Comprehensive Introduction and Patho-Epidemiology
Epidemiology of Forefoot Entrapment Neuropathies
Nerve entrapment syndromes of the foot and ankle present a remarkably complex diagnostic and therapeutic challenge for the orthopedic surgeon. Among the most clinically significant, yet frequently misdiagnosed or underappreciated, are Anterior Tarsal Tunnel Syndrome (ATTS) and Interdigital Neuritis (commonly, albeit incorrectly, referred to as Morton's Neuroma). The epidemiological profile of these two distinct entities varies significantly, dictating a high index of suspicion during clinical evaluation. Interdigital neuritis is overwhelmingly prevalent in the female population, with a female-to-male ratio frequently reported as high as 4:1 to 10:1. This stark demographic skew is largely attributed to extrinsic biomechanical factors, predominantly the utilization of restrictive, narrow toe-box footwear with elevated heels, which exponentially increases compressive forces across the forefoot. The peak incidence of interdigital neuritis occurs in the fifth and sixth decades of life, correlating with the cumulative effects of chronic microtrauma and age-related attenuation of the plantar fat pad.
Conversely, Anterior Tarsal Tunnel Syndrome is a far more insidious and less epidemiologically defined condition. ATTS involves the compression of the deep peroneal nerve beneath the unyielding inferior extensor retinaculum. It does not exhibit the same profound gender disparity as interdigital neuritis and is more frequently associated with specific anatomical variations, prior trauma, or space-occupying lesions such as dorsal midfoot osteophytes or ganglion cysts. Athletes, particularly runners and dancers, who subject their midfoot to repetitive extreme plantarflexion, are at an elevated risk for developing ATTS. The true incidence of ATTS is likely underestimated in the general population, as its symptoms—vague dorsal midfoot pain and isolated first web space paresthesias—are frequently misattributed to extensor tendinopathy, midfoot osteoarthritis, or L5 radiculopathy.
Understanding the distinct epidemiological landscapes of these neuropathies is paramount for the treating physician. While interdigital neuritis is a ubiquitous presentation in any high-volume foot and ankle clinic, ATTS remains an elusive "zebra" that requires meticulous clinical acumen to isolate. The failure to recognize the epidemiological and demographic clues often leads to protracted conservative management failures, unnecessary advanced imaging, and delayed surgical intervention, ultimately compromising the patient's functional outcome and quality of life.
Pathophysiology of Anterior Tarsal Tunnel Syndrome
The pathophysiology of Anterior Tarsal Tunnel Syndrome is fundamentally rooted in the anatomical constraints of the anterior ankle and dorsal midfoot. As the deep peroneal nerve descends into the foot, it must traverse a rigid fibro-osseous tunnel. The roof of this tunnel is formed by the cruciform inferior extensor retinaculum, while the floor consists of the talonavicular and naviculocuneiform joint capsules. Any alteration in the volume of this confined space precipitates a compressive neuropathy. The pathophysiology is primarily mechanical; compression induces localized nerve ischemia, leading to a breakdown of the blood-nerve barrier, endoneurial edema, and subsequent localized demyelination. If the compression remains unaddressed, the pathology progresses to Wallerian degeneration of the distal axonal segments, manifesting clinically as irreversible sensory deficits and motor atrophy of the extensor digitorum brevis (EDB).
The etiology of this spatial compromise is multifactorial. The most frequent intrinsic cause is the development of dorsal osteophytes at the talonavicular joint, a common sequela of midfoot osteoarthritis or prior athletic trauma. These bony prominences act as an anvil against which the deep peroneal nerve is repeatedly compressed during the gait cycle, particularly during the toe-off phase when the midfoot experiences maximum loading. Additionally, occult ganglion cysts originating from the underlying joint capsules frequently migrate dorsally, insinuating themselves beneath the retinaculum and exerting direct hydrostatic pressure on the nerve.
Extrinsic factors also play a critical pathophysiological role. Repetitive microtrauma from tightly laced footwear, rigid ski boots, or specialized athletic footwear can induce a hypertrophic fibrotic response within the inferior extensor retinaculum itself. This localized fascial thickening reduces the compliance of the retinacular roof, transforming a dynamic anatomical passage into a static, constricting bottleneck. The orthopedic surgeon must appreciate that ATTS is rarely a spontaneous idiopathic event; it is almost universally the end-stage clinical manifestation of an identifiable biomechanical or structural abnormality that must be addressed concurrently during surgical decompression.
