Comprehensive Introduction and Patho-Epidemiology
A profound and exhaustive understanding of spinal nerve anatomy and its peripheral extensions represents the absolute cornerstone of orthopaedic neurology, complex spine surgery, and peripheral nerve reconstruction. Each segmental spinal nerve acts as the critical, highly organized junction between the central nervous system (CNS) and the peripheral nervous system (PNS). Formed at or in immediate proximity to its respective intervertebral foramen, the mixed spinal nerve is generated by the precise anatomical union of its dorsal (sensory) root and its ventral (motor) root. The mastery of this transition zone is non-negotiable for the operating orthopaedic surgeon, as it dictates the surgical approach, the interpretation of electrodiagnostic studies, and the ultimate prognosis following traumatic or iatrogenic nerve injury.
The patho-epidemiology of peripheral nerve injuries reveals a significant burden within the realm of orthopaedic trauma. Major peripheral nerve injuries complicate approximately 2% to 3% of all major extremity trauma, with a markedly higher incidence in high-energy mechanisms such as motorcycle collisions, industrial crush injuries, and military ballistic trauma. In the lower extremity, sciatic nerve injuries are intimately associated with posterior fracture-dislocations of the hip and complex acetabular fractures, occurring in up to 10% to 15% of these specific trauma cohorts. Furthermore, iatrogenic injuries remain a persistent challenge; the common peroneal nerve is uniquely vulnerable during proximal fibular osteotomies, lateral knee arthrotomies, and total knee arthroplasty in the setting of severe valgus deformities. Understanding the precise epidemiological distribution of these injuries allows the surgeon to maintain a high index of suspicion during the initial trauma bay evaluation.
At the cellular level, the pathophysiology of nerve injury is dictated by the severity of the mechanical insult, classically categorized by Seddon (Neuropraxia, Axonotmesis, Neurotmesis) and further stratified by Sunderland into five distinct degrees of injury. Following a complete transection (Sunderland Grade V), the distal axonal segment undergoes Wallerian degeneration, a complex biological cascade characterized by the disintegration of the axoplasm and myelin sheath, followed by macrophage-mediated phagocytosis. Concurrently, the proximal neuronal cell body undergoes chromatolysis, upregulating the synthesis of cytoskeletal proteins required for axonal regeneration. In the distal stump, Schwann cells proliferate and align longitudinally to form the Bands of Büngner, which serve as biological conduits for regenerating axonal growth cones.
The biological clock governing nerve regeneration is unforgiving, primarily due to the progressive, irreversible fibrosis of the motor endplates within the target musculature. While sensory receptors can remain viable for years, denervated skeletal muscle undergoes profound atrophy, with the critical limit of delay for successful motor reinnervation generally accepted as 12 to 18 months. Because regenerating axons advance at a highly predictable rate of approximately 1 mm per day (or 1 inch per month), the anatomical distance between the site of injury and the target motor endplate is the single most critical prognostic factor. Proximal injuries, such as high sciatic nerve transections, carry a inherently guarded prognosis for distal motor recovery (e.g., intrinsic foot musculature) simply because the regenerating axons cannot traverse the required anatomical distance before irreversible motor endplate fibrosis occurs.
