Anterior Tarsal Wedge Osteotomy and Adjunctive Cavus Foot Corrections
Key Takeaway
The anterior tarsal wedge osteotomy is a powerful structural intervention for rigid cavus foot deformities. By resecting a dorsally based wedge across the midfoot, surgeons can effectively elevate the metatarsal heads and restore a plantigrade foot. This guide details the Cole midtarsal osteotomy, the Japas V-osteotomy, and adjunctive calcaneal procedures like the Dwyer and Samilson osteotomies, providing step-by-step surgical protocols, biomechanical principles, and postoperative management strategies for optimal patient outcomes.
PATHOPHYSIOLOGY AND BIOMECHANICS OF THE CAVUS FOOT
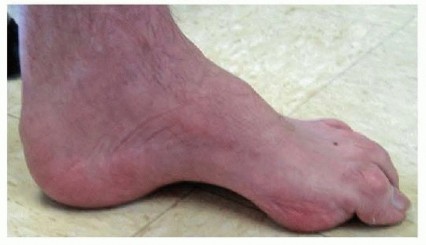
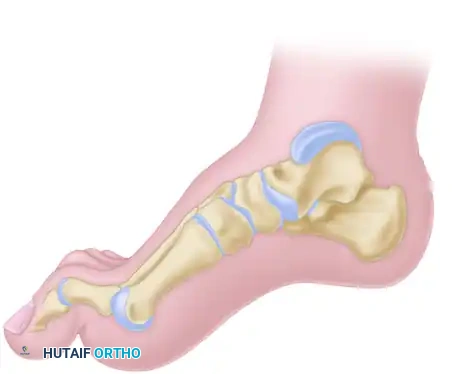
The cavus foot is a complex, multiplanar deformity characterized by an abnormally high medial longitudinal arch, often accompanied by hindfoot varus, forefoot equinus (plantarflexion), and clawing of the toes. The etiology is frequently neuromuscular, with Charcot-Marie-Tooth (CMT) disease being the most common cause, though poliomyelitis, spinal dysraphism, and idiopathic presentations are also encountered.
Surgical management of the rigid cavus foot requires a comprehensive understanding of foot biomechanics. The primary deforming force is often a plantarflexed first ray, driven by a strong peroneus longus overpowering a weak tibialis anterior. Over time, this flexible forefoot deformity drives the hindfoot into a compensatory, and eventually rigid, varus position.
When soft tissue releases (such as the Steindler plantar fasciotomy) and tendon transfers are insufficient to correct a rigid structural deformity, osseous interventions are mandated. The anterior tarsal wedge osteotomy (Cole procedure) and the V-osteotomy of the tarsus (Japas procedure) are foundational techniques designed to correct midfoot cavus by elevating the forefoot and restoring a plantigrade weight-bearing surface.
Clinical Pearl: Always perform a Coleman block test preoperatively. If the hindfoot varus corrects when the plantarflexed first ray is allowed to drop off the block, the hindfoot is flexible, and a forefoot/midfoot correction alone may suffice. If the hindfoot varus remains rigid, a concomitant calcaneal osteotomy (e.g., Dwyer) is strictly required.
PREOPERATIVE PLANNING AND INDICATIONS
Indications for Midtarsal Osteotomies
- Rigid anterior cavus deformity where the apex of the deformity is located at the midtarsal or tarsometatarsal joints.
- Failure of conservative management (custom orthotics, bracing).
- Progressive neuromuscular conditions where structural stabilization is required to prevent recurrent ulceration or severe gait impairment.
Radiographic Assessment
Standard weight-bearing anteroposterior (AP) and lateral radiographs of the foot are essential.
* Meary’s Angle: The angle between the longitudinal axis of the talus and the first metatarsal. In a cavus foot, this angle is increased (apex dorsal).
* Hibbs Angle: The angle between the longitudinal axis of the calcaneus and the first metatarsal. It approaches 90 degrees in severe cavus.
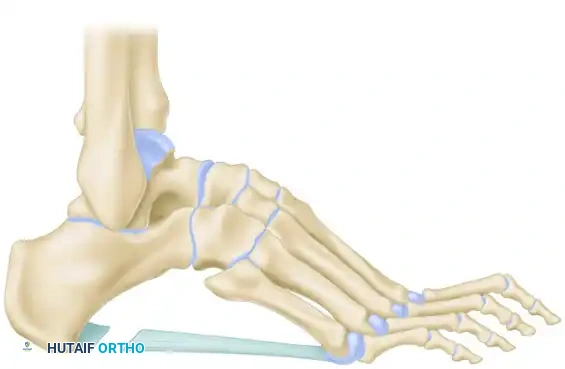
* Calcaneal Pitch: Often increased in true calcaneocavus deformities.