Pathophysiology and Histology of Interdigital Neuritis
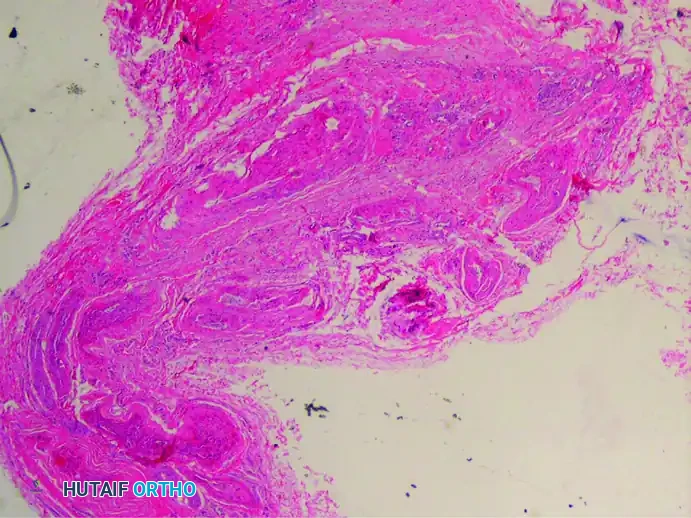
While ATTS is a classic entrapment neuropathy, interdigital neuritis represents a profound degenerative process. Despite the ubiquitous use of the term "neuroma," extensive histological analysis unequivocally reveals that this condition is not a true neoplastic or proliferative neuroma. A true traumatic neuroma exhibits a haphazard, disorganized proliferation of axonal sprouts attempting to bridge a nerve gap. This proliferative axonal sprouting is entirely absent in Morton's neuroma. Instead, the gross enlargement of the nerve is accounted for by the massive deposition of hyaline and collagenous material, making the terms interdigital neuritis or perineural fibroma scientifically accurate.
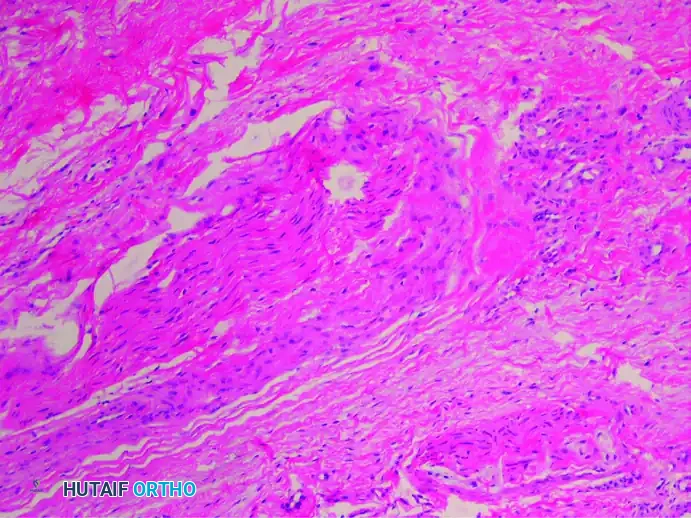
Histological examination of excised interdigital neuromas reveals a consistent triad of perineural fibrosis, vascular degeneration, and axonal loss. The interdigital nerve becomes greatly thickened by dense, concentric layers of perineural fibrous tissue. This fibrosis acts as a constricting scar around the nerve fascicles, severely compromising the microvascular circulation.