Detailed Surgical Anatomy and Biomechanics
Gross Anatomy and Functional Organization
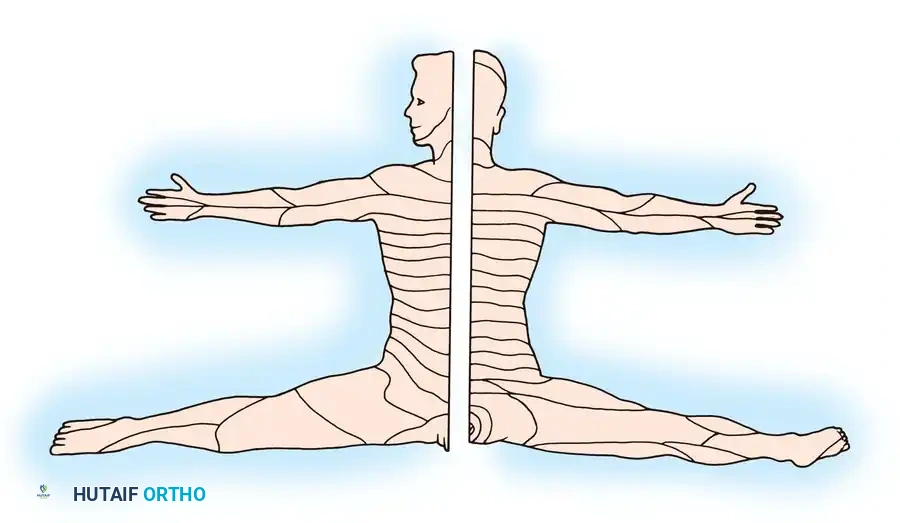
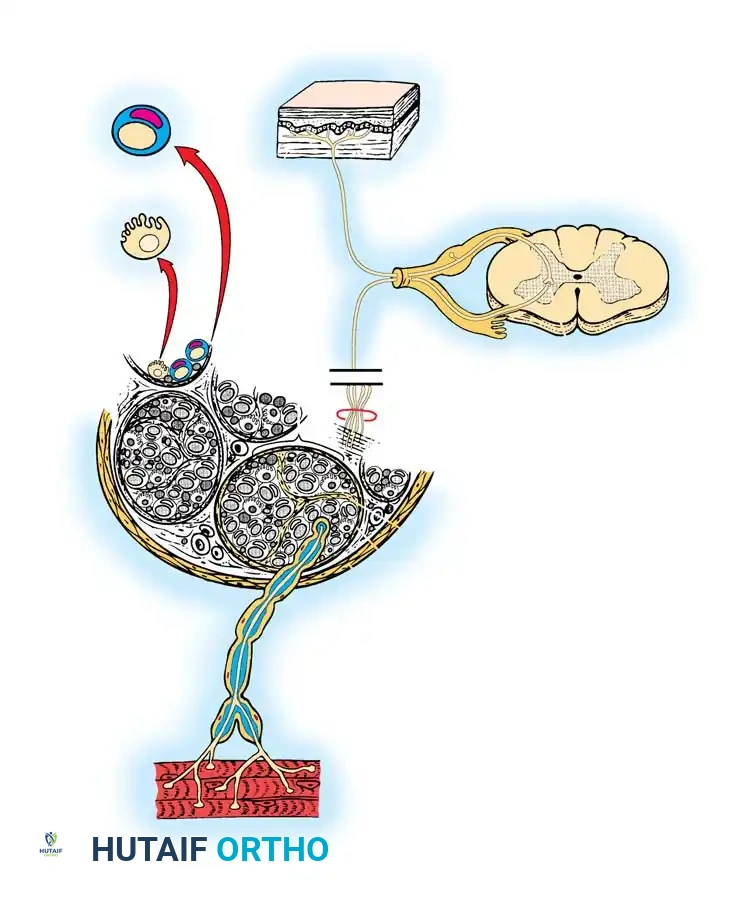
In the human anatomical axis, a total of 31 pairs of mixed spinal nerves exit their respective intervertebral foramina to innervate the homolateral trunk and extremities. This highly conserved metameric distribution is categorized into 8 Cervical (C1–C8), 12 Thoracic (T1–T12), 5 Lumbar (L1–L5), 5 Sacral (S1–S5), and 1 Coccygeal (Co1) segment. A typical mixed spinal nerve is a highly organized neurovascular conduit comprising three distinct functional components: motor (somatic efferent), sensory (somatic afferent), and sympathetic (autonomic).