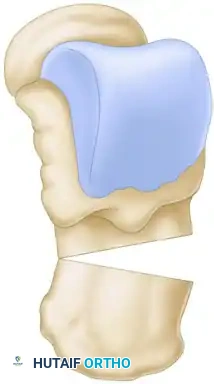
SURGICAL TECHNIQUE: ANTERIOR TARSAL WEDGE OSTEOTOMY (COLE)
The Cole procedure is a classic, dorsally based closing wedge osteotomy through the navicular-cuneiform and cuboid articulations. It is highly effective for correcting severe anterior cavus but does result in some shortening of the foot.
1. Positioning and Exposure
- Place the patient supine on the operating table with a bump under the ipsilateral hip to internally rotate the leg to a neutral position.
- Apply a well-padded thigh or calf tourniquet.
- Make a dorsal longitudinal incision in the midline of the foot. Begin the incision just proximal to the midtarsal joints (talonavicular and calcaneocuboid) and extend it distally to the level of the middle of the metatarsal shafts.
- Carefully dissect through the subcutaneous tissues, identifying and protecting the superficial peroneal nerve branches and the dorsalis pedis artery.
- Retract the extensor hallucis longus (EHL) and extensor digitorum longus (EDL) tendons to expose the underlying midtarsal bones.
2. Osteotomy Execution
- Identify the navicular, cuneiforms, and cuboid. The goal is to remove a dorsally based wedge of bone to elevate the metatarsal heads.
- Using an oscillating saw or sharp osteotomes, make the proximal cut through the center of the navicular and the cuboid.
- Make the distal cut through the proximal portions of the cuneiforms and the distal cuboid.
- Resection Parameters: Approximately 19 mm of bone should be removed from the second and third metatarsal-cuneiform joints, with slightly less removed from the first metatarsal-cuneiform articulation to accommodate the natural arch.
- If the first metatarsal is in marked, rigid equinus, carry the medial limb of the osteotomy directly through the base of the first metatarsal to ensure adequate correction of the medial column.
Surgical Warning: Do not over-resect the plantar cortex. The plantar cortex should act as a hinge. If the hinge is completely violated, the foot may become unstable, leading to a rocker-bottom deformity or nonunion.
3. Deformity Correction and Fixation
- Depress the proximal margin of the osteotomy plantarward while simultaneously elevating the metatarsal heads to close the dorsal gap.
- Correct any residual abduction or adduction deformity of the forefoot by simple manipulation before final fixation.
- Secure the osteotomy with heavy Steinmann pins, crossed cannulated screws, or a dorsal locking plate, depending on bone quality and surgeon preference.
SURGICAL TECHNIQUE: V-OSTEOTOMY OF THE TARSUS (JAPAS)
The Japas V-osteotomy was designed to correct cavus without shortening the foot as significantly as the Cole procedure. The apex of the "V" is located proximally within the navicular, with the limbs extending distally through the medial and lateral columns.
1. Soft Tissue Release (Steindler Stripping)
- Perform a Steindler plantar fasciotomy through a medial incision on the heel.
- Release the plantar fascia, the origin of the abductor hallucis, flexor digitorum brevis, and abductor digiti minimi from the calcaneal tuberosity. This allows the forefoot to elevate once the bone cuts are made.
2. Dorsal Approach and Exposure
- On the dorsum of the foot, make a longitudinal incision 6 to 8 cm long.
- Carry the dissection between the long extensor tendons of the second and third toes.
- Retract the extensor digitorum brevis (EDB) laterally.
- Expose the dorsum of the foot extraperiosteally from the talonavicular joint proximally to the tarsometatarsal joints distally.
3. Executing the V-Osteotomy
- Using a power saw, chisel, and osteotome, outline the V-osteotomy.
- Medial Limb: Begin the medial limb of the osteotomy in the first cuneiform, immediately proximal to the first metatarsal-cuneiform joint.
- Lateral Limb: Begin the lateral limb in the cuboid, immediately proximal to the joint between the cuboid and the fifth metatarsal.
- Apex: Carry these limbs proximally to join in the midline of the foot at the apex of the cavus deformity, which is usually located within the substance of the navicular.
Pitfall: Strictly avoid entering the midtarsal joint (talonavicular and calcaneocuboid joints). Violating these joints will lead to severe postoperative stiffness and degenerative arthritis.