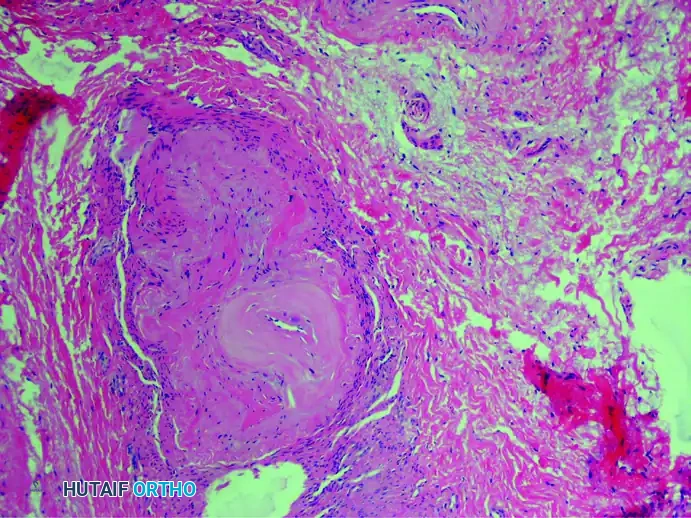
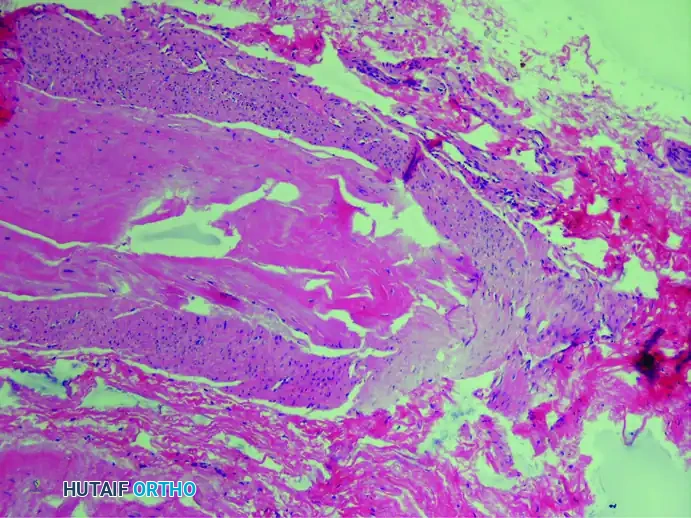
Furthermore, there is profound vascular degeneration of the vasa nervorum. There is a markedly increased number of intrafascicular arterioles, but these vessels exhibit thickened, hyalinized walls caused by the deposition of multiple layers of basement membranes. Degenerative changes such as the fraying and duplication of the internal elastic lamina are frequently observed, leading to localized nerve ischemia.
Secondary to this chronic compression and ischemia, there is profound demyelinization and degeneration of the nerve fibers. Histological stains specific for nerve tissue, such as the Bielschowsky stain, reveal a significant decrease in the total number of viable axis cylinders.
It is also highly frequent to find reactive bursal tissue accompanying the excised nerve specimen. This intermetatarsal bursitis is often the initial source of inflammation that subsequently leads to the perineural fibrosis of the adjacent nerve.
Detailed Surgical Anatomy and Biomechanics
Osteoligamentous Boundaries of the Anterior Tarsal Tunnel
The anterior tarsal tunnel is a complex fibro-osseous space situated over the dorsum of the midfoot. A profound understanding of its boundaries is essential for safe and effective surgical decompression. The roof of the tunnel is formed by the inferior extensor retinaculum, a Y-shaped or cruciform fascial band. The stem of this "Y" originates laterally from the superior surface of the calcaneus, anterior to the sulcus calcanei. As it courses medially over the dorsum of the foot, it splits into two bands: an upper band that attaches to the medial malleolus, and a lower band that blends with the plantar aponeurosis medially. The deep peroneal nerve and the dorsalis pedis artery pass beneath this unyielding structure.
The floor of the anterior tarsal tunnel is composed of the osseous and capsular structures of the dorsal midfoot, predominantly the talus, navicular, and the intervening talonavicular joint capsule. Distally, the floor extends to encompass the naviculocuneiform joints. Because the deep peroneal nerve lies directly upon these capsular structures, it is exquisitely vulnerable to compression from any dorsal osteophytosis or capsular hypertrophy. The medial and lateral boundaries are less rigidly defined but are functionally constrained by the tendons of the extensor hallucis longus (EHL) medially and the extensor digitorum longus (EDL) laterally.
Within this tunnel, the deep peroneal nerve is accompanied by the dorsalis pedis artery and its venae comitantes. The artery typically lies medial to the nerve, serving as a critical intraoperative landmark. However, anatomical variants are common, and the surgeon must be prepared for the nerve to cross anterior to the artery or to bifurcate unusually proximal to the retinaculum. The tight spatial constraints of this fibro-osseous tunnel mean that even millimeter-scale increases in volume—whether from a ganglion, osteophyte, or localized edema—can rapidly exceed the compliance of the retinaculum, precipitating the ischemic cascade of ATTS.