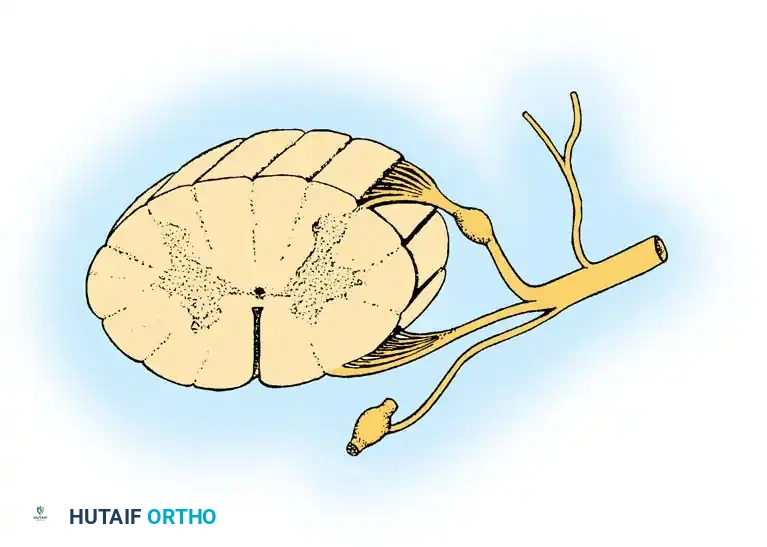
The motor components arise directly from the heavily myelinated alpha motor neurons situated within the anterior horn of the spinal cord gray matter. These fibers traverse the anterolateral sulcus via several rootlets to form the ventral root, dictating the myotomal function of skeletal muscles. Conversely, the sensory fibers originate from peripheral receptors and project centrally. The cell bodies for these pseudounipolar neurons are housed within the dorsal root ganglia (DRG), which typically reside within the neural foramen. Central projections follow distinct, highly segregated pathways: proprioceptive and fine tactile fibers ascend ipsilaterally in the dorsal columns (gracile and cuneate fasciculi), whereas pain and temperature fibers synapse in the substantia gelatinosa, cross the midline via the anterior white commissure, and ascend in the contralateral spinothalamic tracts.
The sympathetic component introduces further anatomical complexity. Originating from the intermediolateral cell column (T1–L2), preganglionic efferent fibers exit via the motor roots and emerge as white rami communicantes. They project to the paravertebral sympathetic ganglia, from which unmyelinated postganglionic fibers return to all 31 mixed spinal nerves via gray rami communicantes. This provides essential segmentally distributed sudomotor, vasomotor, and pilomotor innervation. Upon exiting the foramen, the mixed spinal nerve promptly bifurcates. The posterior primary rami supply the paraspinal musculature and overlying dorsal skin, while the massive anterior primary rami proceed to form the intricate cervical, brachial, lumbar, and lumbosacral plexuses, abandoning primitive myomeric patterns to accommodate the complex biomechanical demands of the appendicular skeleton.
Microscopic Architecture and Intraneural Topography
The surgical repair of peripheral nerves demands an uncompromising, rigorous understanding of their microscopic architecture and internal topography. Each peripheral nerve fiber (axon) is an uninterrupted extension of a neuron and is classified as either myelinated or unmyelinated, with sensory and motor nerves typically containing both in a ratio approximating 4:1. The functional capacity of these axons is heavily dependent on their supporting glial cells.
