Ankle Injuries Weber A
Introduction & Epidemiology
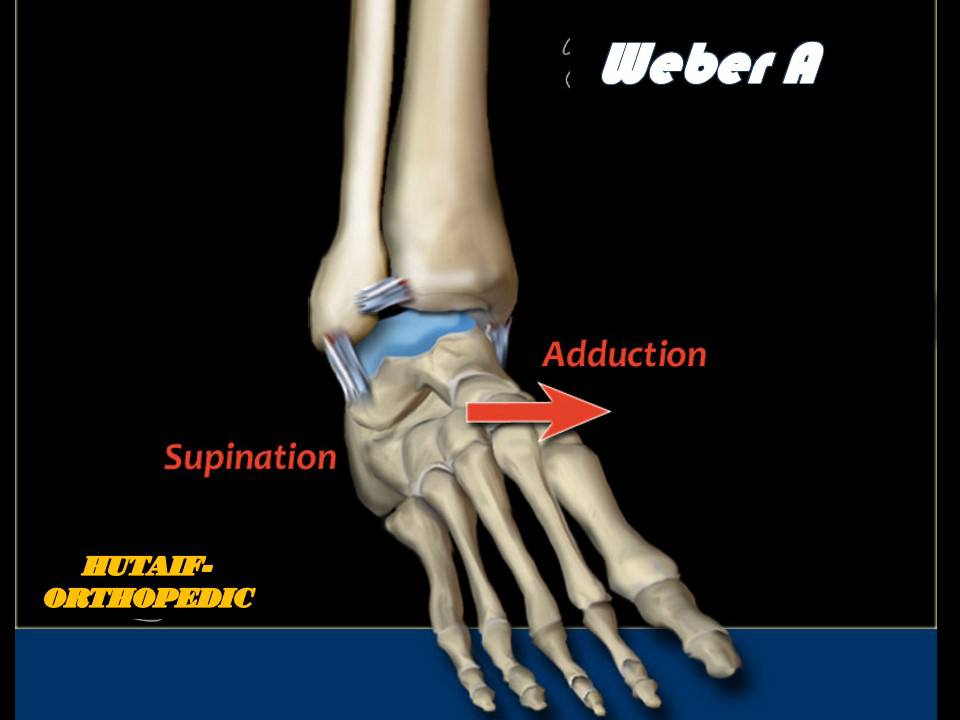
Ankle fractures represent a significant burden on healthcare systems and functional patient outcomes, with an incidence of approximately 100-200 per 100,000 person-years. The classification of ankle fractures is fundamental to guiding treatment strategies and predicting outcomes. The AO/Danis-Weber classification system, widely adopted for its prognostic value, categorizes lateral malleolar fractures based on their relationship to the syndesmosis. Weber A fractures are defined as extra-articular fractures of the fibula distal to the level of the syndesmosis. This classification inherently implies an intact syndesmosis, making these injuries generally stable.
Based on the Lauge-Hansen classification system, Weber A fractures most commonly result from a supination-adduction (SA) mechanism. This typically involves an adduction force applied to a supinated foot, leading to a transverse fracture of the lateral malleolus below the level of the tibiotalar joint line and syndesmosis, often accompanied by either an impaction fracture of the medial malleolus or a tear of the deltoid ligament. However, the integrity of the deltoid ligament and syndesmosis, in the absence of a medial malleolus fracture, typically ensures overall ankle stability. Isolated Weber A fractures are intrinsically stable injuries due to the robust ligamentous structures of the ankle mortise remaining intact superior to the fracture.
The accurate diagnosis and classification of Weber A fractures are critical to avoid both undertreatment of unstable injuries (misdiagnosed as stable Weber A) and overtreatment of genuinely stable ones. While most Weber A fractures are amenable to non-operative management, the presence of associated medial pathology or significant displacement can necessitate surgical intervention. This review will delve into the comprehensive management of Weber A ankle fractures, emphasizing the nuanced decision-making process for operative versus non-operative care.

Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the ankle joint is paramount for managing Weber A fractures. The ankle is a hinge joint formed by the distal tibia (plafond and medial malleolus), the distal fibula (lateral malleolus), and the talus. The stability of this mortise is maintained by a complex array of bony architecture and ligamentous restraints.