Course and Arborization of the Deep Peroneal Nerve
The deep peroneal nerve originates from the bifurcation of the common peroneal nerve at the fibular neck. It descends through the anterior compartment of the leg, providing motor innervation to the tibialis anterior, EHL, EDL, and peroneus tertius. As it approaches the ankle joint, it courses deep to the superior extensor retinaculum, crossing the anterior capsule of the ankle joint. Upon entering the dorsum of the foot beneath the inferior extensor retinaculum, the nerve typically undergoes a critical bifurcation into medial and lateral terminal branches.
The medial terminal branch is primarily sensory. It courses distally alongside the dorsalis pedis artery, eventually diving deep to the EHB tendon. It provides sensory innervation to the dorsal aspect of the first web space, communicating with branches of the superficial peroneal nerve. The lateral terminal branch is primarily motor. It curves laterally beneath the EDB and EHB muscle bellies, providing their essential motor innervation. Crucially, this lateral branch also gives off multiple articular branches to the tarsal and tarsometatarsal joints.
Compression within the anterior tarsal tunnel typically affects the nerve prior to its bifurcation, resulting in a mixed clinical picture of first web space numbness and EDB weakness. However, selective entrapment of either the medial or lateral branch can occur distal to the retinaculum. For instance, tight footwear can selectively compress the medial sensory branch against the dorsal cuneiforms, producing pure sensory symptoms without motor deficits. A meticulous preoperative clinical examination is required to map the exact arborization pattern affected, which directly dictates the extent and location of the surgical release.
Anatomy of the Intermetatarsal Space and Common Digital Nerves
The intermetatarsal spaces of the forefoot house the neurovascular bundles responsible for the distal toes. The common digital nerves, branches of the medial and lateral plantar nerves, course plantarly to the deep transverse intermetatarsal ligament (DTIML). The DTIML is a strong, unyielding band of fibrous tissue that connects the plantar plates of the adjacent metatarsophalangeal (MTP) joints, effectively tethering the metatarsal heads together and preventing excessive splaying of the forefoot during weight-bearing.
The third intermetatarsal space is the most frequent site of interdigital neuritis, accounting for approximately 80-85% of cases, followed by the second intermetatarsal space. The anatomical predisposition of the third web space is largely attributed to its unique innervation pattern. The third common digital nerve frequently receives communicating branches from both the medial and lateral plantar nerves. This dual tethering creates a thicker nerve trunk that is relatively fixed in position, rendering it highly susceptible to mechanical shearing forces against the distal edge of the DTIML.
Distal to the DTIML, the common digital nerve bifurcates into the proper digital nerves, which supply the adjacent sides of the toes. The nerve is intimately accompanied by the common digital artery and vein. As demonstrated by Su et al., the digital artery is intertwined with the nerve in a dense fibrotic mass in the presence of a neuroma, leading to a high rate of inadvertent arterial excision during neurectomy (up to 39%). The surgeon must possess a profound three-dimensional understanding of this intermetatarsal anatomy to safely navigate the neurectomy, ensuring complete resection of the pathological nerve while minimizing collateral damage to the surrounding lumbrical musculature and vascular structures.
Biomechanical Etiology of Nerve Compression
The pathogenesis of both ATTS and interdigital neuritis is inextricably linked to the biomechanics of the human gait cycle. During the terminal stance phase of gait, the heel rises, and the body weight is transferred entirely to the forefoot. This action forces the MTP joints into maximum dorsiflexion. In the intermetatarsal space, this dorsiflexion stretches the common digital nerve tightly across the distal, unyielding edge of the DTIML. This phenomenon, known as the bowstringing effect, subjects the nerve to immense tensile and compressive forces.
When this physiological bowstringing is compounded by extrinsic factors—such as high-heeled shoes that pre-position the MTP joints in dorsiflexion, or narrow toe-boxes that laterally compress the metatarsal heads—the mechanical threshold of the nerve is rapidly exceeded. The repetitive mechanical shearing against the ligament initiates the cascade of localized trauma, intermetatarsal bursitis, ischemia of the vasa nervorum, and ultimately, irreversible perineural fibrosis.
Similarly, the biomechanics of the midfoot heavily influence the development of ATTS. During the toe-off phase, the midfoot joints experience significant compressive loading. Over time, this loading can stimulate the formation of dorsal osteophytes at the talonavicular joint. Furthermore, extreme plantarflexion of the ankle and midfoot, as seen in ballet dancers (en pointe) or soccer players, maximally stretches the deep peroneal nerve against the anterior ankle capsule and the inferior extensor retinaculum. This repetitive traction-compression dynamic induces a localized inflammatory response, leading to retinacular hypertrophy and subsequent entrapment. A thorough biomechanical assessment is therefore a mandatory component of the preoperative evaluation for any forefoot nerve entrapment syndrome.