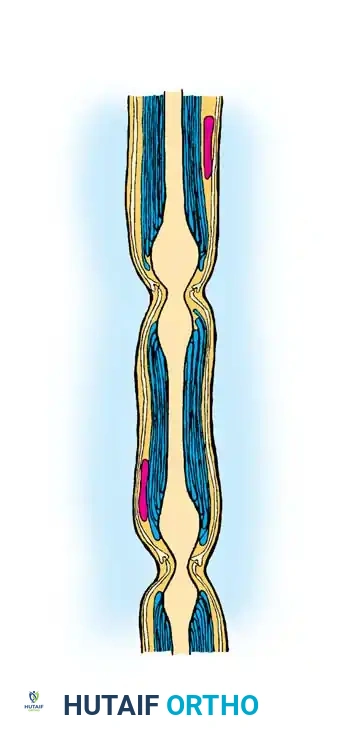
In heavily myelinated fibers, a single Schwann cell rotates concentrically to form a multilaminated myelin sheath around a single axon. The specific segment of the axon enclosed by one Schwann cell is termed the internode, which ranges from 0.1 to 1.8 mm in length. The myelin-free gap between adjacent Schwann cells, known as the Node of Ranvier, is rich in voltage-gated sodium channels and facilitates rapid, saltatory action potential conduction. In unmyelinated fibers, a single Schwann cell may envelop several axons, providing metabolic support without the rapid conduction benefits of saltatory transmission.
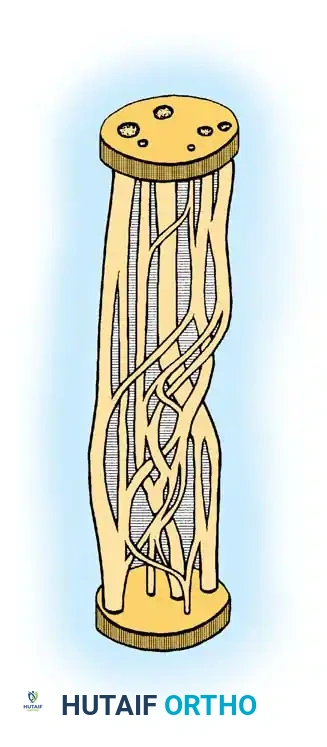
The structural integrity and biomechanical resilience of a peripheral nerve are maintained by three distinct, highly specialized connective tissue layers. The endoneurium is a delicate, continuous veil of collagenous tissue surrounding individual axons and their associated Schwann cells. The perineurium is a dense, metabolically active, lamellated layer that surrounds a group of axons to form a fascicle (or funiculus). The perineurium is biomechanically critical; it provides the primary tensile strength of the nerve and maintains the highly restrictive blood-nerve barrier. Finally, the epineurium is the outermost layer of loose, areolar connective tissue that encases the entire group of fascicles, forming the macroscopic peripheral nerve and cushioning the internal fascicles against external compressive and sheer forces.
The vascular supply to this complex structure, the vasa nervorum, is equally intricate. Blood enters through the mesoneurium, a suspensory ligament extending from the epineurium to surrounding fascial beds. This extrinsic system feeds a highly anastomotic intrinsic longitudinal network within the epineurium, perineurium, and endoneurium. Biomechanically, the undulating course of the fascicles (the Bands of Fontana) allows the nerve to stretch approximately 8% to 15% of its resting length before structural failure occurs. However, surgical over-mobilization or aggressive circumferential stripping of the epineurium can easily disrupt the extrinsic vasa nervorum, leading to profound ischemic fibrosis and catastrophic failure of nerve regeneration.
Exhaustive Indications and Contraindications
The decision-making algorithm for surgical intervention in peripheral nerve injuries is heavily dictated by the mechanism of injury, the temporal relationship to the traumatic event, and the specific anatomical level of the lesion. Absolute indications for immediate surgical exploration (within 72 hours) include clean, sharp lacerations (e.g., knife wounds, glass lacerations) where the nerve ends are visible or highly suspected to be transected, and nerve injuries associated with concomitant vascular injuries requiring immediate repair. In these scenarios, primary end-to-end neurorrhaphy yields the most superior functional outcomes, as the anatomical topography is preserved and Wallerian degeneration has not yet caused massive retraction of the nerve stumps.