Bony Anatomy
- Tibia: The distal tibia forms the medial malleolus and the weight-bearing surface of the plafond. The medial malleolus provides medial stability and is an attachment site for the deltoid ligament.
- Fibula: The distal fibula forms the lateral malleolus, which articulates with the lateral aspect of the talus. It acts as a buttress against lateral talar displacement and serves as the origin for the lateral collateral ligaments. In a Weber A fracture, the fibula fractures below the level of the tibiotalar joint and syndesmosis. The fracture line is typically transverse or minimally oblique.
- Talus: The talus articulates with the tibia and fibula superiorly and laterally, respectively. Its trochlea is wider anteriorly than posteriorly, contributing to ankle stability in dorsiflexion.
Ligamentous Anatomy
The major ligamentous stabilizers of the ankle include:
*
Lateral Collateral Ligament Complex:
Composed of the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular ligament (PTFL). These ligaments resist inversion and internal rotation. The ATFL is the weakest and most commonly injured.
*
Medial Collateral Ligament (Deltoid Ligament):
A strong, fan-shaped ligament with superficial and deep components. It resists eversion and external rotation, attaching from the medial malleolus to the talus, calcaneus, and navicular. Its integrity is crucial for medial ankle stability.
*
Syndesmotic Ligaments:
These robust ligaments bind the distal tibia and fibula, forming the tibiofibular syndesmosis. They include the anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), and the interosseous membrane (IOM) extending proximally from the interosseous ligament (IOL). The syndesmosis prevents excessive external rotation and superior translation of the fibula relative to the tibia.
In Weber A fractures, the syndesmosis is by definition intact.
Biomechanics of Weber A Injuries
As previously noted, Weber A fractures typically result from a supination-adduction mechanism. The sequence of injury under such forces is generally:
1.
Stage I:
A transverse fracture of the lateral malleolus occurs distal to the syndesmosis. This is the hallmark of a Weber A injury. The adduction force creates a tension failure laterally.
2.
Stage II:
If the adduction force continues, it may lead to impaction of the medial talus against the medial malleolus, causing a vertical or oblique fracture of the medial malleolus, or a tear of the deltoid ligament.
The critical biomechanical aspect differentiating Weber A from higher-grade ankle fractures (Weber B and C) is the intact syndesmosis . The integrity of the syndesmosis ensures that the tibiofibular relationship, and thus the stability of the ankle mortise, remains preserved. Even in the presence of a medial malleolus fracture or deltoid ligament disruption, if the fibular fracture is truly a Weber A (distal to the syndesmosis) and the syndesmosis itself is uninjured, the overall stability profile is generally superior to those with syndesmotic compromise. The strength of the deltoid ligament in resisting talar tilt and the intact syndesmosis are key to the inherent stability of this fracture pattern.

Indications & Contraindications
The decision-making process for operative versus non-operative management of Weber A ankle fractures hinges primarily on the stability of the ankle mortise. Given the definition of a Weber A fracture—fibula fracture distal to the syndesmosis with an intact syndesmosis—most isolated Weber A fractures are inherently stable and managed non-operatively. Surgical intervention is typically reserved for instances where the fracture is unstable due to associated injuries or significant displacement.
Non-Operative Indications
- Isolated Weber A fracture: No associated medial malleolus fracture, deltoid ligament rupture, or talar displacement.
- Stable ankle mortise: Confirmed by clinical examination and stress radiographs (e.g., gravity stress views, external rotation stress views) demonstrating no significant talar tilt (>2-3mm), no widening of the medial clear space (>4mm, or >1mm greater than contralateral side), and no tibiofibular diastasis.
- Minimally displaced fracture: Acceptable reduction of any fracture components, with minimal to no displacement of the fibular fracture.
Operative Indications
- Associated Medial Malleolus Fracture: If the medial malleolus is fractured and significantly displaced, or if its fracture pattern (e.g., vertical oblique) contributes to instability, operative fixation is warranted.
- Deltoid Ligament Rupture with Ankle Instability: In cases where the deltoid ligament is ruptured (evidenced by medial tenderness and medial clear space widening on stress radiographs) leading to talar shift or tilt, surgical stabilization is indicated. This transforms the fracture from a stable to an unstable injury.