Exhaustive Indications and Contraindications
Clinical Evaluation and Provocative Testing
Accurate clinical diagnosis relies heavily on targeted physical examination maneuvers designed to reproduce the patient's symptoms by compressing the enlarged nerve against the deep transverse intermetatarsal ligament or the inferior extensor retinaculum. For interdigital neuritis, the Squeeze Test, or Mulder's Sign, is the pathognomonic clinical maneuver. Digital manipulation is performed with pressure applied just proximal to the metatarsal heads. The examiner squeezes the forefoot between the index finger and thumb, compressing the metatarsal heads together. This action forces the thickened nerve plantarward, often producing a palpable and audible "click" (Mulder's click) accompanied by sharp, radiating pain into the affected toes.

Additionally, Web Space Compression is highly sensitive. Simultaneous compression of the forefoot with one hand and direct plantar-to-dorsal compression of the affected web space with two fingers of the opposite hand will exquisitely localize the pain to the affected interdigital nerve.

For Anterior Tarsal Tunnel Syndrome, the clinical evaluation must isolate the deep peroneal nerve. A positive Tinel's sign localized strictly over the deep peroneal nerve at the level of the inferior extensor retinaculum, combined with isolated first web space paresthesia, is highly indicative of ATTS. The examiner must also assess the motor function of the EDB. Atrophy or weakness of the EDB, visualized as a loss of the normal muscle belly prominence on the lateral dorsum of the foot during resisted toe extension, signifies advanced motor branch entrapment and mandates expeditious surgical intervention.
Diagnostic Imaging and Electrodiagnostic Modalities
While the diagnosis of forefoot entrapment neuropathies is primarily clinical, advanced imaging and electrodiagnostic studies play a critical role in preoperative planning and ruling out confounding pathologies. For interdigital neuritis, high-resolution ultrasound is widely considered the imaging modality of choice. It allows for dynamic assessment of the intermetatarsal space; the sonographer can perform a Mulder's maneuver under real-time visualization to observe the neuroma displacing plantarly beneath the DTIML. Magnetic Resonance Imaging (MRI) is also highly sensitive and specific, typically demonstrating a teardrop-shaped mass in the intermetatarsal space that is hypointense on T1 and T2-weighted sequences, distinguishing it from the hyperintense signal of an isolated intermetatarsal bursitis.
For Anterior Tarsal Tunnel Syndrome, weight-bearing radiographs of the foot are mandatory to evaluate for dorsal midfoot osteophytosis, midfoot osteoarthritis, or subtle malalignments. MRI is indispensable for identifying space-occupying lesions such as occult ganglion cysts, tenosynovitis of the extensor tendons, or severe retinacular hypertrophy.
Electrodiagnostic studies, including Electromyography (EMG) and Nerve Conduction Velocities (NCV), are highly valuable in the workup of ATTS. A prolonged distal motor latency to the EDB or decreased sensory nerve action potentials (SNAPs) at the first web space confirm the diagnosis and objectively quantify the severity of the neuropathy. Furthermore, EMG/NCV studies are critical for ruling out proximal lesions, such as L5 radiculopathy or common peroneal nerve entrapment at the fibular head, which can present with overlapping clinical symptoms.
Surgical Indications and Contraindications
Surgical intervention for both ATTS and interdigital neuritis is indicated only after the rigorous exhaustion of conservative measures. For interdigital neuritis, conservative management includes wide toe-box footwear, metatarsal pads to splay the metatarsal heads, NSAIDs, and ultrasound-guided corticosteroid or alcohol sclerosing injections. Failure of these modalities over a 3-to-6-month period, accompanied by persistent pain that limits activities of daily living, constitutes a strong surgical indication. For ATTS, indications include persistent first web space paresthesias, progressive EDB weakness, or the presence of a definitive space-occupying lesion (e.g., ganglion cyst) causing mechanical compression.
