graft fails and the extensor tendon desiccates, the patient faces severe functional impairment. Salvage requires aggressive debridement and potentially a secondary local flap or reverse homodigital flap to cover the exposed tendon. Furthermore, prolonged immobilization can lead to severe Proximal Interphalangeal (PIP) joint flexion contractures in both the donor and recipient fingers, highlighting the critical need for timely flap division and aggressive hand therapy.
The reverse Radial Forearm Flap carries a distinct set of morbidities. Venous congestion occurs in up to 15% of cases. Immediate salvage interventions include releasing any constricting sutures, ensuring the wrist is not excessively flexed or extended, and applying medical grade leeches (Hirudo medicinalis) to provide temporary venous outflow while neovascularization occurs. Donor site morbidity is a major criticism of the RFF; aesthetic deformity is universal, and functional deficits such as reduced grip strength, delayed healing of the skin graft, or partial loss of the FCR tendon occur in 10-20% of patients. Neuropraxia of the superficial radial nerve is also a recognized complication, requiring meticulous protection during dissection.
Complications and Salvage Management Matrix
| Complication | Flap Type | Estimated Incidence | Clinical Presentation | Salvage / Management Strategy |
|---|---|---|---|---|
| Venous Congestion | RFF (Reverse) | 10 - 15% | Violaceous color, rapid dark capillary refill, swelling. | Release tight sutures; optimize wrist position; apply Hirudo medicinalis (leeches); systemic heparin. |
| Arterial Insufficiency | CFF / RFF | 2 - 5% | Pallor, cool to touch, absent capillary refill. | Remove constrictive dressings; explore pedicle for kinking/hematoma; consider revision of tunnel. |
| Donor Graft Failure | CFF | 5 - 10% | Necrotic STSG/FTSG, exposed extensor tendon. | Debridement; if paratenon lost, requires secondary flap coverage (e.g., reverse metacarpal flap). |
| PIP Joint Contracture | CFF | 15 - 25% | Inability to fully extend PIP joint post-division. | Aggressive dynamic splinting; intensive hand therapy; rarely surgical capsulotomy. |
| Radial Nerve Injury | RFF | 3 - 8% | Paresthesia/numbness in dorsal radial hand; Tinel's sign. | Observation for neuropraxia; gabapentinoids; surgical exploration if neuroma suspected. |
| FCR Tendon Exposure | RFF | 5 - 12% | Graft loss over FCR tendon at donor site. | Local wound care; NPWT; secondary grafting once granulation tissue forms. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is as critical to the final functional outcome as the surgical execution itself. A poorly managed postoperative phase can ruin a perfectly executed flap through pedicle avulsion, joint contracture, or graft shear. The protocol is inherently phased, balancing the competing demands of flap vascular protection and the prevention of digital stiffness.
Phase 1: Protection and Monitoring (Days 0 to 14)
Immediately postoperatively, the primary goal is flap survival. The hand is elevated continuously to optimize venous drainage and minimize interstitial edema. For the Cross Finger Flap, the digits are immobilized in a custom volar orthosis, ensuring absolutely no tension is placed on the pedicle bridge. For the RFF, the wrist is splinted in a neutral or slightly extended position. Clinical monitoring of flap perfusion (color, temperature, capillary refill, and turgor) is performed every 2 hours for the first 48 hours, then every 4 hours. The donor site dressings remain undisturbed unless there is suspicion of hematoma or infection. Uninvolved digits are encouraged to perform gentle active range of motion (AROM) to prevent global hand stiffness.
Phase 2: Flap Division and Early Motion (Weeks 2 to 4)
For the Cross Finger Flap, pedicle division is typically performed between days 14 and 21. This is executed under local anesthesia. The pedicle is sharply divided, and the margins are meticulously inset into both the donor and recipient fingers. Crucially, the inset must align perfectly with the midlateral line to prevent volar scar contractures. Immediately following division, aggressive AROM and gentle passive range of motion (PROM) of both the donor and recipient digits are initiated. For the RFF, the donor site graft is inspected at day 5-7. Once graft take is confirmed, gentle wrist AROM is initiated, avoiding extreme positions that could stretch the pedicle.
Phase 3: Scar Management and Stretching (Weeks 4 to 8)
As the wounds consolidate, the focus shifts to scar management and overcoming joint contractures. Silicone gel sheeting, elastomer molds, and deep friction massage are employed to soften the scars, particularly at the RFF donor site and the CFF inset lines. Dynamic or static progressive splinting may be introduced if PIP joint extension deficits persist in the CFF digits. Desensitization techniques are initiated to manage hypersensitivity as peripheral nerve ingrowth begins in the flaps.
Phase 4: Strengthening and Return to Function (Weeks 8 and beyond)
Once full range of motion is achieved and the soft tissues are stable, progressive strengthening is introduced. Grip and pinch strengthening exercises are utilized to restore functional capacity. For the RFF, specific attention is given to restoring forearm strength and addressing any residual deficits from the donor site. Patients are typically cleared for return