- Open Fractures: All open ankle fractures require surgical debridement and stabilization.
- Irreducible Fractures: Fractures that cannot be anatomically reduced by closed means due to interposed soft tissues or significant displacement.
- Concomitant Talar or Pilon Fractures: While rare in pure Weber A patterns, any associated complex fractures that inherently destabilize the ankle.
Contraindications
Absolute contraindications to surgery are rare and usually relate to the patient's overall medical status rather than the fracture itself:
*
Unstable Medical Comorbidities:
Severe cardiac, pulmonary, or systemic conditions that preclude safe anesthesia and surgery.
*
Active Infection (local or systemic):
Infection in the operative field requires eradication prior to elective internal fixation.
*
Severe Peripheral Vascular Disease:
Compromised perfusion increasing the risk of wound complications and non-union.
*
Non-Ambulatory Status:
For patients with very limited functional demands, non-operative management might be preferred even for unstable fractures, after careful consideration of potential complications from non-treatment.
Summary of Operative vs. Non-Operative Indications
| Feature | Non-Operative Management | Operative Management |
|---|---|---|
| Fibular Fracture | Isolated, distal, transverse, non-displaced. | Displaced, comminuted (rare for Weber A), open. |
| Medial Malleolus | Intact or minimally displaced, non-articular fracture. | Displaced fracture, intra-articular step-off, rotational instability. |
| Deltoid Ligament | Intact or minor sprain, no medial clear space widening on stress. | Ruptured, leading to medial clear space widening (>4mm or >1mm compared to contralateral) and talar shift/tilt. |
| Syndesmosis | Intact (by definition of Weber A). | Intact (by definition of Weber A), but stress test confirms integrity. |
| Ankle Mortise Stability | Stable on clinical exam and stress radiographs. | Unstable on clinical exam and stress radiographs. |
| Soft Tissue Status | Closed injury, minimal swelling, no skin compromise. | Open fracture, severe soft tissue compromise (impending skin necrosis). |
| Patient Factors | Patient compliance with non-weight-bearing/immobilization. | Patients requiring earlier mobilization, young, active individuals. |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is essential for optimizing surgical outcomes and minimizing complications, even for seemingly straightforward ankle fractures.
Imaging
-
Standard Ankle Radiographs:
- Anteroposterior (AP) View: Assesses medial clear space, tibiofibular overlap/clearance, and fibular fracture location.
- Mortise View (15-20 degrees internal rotation): Provides an unobstructed view of the ankle mortise, allowing assessment of talar tilt, medial clear space, and syndesmotic integrity (tibiofibular clear space).
- Lateral View: Evaluates posterior malleolus fractures (though rare with Weber A), talar subluxation, and overall alignment.
-
Stress Radiographs:
Crucial for assessing ankle stability, especially if medial injury is suspected.
- Gravity Stress View: Performed with the patient supine and the leg hanging over the table edge, allowing gravity to apply an external rotation and slight valgus stress. Widening of the medial clear space suggests deltoid ligament injury and instability.
- External Rotation Stress View: Applied manually by an assistant with the foot in dorsiflexion. Similar to gravity stress, it can reveal medial clear space widening.
- A medial clear space >4mm or >1mm greater than the contralateral uninjured ankle is generally considered indicative of deltoid rupture and ankle instability.
- Computed Tomography (CT) Scan: Rarely indicated for isolated Weber A fractures. It may be considered for complex patterns, suspected concomitant talar or calcaneal fractures, significant comminution (uncommon in Weber A fibula), or pre-operative planning if precise intra-articular steps or fragment orientation is critical.
- Magnetic Resonance Imaging (MRI): Not routinely required. May be considered if specific ligamentous injuries (e.g., syndesmosis, deltoid) are strongly suspected but not confirmed by stress radiographs, and if this information would significantly alter management. Given Weber A definition, syndesmotic injury is excluded, but deltoid injury leading to instability is relevant.
Pre-Operative Preparation
- Timing of Surgery: If indicated, surgery should ideally be performed once soft tissue swelling has subsided (wrinkle sign) to minimize wound complications. Immediate surgical intervention is reserved for open fractures or irreducible dislocations.