Delayed exploration and reconstruction (typically between 3 to 6 months post-injury) is indicated for blunt trauma, high-energy stretch injuries, and severe crush injuries. In these mechanisms, the initial zone of injury is highly unpredictable, and immediate repair is contraindicated due to the inability to distinguish viable fascicles from irreversibly damaged tissue. The surgeon must allow time for the true zone of injury to demarcate. If serial clinical examinations and electrodiagnostic studies (EMG/NCS) at 3 months show absolutely no evidence of nascent motor unit potentials or clinical reinnervation, surgical exploration with intraoperative nerve action potential (NAP) monitoring is strongly indicated. If no NAP is conducted across the neuroma-in-continuity, resection and autologous cable grafting are mandatory.
Contraindications to peripheral nerve repair are equally critical to understand to avoid subjecting the patient to futile surgical morbidity. Absolute contraindications include a prolonged delay in presentation (typically greater than 18 to 24 months for motor nerve injuries), as the target motor endplates will have undergone irreversible fibrosis, rendering any proximal nerve repair biologically useless. In such cases, the patient is better served by regional tendon transfers or arthrodesis. Severe physiological instability, active deep soft tissue infection at the planned surgical site, and massive segmental nerve loss where autologous donor graft material is insufficient also represent significant contraindications to primary repair or grafting.
| Clinical Scenario | Surgical Indication | Contraindication / Alternative |
|---|---|---|
| Sharp Laceration (e.g., glass) | Immediate primary exploration and end-to-end epineurial repair (within 72 hours). | Do not delay; waiting allows for stump retraction and topographic mismatch. |
| High-Energy Stretch/Crush | Delayed exploration at 3-6 months if no clinical/EMG recovery is evident. | Immediate repair is contraindicated due to indistinguishable zone of injury. |
| Neuroma-in-Continuity (NAP negative) | Resection of neuroma back to healthy fascicles and autologous cable grafting. | Leaving the neuroma intact is contraindicated; it will block axonal regeneration. |
| Late Presentation (>18-24 months) | Tendon transfers, free functional muscle transfers, or arthrodesis. | Proximal nerve repair is absolutely contraindicated due to motor endplate fibrosis. |
| Massive Segmental Defect (>10 cm) | Vascularized nerve grafts or targeted muscle reinnervation (TMR). | Standard non-vascularized cable grafts may fail due to central core ischemia. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the absolute prerequisite for successful peripheral nerve surgery. The clinical examination must be meticulously documented, establishing a precise baseline. Motor function is graded using the Medical Research Council (MRC) scale (M0 to M5), and sensory mapping is performed using two-point discrimination and Semmes-Weinstein monofilaments. The exact location of the advancing Tinel's sign must be marked on the patient's skin with a permanent marker at each clinic visit, providing a macroscopic clinical indicator of the leading edge of regenerating axonal growth cones.
Electrodiagnostic studies and advanced neuroimaging are critical adjuncts. Electromyography (EMG) and Nerve Conduction Studies (NCS) should not be performed earlier than 3 to 4 weeks post-injury, as Wallerian degeneration must be complete for the studies to accurately reflect the extent of denervation (e.g., the presence of fibrillation potentials and positive sharp waves). High-resolution Magnetic Resonance Neurography (MRN) and high-frequency ultrasound have revolutionized pre-operative templating. These modalities allow the surgeon to visualize neuromas, measure the exact length of the anatomical gap, and assess the cross-sectional area of the injured nerve, facilitating precise calculation of the required length and number of autologous nerve grafts (e.g., sural nerve) needed for the reconstruction.
Patient positioning and operating room setup must be optimized for both the primary exposure and the potential donor graft harvest sites. For sciatic and tibial nerve explorations, the patient is positioned prone on a radiolucent Jackson table with all bony prominences meticulously padded. The knees are slightly flexed to relax the posterior neurovascular structures. For common peroneal nerve surgery, a lateral decubitus or a supine position with a large bump under the ipsilateral hip is utilized, allowing free access to the posterolateral corner of the knee and the entire fibular length.