Contraindications to surgical intervention must be carefully respected to avoid catastrophic postoperative outcomes. Absolute contraindications include active local or systemic infection, severe peripheral vascular disease precluding adequate wound healing, and poorly controlled medical comorbidities. Relative contraindications include profound uncontrolled diabetes mellitus with severe generalized peripheral neuropathy, as the surgical release may not yield symptomatic improvement if the underlying nerve architecture is globally compromised. Furthermore, patients exhibiting signs of active Complex Regional Pain Syndrome (CRPS) should not undergo elective nerve surgery until the sympathetic dystrophy is aggressively managed and stabilized.
| Parameter | Anterior Tarsal Tunnel Syndrome (ATTS) | Interdigital Neuritis (Morton's Neuroma) |
|---|---|---|
| Primary Surgical Indications | Failed conservative therapy (>3-6 months); Progressive EDB motor weakness; Intractable 1st web space pain; Confirmed space-occupying lesion (ganglion/osteophyte); Positive EMG/NCS confirming isolated deep peroneal entrapment. | Failed conservative therapy (shoe modification, orthotics, injections); Intractable pain limiting ambulation; Positive Mulder's click with failed injection therapy; MRI/Ultrasound confirmed >5mm neuroma. |
| Absolute Contraindications | Active local infection; Severe peripheral arterial disease (ABI < 0.5); Active Complex Regional Pain Syndrome (CRPS). | Active local infection; Severe vascular insufficiency; Active CRPS; Diagnostic uncertainty (e.g., overlapping metatarsalgia). |
| Relative Contraindications | Severe generalized diabetic sensorimotor polyneuropathy; Unrealistic patient expectations; Active psychiatric overlay. | Multiple adjacent web space neuromas (high risk of failure); Severe untreated hallux valgus/metatarsal cascade abnormalities; Generalized peripheral neuropathy. |
| Timing of Intervention | Expeditious if progressive motor atrophy (EDB) is present; otherwise elective after 3-6 months of conservative care. | Elective, strictly after failure of comprehensive conservative protocol (typically 4-6 months). |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Review and Templating
Preoperative planning for forefoot nerve decompression requires a meticulous review of all diagnostic imaging to formulate a precise surgical blueprint. For ATTS, the surgeon must correlate the exact site of maximum Tinel's sign with the MRI and radiographic findings. If dorsal osteophytes are identified on the lateral weight-bearing radiograph, the surgeon must template the extent of the required exostectomy. The goal is to resect sufficient bone to create a completely flat, tension-free bed for the deep peroneal nerve, without compromising the structural integrity of the talonavicular or naviculocuneiform joints. If a ganglion cyst is identified on MRI, the surgeon must trace its stalk to the joint of origin, as failure to excise the capsular base of the stalk guarantees a high rate of recurrence.
For interdigital neurectomy, MRI review is critical for confirming the exact web space involved and ruling out adjacent web space neuromas. While concurrent adjacent neuromas (e.g., 2nd and 3rd web spaces simultaneously) are exceedingly rare, they do occur and drastically alter the surgical approach. The surgeon must also evaluate the MRI for associated pathologies, such as a plantar plate tear, severe MTP joint synovitis, or a Freiberg's infraction, which could mimic or exacerbate the neuroma symptoms. Preoperative templating ensures that the surgical incision is accurately placed and that all concurrent pathologies are addressed through a single, optimized approach.
Anesthetic Considerations and Tourniquet Application
The choice of anesthesia and hemostatic control is critical for optimizing the surgical field and ensuring patient comfort. For both ATTS release and interdigital neurectomy, a regional anesthetic approach is highly preferred over general anesthesia. A popliteal sciatic nerve block, combined with a saphenous nerve block, provides excellent intraoperative anesthesia and profound, long-lasting postoperative analgesia. Alternatively, a highly targeted ankle block utilizing a long-acting local anesthetic (e.g., bupivacaine or ropivacaine) can be employed for shorter, less complex primary procedures.
A bloodless surgical field is an absolute prerequisite for peripheral nerve surgery in the foot. Even minor capillary bleeding can obscure the delicate arborization of the deep peroneal nerve or the intricate relationship between the common digital nerve and artery. Therefore, a pneumatic tourniquet is mandatory. For isolated forefoot procedures, an ankle or calf tourniquet inflated to 250 mmHg following meticulous exsanguination with an Esmarch bandage is highly effective and minimizes the thigh discomfort associated with proximal tourniquets. The tourniquet time must be strictly monitored, and if the procedure exceeds 120 minutes, the tourniquet must be deflated to allow for reperfusion before re-inflation.