- Anesthesia: General or regional anesthesia (e.g., spinal) can be utilized. A popliteal nerve block can be a useful adjunct for post-operative pain control.
- Patient Consent: Comprehensive discussion with the patient regarding the nature of the injury, operative procedure, potential risks (infection, nonunion, malunion, nerve injury, DVT/PE, hardware irritation, post-traumatic arthritis), expected recovery, and rehabilitation.
- Antibiotics: Prophylactic intravenous antibiotics (e.g., cefazolin) administered within 60 minutes of incision.
- Tourniquet: A thigh tourniquet is typically used to provide a bloodless surgical field, inflated to 100 mmHg above systolic blood pressure.
- Equipment: Availability of small fragment (3.5mm) plate and screw sets, K-wires, power drills, appropriate retractors, and fluoroscopy.
- Deep Venous Thrombosis (DVT) Prophylaxis: Routine DVT prophylaxis protocols, including mechanical and/or chemical methods, should be followed.
Patient Positioning
- Supine Position: The patient is positioned supine on the operating table.
- Ipsilateral Hip Bolster: A bolster or sandbag placed under the ipsilateral hip helps internally rotate the leg, presenting the lateral malleolus more directly to the surgeon and facilitating fluoroscopic imaging of the mortise.
- Fluoroscopy Access: The C-arm image intensifier should be positioned to allow easy access for AP, mortise, and lateral views of the ankle without significant repositioning of the patient or draped surgical field. This often involves placing the monitor on the contralateral side and the C-arm on the ipsilateral side of the operating table.
- Foot Position: The foot should be positioned on a sterile Mayo stand or a padded pillow to allow for comfortable surgical access and manipulation during reduction.
Detailed Surgical Approach / Technique
Surgical intervention for Weber A fractures is typically indicated when the fracture is associated with instability, usually due to a concomitant medial malleolus fracture or a deltoid ligament rupture that results in talar shift or tilt. The isolated, stable Weber A fracture is rarely operated on. The following describes a common approach for fixation of the fibula and addressing associated medial injuries.
1. Incision and Exposure
-
Lateral Malleolus (Fibular Fracture):
- A direct lateral incision centered over the distal fibula is generally employed. The length of the incision should be sufficient for adequate exposure, typically 5-7 cm.
- The incision is made parallel to the fibula, extending from approximately 5 cm proximal to the fibular tip distally to the level of the fibular fracture.
- Careful dissection through the subcutaneous tissue is performed. The superficial peroneal nerve should be identified and protected, as it typically lies anterior to the fibula in this region. Retract it anteriorly. The sural nerve is posterior and generally out of the field for a direct lateral approach.
- The periosteum is incised longitudinally along the fibula. Subperiosteal dissection is then carried out to expose the fracture fragments. Avoid excessive soft tissue stripping to preserve periosteal blood supply.
-
Medial Malleolus (if indicated):
- If there is a displaced medial malleolus fracture, a separate medial incision is made, centered over the medial malleolus.
- The incision is typically longitudinal, about 4-6 cm in length.
- Care is taken to protect the saphenous vein and nerve anteriorly and the posterior tibial tendon sheath posteriorly.
- Dissection is carried down through subcutaneous tissue to the periosteum of the medial malleolus.
2. Fracture Reduction
-
Fibular Fracture Reduction:
- The primary goal is anatomic reduction of the fibula length, rotation, and alignment.
- For a typical transverse Weber A fracture, direct manipulation with bone clamps (e.g., pointed reduction forceps, small Weber clamp) is usually sufficient. Restore fibular length by gentle distraction if impaction has occurred.
- Once anatomically reduced, provisional fixation is achieved with 1-2 small K-wires, ensuring they do not interfere with planned definitive screw or plate placement. Confirm reduction with fluoroscopy in AP, mortise, and lateral views.
-
Medial Malleolus Fracture Reduction (if present):
- Remove any interposed soft tissue from the fracture site (e.g., deltoid ligament fibers).
- Reduce the fracture anatomically. This often involves direct manipulation and impaction to restore the articular surface.
- Provisional fixation with K-wires or a small pointed reduction clamp is used. Confirm reduction with fluoroscopy.