4. Correction and Fixation
- After the osteotomy has been completed, apply longitudinal traction to the forefoot and depress the metatarsal heads in a dorsal direction to flatten the longitudinal arch.
- When proper alignment has been obtained, fix the osteotomy with one or two stout Steinmann pins inserted in a retrograde or antegrade fashion across the osteotomy site.
- Remove the tourniquet, obtain meticulous hemostasis, and close the incisions in layers.
- If lengthening of the Achilles tendon (TAL) or gastrocnemius recession is necessary to correct hindfoot equinus, perform this procedure after the tarsal osteotomy has been stabilized.

ADJUNCTIVE HINDFOOT OSTEOTOMIES
When the cavus deformity is accompanied by a rigid hindfoot varus or severe calcaneocavus, midtarsal osteotomies alone are insufficient. Calcaneal osteotomies must be performed concomitantly to realign the mechanical axis of the hindfoot.
Dwyer Lateral Closing Wedge Osteotomy
The Dwyer osteotomy is indicated for rigid hindfoot varus. It involves resecting a laterally based wedge of bone from the calcaneus to valgus-producing alignment.
- Make a curved lateral incision posterior and inferior to the lateral malleolus, avoiding the sural nerve.
- Incise the periosteum and reflect it to expose the lateral wall of the calcaneus.
- A wedge of bone with its base lateral is resected just inferior and posterior to the peroneus longus tendon, running parallel to it.
- Crucial Step: The medial cortex of the calcaneus is not divided with the saw. Instead, it is broken manually (greenstick fracture) to close the gap, preserving the medial periosteal hinge and protecting the neurovascular bundle.
- Close the osteotomy by everting the heel and fix it with a single cannulated screw or staple.

Samilson Crescentic Osteotomy
The Samilson osteotomy is utilized for calcaneocavus deformities where the calcaneal pitch is excessively high.
- A lateral approach to the calcaneus is utilized.
- A crescentic (dome-shaped) bone cut is made through the calcaneal tuberosity.
- The posterior fragment is displaced dorsally and translated laterally if varus correction is also needed.
- This technique allows for multiplanar correction without sacrificing calcaneal height or creating a prominent bony step-off on the plantar surface.
- Fixation is typically achieved with two large-fragment cannulated screws directed from the posterior tuberosity into the anterior calcaneal body.



POSTOPERATIVE CARE AND REHABILITATION
Strict adherence to postoperative protocols is vital to ensure bony union and prevent loss of correction.
- Immediate Postoperative Phase (0-2 Weeks):
- Apply a well-padded, short-leg splint or cast from the base of the toes to the tibial tuberosity in the operating room.
- The limb is strictly elevated above heart level to minimize edema and prevent wound complications.
- The patient is strictly non-weight-bearing (NWB).
- Intermediate Phase (2-8 Weeks):
- At 2 weeks, sutures are removed, and a rigid fiberglass short-leg cast is applied.
- The patient remains NWB.
- At 8 weeks (2 months), the cast and any percutaneous Steinmann pins are removed in the clinic.
- The foot is examined clinically for stability, and weight-bearing radiographs are obtained to confirm osseous union.
- Rehabilitation Phase (8-12 Weeks):
- If radiographic union is progressing satisfactorily, a walking boot cast (CAM boot) is applied.
- The patient is allowed to transition to weight-bearing as tolerated (WBAT) in the boot for 1 month.
- At 12 weeks, the boot is discontinued, and formal physical therapy is initiated. Therapy focuses on restoring ankle and subtalar range of motion, peroneal strengthening, and gait retraining.
COMPLICATIONS AND MANAGEMENT
While highly effective, midtarsal and hindfoot osteotomies carry specific risks that the orthopedic surgeon must anticipate:
- Nonunion or Delayed Union: The midfoot has a robust blood supply, but excessive periosteal stripping or thermal necrosis from power saws can impair healing. Ensure copious irrigation during bone cuts and rigid internal fixation.
- Under-correction: Often results from failing to recognize a rigid hindfoot varus (failure to perform a Dwyer) or inadequate soft tissue release (omitting the Steindler stripping).
- Over-correction (Rocker-Bottom Foot): Occurs if the plantar cortex is completely resected and the forefoot is excessively dorsiflexed during a Cole procedure. Careful preoperative templating is required.
- Nerve Injury: The superficial peroneal nerve is at high risk during the dorsal approach for the Cole and Japas procedures. The sural nerve is at risk during the Dwyer and Samilson lateral approaches. Meticulous blunt dissection and appropriate retraction are mandatory.
By mastering these foundational osteotomies and understanding the complex biomechanics of the cavus foot, the orthopedic surgeon can reliably restore a stable, plantigrade, and functional foot for patients suffering from severe structural deformities.
You Might Also Like