Patient Positioning and Operating Room Setup
Proper patient positioning is essential to provide optimal exposure of the dorsal midfoot and forefoot. The patient is placed in the supine position on the operating table. Because the lower extremity naturally rests in external rotation, a padded bump or sandbag is placed under the ipsilateral hip. This internally rotates the leg to a neutral position, bringing the dorsum of the foot perfectly parallel to the ceiling and providing the surgeon with an unhindered, ergonomic approach to the anterior tarsal tunnel and the intermetatarsal spaces.
The operating room setup should include high-intensity, focused overhead lighting. Given the microscopic nature of the neurovascular structures, the use of surgical loupes (minimum 2.5x to 3.5x magnification) is strongly recommended, and some advanced peripheral nerve surgeons advocate for the use of an operating microscope during complex revision cases. Bipolar electrocautery must be available and tested prior to the incision, as monopolar cautery carries an unacceptably high risk of thermal injury to the adjacent peripheral nerves. The surgical technician should have a complete set of delicate soft tissue instruments available, including tenotomy scissors, fine dissecting forceps, and small blunt retractors (e.g., Senn or Ragnell retractors).
Step-by-Step Surgical Approach and Fixation Technique
Anterior Tarsal Tunnel Release (Mann's Approach)
The surgical technique for anterior tarsal tunnel release, popularized by Mann and Baxter, emphasizes a targeted, minimally invasive release of the constricting structures to preserve the biomechanical integrity of the extensor mechanism.
Step 1: Incision and Superficial Dissection
Following exsanguination and tourniquet inflation, a longitudinal incision, approximately 5 to 7 cm in length, is made over the dorsum of the foot. The incision is centered over the maximum point of compression, typically extending from the level of the talonavicular joint distally toward the first intermetatarsal space. The subcutaneous tissues are carefully divided. Extreme caution must be exercised during this superficial dissection to identify and gently retract any crossing branches of the superficial peroneal nerve. Laceration of these branches will result in a highly symptomatic, recalcitrant postoperative neuroma that often eclipses the original ATTS symptoms.
Step 2: Deep Dissection and Nerve Identification
The deep fascia and the inferior extensor retinaculum are identified. The surgeon must locate the dorsalis pedis artery by palpation (if the tourniquet is not yet inflated) or by anatomical visualization. The deep peroneal nerve typically lies immediately adjacent, usually lateral, to the artery. Using fine tenotomy scissors, the paravascular sheath is opened, and the deep peroneal nerve is definitively identified and isolated with a vessel loop. The nerve is then traced distally as it courses beneath the extensor hallucis brevis muscle belly.
Step 3: Retinacular Release and Decompression
Once the nerve is fully isolated, the surgeon identifies the specific constricting portion of the inferior extensor retinaculum. Mann and Baxter strongly recommend releasing only the portion of the retinaculum that is actively constricting the nerve. Complete, aggressive division of the entire retinaculum can lead to catastrophic extensor tendon bowstringing and subsequent biomechanical dysfunction of the forefoot. The constricting fascial bands are carefully divided using tenotomy scissors, ensuring the nerve is strictly protected with a blunt elevator or right-angle forceps during the release.
Step 4: Addressing Underlying Pathology and Closure
The floor of the anterior tarsal tunnel is meticulously inspected. If a ganglion cyst is present, it is excised down to its capsular stalk, and the capsular defect is lightly cauterized to prevent recurrence. If dorsal osteophytes are the source of compression, a rongeur or a small osteotome is utilized to resect the bony prominences until the nerve bed is completely flat and free of tension. Bone wax may be applied to the raw cancellous bone to minimize postoperative hematoma. The tourniquet is deflated, and absolute hemostasis is achieved using bipolar electrocautery. Hematoma formation in this tight space is a primary cause of recurrent scarring and entrapment. The subcutaneous tissue is closed with 3-0 or 4-0 absorbable sutures, and the skin is approximated with non-absorbable monofilament sutures in a tension-free manner.
Dorsal Approach for Interdigital Neurectomy
The dorsal approach is the gold standard for primary interdigital neurectomy, offering excellent visualization while avoiding a potentially painful plantar scar on the weight-bearing surface of the foot.
Step 1: Incision and Dissection
A 3 to 4 cm longitudinal incision is made in the dorsal web space, centered between the metatarsal heads. Blunt dissection with a hemostat is used to separate the subcutaneous fat and expose the deep transverse intermetatarsal