3. Internal Fixation
-
Fibular Fracture Fixation:
- For a simple transverse Weber A fracture, two 3.5 mm cortical lag screws across the fracture plane can provide adequate fixation, provided the fragment is long enough. The screws are inserted from lateral to medial, ensuring good cortical purchase on both sides.
-
Alternatively, a
one-third tubular plate
or a small fragment
locking compression plate (LCP)
can be applied to the lateral aspect of the fibula. The plate acts as a neutralization plate, protecting lag screws from bending and rotational forces, particularly if there is some comminution or if strong stability is desired.
- Place a lag screw across the fracture first (if feasible), then apply the plate.
- Secure the plate with at least 2 screws proximally and 2 screws distally to the fracture, ensuring adequate bone purchase in each fragment.
-
Confirm final fibular fixation with fluoroscopy.

-
Medial Malleolus Fracture Fixation (if present):
- Typically, two partially threaded 4.0 mm cancellous screws or 3.5 mm cortical screws are used.
- The screws are inserted from the tip of the medial malleolus proximally, angling superiorly and slightly laterally towards the tibial shaft for optimal purchase. Alternatively, a posterior-to-anterior approach may be used if the fracture geometry dictates.
- Ensure the screws do not violate the ankle joint or damage the articular cartilage. Confirm position with fluoroscopy.
- For small, avulsed fragments, tension band wiring may be an option.
-
Deltoid Ligament Repair (if ruptured and unstable without a medial malleolus fracture):
- Direct repair of the deltoid ligament is rarely performed as an isolated procedure for a Weber A pattern unless significant instability persists after fibular fixation, and the ligament itself is amenable to repair. If the syndesmosis is truly intact, fibular fixation may be enough to indirectly stabilize the deltoid.
- If required, sutures (non-absorbable or strong absorbable) are passed through the ruptured ends of the deltoid ligament and secured to the medial malleolus periosteum or drilled bone tunnels. This is primarily aimed at restoring medial stability.
4. Syndesmotic Stability Assessment
- Although Weber A fractures are defined by an intact syndesmosis, it is imperative to confirm syndesmotic stability after fibular and any medial malleolus fixation, particularly if there was any concern pre-operatively or intra-operatively.
-
Perform an
external rotation stress test
under fluoroscopy.
- With the ankle in dorsiflexion, externally rotate the foot relative to the tibia.
- Observe for widening of the tibiofibular clear space (>6mm at 1cm above the plafond) or loss of tibiofibular overlap (>10mm on AP, >4mm on mortise) compared to the contralateral side.
- Given the definition of Weber A, this test should be negative. If positive, it suggests an atypical presentation or misclassification, and syndesmotic fixation (e.g., one or two 3.5 mm cortical screws or suture-button devices) would be indicated. However, this scenario is exceedingly rare for a true Weber A fracture.
5. Wound Closure
- Copiously irrigate the surgical sites with saline.
- Check for hemostasis.
- Close the periosteum and deep fascia with absorbable sutures.
- Close subcutaneous tissue and skin layers in a standard fashion.
- Apply a sterile dressing and a well-padded splint (e.g., posterior splint with stirrup) in neutral dorsiflexion.

Complications & Management
While Weber A fractures are generally considered stable and associated with fewer complications than higher-grade ankle fractures, surgical intervention or even non-operative management can still lead to various issues. Understanding these potential complications and their management is crucial for optimal patient care.
Common Complications and Management Strategies
| Complication | Incidence (Approximate Range) | Management / Salvage Strategy |
|---|---|---|
| Infection | 1-5% (lower for closed ORIF) |
*
Superficial:
Oral antibiotics, local wound care.
* Deep: Surgical debridement, IV antibiotics, implant removal (if stable union achieved or chronic infection). Consider a plastic surgery consult for wound coverage if severe. |
| Wound Healing Issues / Skin Necrosis | 5-10% | Local wound care, strict elevation, edema control. Debridement of necrotic tissue. Consider negative pressure wound therapy (NPWT) or skin grafting/flaps for large defects. |
| Nonunion / Malunion | <1-2% for Weber A fibula |
*
Nonunion:
Revision ORIF with bone grafting (autograft or allograft), plate/screw augmentation. Consider external fixation for high-risk patients.
* Malunion: Corrective osteotomy if symptomatic (e.g., impingement, altered gait, early arthritis). |
| Hardware Irritation / Prominence | 10-20% | Common complaint due to superficial hardware. Hardware removal after fracture union (typically 6-12 months post-op) if symptomatic. |
| Nerve Injury | <1% (superficial peroneal, sural, saphenous) | Most common is neuropraxia (transient). Observation for recovery. Neuropathic pain management. Surgical exploration and neurolysis for persistent, severe symptoms or documented nerve transection. |
| Deep Venous Thrombosis (DVT) / Pulmonary Embolism (PE) | DVT: 5-15% (lower limb trauma), PE: <1% | DVT prophylaxis (pharmacologic/mechanical). Diagnosis via duplex ultrasound. Treatment with anticoagulation. Surgical thrombectomy for massive PE. |
| Post-Traumatic Arthritis (PTA) | 5-15% (can be higher for unstable fractures) | Long-term complication. Management involves activity modification, NSAIDs, intra-articular injections (corticosteroids, hyaluronic acid). Advanced cases may require ankle arthrodesis or total ankle arthroplasty. Rare in truly stable, anatomically reduced Weber A fractures. |
| Stiffness / Limited Range of Motion (ROM) | 10-20% | Early mobilization protocols. Aggressive physical therapy, including stretching and strengthening exercises. Rarely, arthroscopic or open arthrolysis for severe capsular contracture or adhesions. |
| Complex Regional Pain Syndrome (CRPS) | 1-5% | Multimodal approach: physical therapy, pain management (nerve blocks, sympathetic blocks, medications), psychological support. Early recognition is key. |
| Medial Clear Space Widening (Post-ORIF) | <1% (if syndesmosis assessed and stable) | Re-evaluation of stability, especially syndesmosis. Revision surgery for syndesmotic fixation if initially overlooked or failed. Re-assessment of medial fixation. |
Discussion of Key Complications
- Soft Tissue Complications: The ankle is prone to soft tissue issues due to its superficial bony anatomy and limited soft tissue envelope. Edema management, judicious incision placement, and atraumatic surgical technique are paramount. Delayed wound healing can increase the risk of infection.
- Post-Traumatic Arthritis: While Weber A fractures are generally stable, any unaddressed instability or articular incongruity, particularly on the medial side, can lead to accelerated degenerative changes. Even subtle malreduction of the fibula, if it impacts the overall mortise congruity, can contribute. Careful anatomical reduction and stable fixation are crucial preventative measures.
- Hardware-Related Issues: The lateral malleolus is subcutaneous, making hardware prominence a common patient complaint, often necessitating elective removal of hardware once union is solid. This is usually performed 6-12 months post-operatively.
- Nonunion/Malunion: Though rare for simple Weber A fractures, nonunion can occur with inadequate fixation, severe comminution (uncommon in Weber A), or compromised vascularity. Malunion, particularly rotational malalignment of the fibula, can subtly alter ankle biomechanics and lead to symptoms.
- Nerve Injuries: The superficial peroneal nerve is at risk during lateral approaches, and the saphenous nerve and vein during medial approaches. Careful dissection, identification, and retraction are necessary.
Thorough pre-operative planning, meticulous surgical technique, and appropriate post-operative rehabilitation are the cornerstones of minimizing complication rates in Weber A ankle fracture management. Regular follow-up and patient education regarding potential warning signs are also critical.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation for Weber A ankle fractures, especially those that required surgical stabilization due to associated instability, is critical for restoring function, preventing stiffness, and minimizing long-term complications. Protocols vary depending on the specific fixation achieved, the stability of the ankle mortise, and the patient's individual healing capacity and activity level.
Phase 1: Immobilization and Protection (Weeks 0-6)
The primary goals are wound healing, pain and edema control, and protection of the surgical repair.
*
Immobilization:
* Initially, a well-padded posterior splint and stirrup or a rigid plaster cast (e.g., short leg cast) is applied in a neutral position for comfort and protection.
* Once swelling subsides (typically 1-2 weeks), this may be converted to a functional walking boot (CAM walker) or a removable cast.
*
Weight-Bearing Status:
*
Non-Weight-Bearing (NWB):
The affected extremity remains NWB using crutches or a knee scooter. This is crucial to protect the healing bone and soft tissues.
*
Note for stable non-operative Weber A:
For truly isolated, stable, non-displaced Weber A fractures managed non-operatively, early protected weight-bearing (e.g., in a walking boot) may be initiated sooner, sometimes as early as 2-3 weeks, based on stability and comfort. However, for operatively treated cases, NWB is the standard.
*
Pain and Edema Management:
* Elevation of the limb above heart level (especially during the first 48-72 hours post-op).
* Ice application (indirectly over dressings).
* Analgesics as prescribed.
*
Early Motion (Upper Extremity/Contralateral Lower Extremity):
* Maintain strength and conditioning of the unaffected limbs.
*
Initiation of Gentle Range of Motion (ROM) for Ankle (Non-Operative or Secure Fixation):
* For very stable fixation, sometimes gentle active plantarflexion/dorsiflexion can begin as early as 2-3 weeks post-op, within the boot, to prevent stiffness. This is at the surgeon's discretion and based on fixation strength. Inversion/eversion is typically avoided or severely restricted initially.
*
Wound Care:
Daily inspection of dressing for discharge. Suture removal typically at 10-14 days post-op.
Phase 2: Progressive Weight-Bearing and Controlled Motion (Weeks 6-12)
The goals include initiating protected weight-bearing, restoring pain-free ankle motion, and beginning muscle strengthening.
*
Radiographic Assessment:
At 6 weeks post-op, radiographs are taken to assess healing and ensure maintenance of reduction.
*
Weight-Bearing Progression:
* If radiographs show adequate healing and the ankle is clinically stable, gradual progression to
Partial Weight-Bearing (PWB)
in the walking boot is initiated.
* Progress from partial (25-50%) to full weight-bearing as tolerated over 2-4 weeks, as pain allows.
*
Ankle Range of Motion:
* Active and passive ROM exercises are increased, focusing on dorsiflexion, plantarflexion, inversion, and eversion.
* Gentle stretching exercises.
*
Strengthening:
* Isometric exercises for ankle musculature (dorsiflexors, plantarflexors, invertors, evertors) within pain limits.
* Theraband exercises.
*
Gait Training:
* Emphasis on normal gait mechanics with appropriate assistive devices (crutches, cane).
*
Transition from Boot:
Depending on clinical and radiographic healing, the walking boot may be discontinued around 10-12 weeks, transitioning to a supportive lace-up ankle brace or stable athletic shoe.
Phase 3: Advanced Strengthening and Proprioception (Weeks 12-24)
The goals are to restore full strength, endurance, proprioception, and prepare for return to activity.
*
Full Weight-Bearing:
Should be achieved by the beginning of this phase.
*
Intensive Strengthening:
* Progressive resistive exercises targeting all ankle muscle groups.
* Calf raises (bilateral, then unilateral).
* Stair climbing.
* Resistance training with weights or machines.
*
Proprioception and Balance Training:
* Single-leg standing, wobble board, balance disc exercises.
* Dynamic balance activities.
*
Endurance Training:
Cycling, swimming, elliptical.
*
Sport-Specific Training (if applicable):
* Agility drills, plyometrics, and gradual return to running/jumping activities, usually beginning around 4-6 months post-op, depending on the severity of the initial injury and the patient's sport.
Phase 4: Return to Activity (Months 6+)
- Return to full unrestricted activities and sports as tolerated, typically 6 months or longer, provided full strength, ROM, and stability are achieved.
- Continued use of an ankle brace may be recommended for certain high-impact sports.
- Patients should be educated on the potential for residual stiffness, occasional swelling, and the risk of post-traumatic arthritis.
General Considerations
- Individualization: Rehabilitation protocols must be tailored to the individual patient, their progress, and specific surgical findings.
- Communication: Close communication between the surgeon, physical therapist, and patient is essential.
- Compliance: Patient compliance with the rehabilitation program significantly impacts the final outcome.
- Pain as a Guide: Activities should generally be pain-free. Any increase in pain or swelling should prompt a reassessment.
Summary of Key Literature / Guidelines
The literature concerning Weber A ankle fractures consistently supports a generally benign course, with non-operative management being the cornerstone for the vast majority of cases. However, discerning true stability remains paramount.
-
AO/Danis-Weber Classification: The AO Foundation's comprehensive classification system for ankle fractures, based on the level of the fibular fracture relative to the syndesmosis, dictates much of the modern treatment philosophy. Weber A fractures, by definition, involve a fibular fracture distal to the syndesmosis, implying an intact syndesmosis and often inherent stability.
- Danis, R. (1949). Théorie et pratique de l'ostéosynthèse. While not specifically focused on Weber A, Danis's work laid the groundwork for classifying malleolar fractures, which was later expanded by Weber.
- Weber, B.G. (1972). Die Verletzungen des oberen Sprunggelenkes. This work popularized the classification system that bears his name, emphasizing the importance of syndesmotic integrity.
-
Lauge-Hansen Classification: While more complex, the Lauge-Hansen system (e.g., Supination-Adduction type) describes the mechanism of injury and predictable patterns of bone and ligamentous damage. Weber A fractures correspond to the SA-I and SA-II types, characterized by a transverse fibular fracture below the joint line (SA-I) and potentially an associated medial malleolus fracture (SA-II). The integrity of the syndesmosis is a defining feature of these types.
- Lauge-Hansen, N. (1950). "Fractures of the Ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations." Archives of Surgery , 60(5), 990-1011. This seminal work detailed the mechanism-based classification.
-
Stability Assessment & Stress Radiographs: Numerous studies underscore the critical role of stress radiographs (gravity stress, external rotation stress) in evaluating ankle mortise stability. Widening of the medial clear space (typically >4mm or >1mm greater than the contralateral side) under stress is a widely accepted criterion for deltoid ligament rupture and associated ankle instability, warranting operative intervention regardless of the Weber A fibular fracture pattern.
- Michelson, J. D., et al. (1997). "The value of the medial clear space in assessing ankle mortise stability." Foot & Ankle International , 18(1), 1-6. This article highlights the importance of the medial clear space measurement.
- Tornetta, P. (2010). "Assessment of Ankle Fractures: Mortise Views, Stress Views, and CT Scans." Instructional Course Lectures , 59, 395-402. A review emphasizing diagnostic imaging for ankle fractures.
-
Non-operative Management Efficacy: The literature overwhelmingly supports non-operative management for stable Weber A fractures. This typically involves a short period of immobilization (e.g., walking boot for 4-6 weeks) followed by early mobilization and protected weight-bearing. Outcomes are generally excellent with low rates of complications or long-term disability.
- Egbers, H. J., & van Hellemondt, G. G. (2012). "Non-operative treatment of stable lateral malleolar fractures: a systematic review." International Orthopaedics , 36(5), 1051-1057. While focusing on lateral malleolus fractures generally, it supports non-operative management for stable variants.
- Kannus, P., et al. (1991). "Weight-bearing in rehabilitation of ankle fractures." Orthopedics , 14(3), 329-331. Discusses the safety and benefits of early weight-bearing for stable ankle fractures.
-
Indications for Operative Management: Surgical fixation of Weber A fractures is primarily indicated when instability is present due to associated injuries (displaced medial malleolus fracture, deltoid rupture with talar shift) or for open fractures. The goal of surgery is anatomic reduction and stable fixation of all components contributing to instability, thus restoring the ankle mortise congruity.
- Bostman, O., et al. (1987). "Complications of malleolar fractures: an 8-year follow-up of 869 patients." Injury , 18(3), 163-165. This study, among others, highlights complications with unstable fractures and underscores the importance of stable fixation.
- Brunner, L. C., et al. (2007). "Medial-side instability in ankle fractures." Journal of Bone & Joint Surgery - American Volume , 89(Suppl 1), 60-66. Discusses the indications for addressing medial pathology.
In summary, current guidelines emphasize meticulous clinical and radiographic assessment, including stress views, to confirm the stability of a Weber A ankle fracture. If stable, non-operative management with early functional rehabilitation is the preferred and highly successful treatment. Operative intervention is reserved for the rare instances where a Weber A pattern presents with frank instability, typically due to associated medial pathology. The principles of anatomic reduction and stable internal fixation, as dictated by the AO principles, guide surgical management when indicated.
Clinical & Radiographic Imaging