Tourniquet use in peripheral nerve surgery requires judicious management. While a bloodless field is essential for identifying microscopic fascicular architecture, standard exsanguination with an Esmarch bandage can empty the vasa nervorum, making the critical intrinsic epineurial vessels difficult to identify during alignment. Many master nerve surgeons prefer to elevate the limb for 3 minutes without Esmarch exsanguination before tourniquet inflation, which traps a small amount of venous blood within the epineurial vessels, greatly facilitating precise rotational alignment during neurorrhaphy. Furthermore, the tourniquet must be deflated prior to final closure to ensure absolute hemostasis, as a postoperative hematoma can cause devastating compressive neuropathy.
Step-by-Step Surgical Approach and Fixation Technique
Sciatic Nerve Exploration and Excision of Neuroma
The sciatic nerve (L4-S3) is the largest peripheral nerve in the human body and requires a massive, extensile approach for adequate mobilization. The patient is positioned prone. The surgical incision is curvilinear, beginning at the posterior superior iliac spine (PSIS), extending distally and laterally over the greater trochanter, and then curving gracefully down the posterior midline of the thigh. The deep fascia is incised, and the gluteus maximus is either split longitudinally in line with its coarse muscle fibers or, for more proximal exposures, reflected medially by detaching its insertion from the gluteal tuberosity and iliotibial tract.
The nerve is identified as it exits the greater sciatic foramen, typically emerging inferior to the piriformis muscle. The surgeon must be acutely aware of anatomical variants, such as the peroneal division piercing or exiting superior to the piriformis. External neurolysis is performed using loop magnification or an operating microscope, meticulously freeing the nerve from surrounding post-traumatic scar tissue. If a neuroma-in-continuity is encountered, intraoperative nerve stimulation and recording of Nerve Action Potentials (NAPs) are performed. If no NAP is conducted across the lesion, the neuroma is serially resected using a fresh diamond knife or razor blade until healthy, pouting fascicles with a "mushrooming" appearance are identified both proximally and distally.
Common Peroneal Nerve Decompression and Sural Cable Grafting
The common peroneal nerve is uniquely vulnerable to compression, traction, and laceration as it winds around the fibular neck, leading to the devastating clinical presentation of a "foot drop." The surgical approach utilizes a longitudinal lateral incision centered over the biceps femoris tendon, extending distally across the fibular neck and into the anterior compartment of the leg. The deep fascia is incised, and the nerve is identified medial to the biceps tendon.
The most critical step in this approach is the complete decompression of the nerve as it dives beneath the sharp, fibrous arch of the peroneus longus muscle. The superficial head of the peroneus longus must be divided to expose the bifurcation of the common peroneal nerve into its deep and superficial branches. If a segmental defect exists following neuroma resection, autologous sural nerve cable grafting is the gold standard. The sural nerve is harvested from the posterior calf, reversed to prevent axonal dispersion down sensory side branches, and cut into appropriate lengths. The cable grafts are then sutured between the proximal and distal stumps using 8-0 or 9-0 non-absorbable monofilament sutures under the operating microscope, ensuring a completely tension-free group fascicular repair augmented with fibrin glue.
Tibial Nerve Interventions in the Popliteal Fossa
The tibial nerve provides vital motor innervation to the deep and superficial posterior compartments of the leg, as well as critical sensory innervation to the plantar aspect of the foot. Exploring the tibial nerve in the popliteal fossa requires an S-shaped or lazy-Z incision across the popliteal crease to prevent the formation of highly morbid postoperative flexion contractures. The deep popliteal fascia is incised, and the nerve is reliably identified superficial and slightly lateral to the popliteal vein and artery.
When addressing gaps in the tibial nerve, the surgeon can often achieve primary repair without grafting by utilizing extensive proximal and distal mobilization. The nerve can be mobilized proximally deep to the hamstring bellies and distally by dividing the fibrous soleus arch. Furthermore, flexing the knee to 90 degrees can close gaps of up to 3 to 4 centimeters. If primary epineurial repair is achieved using this joint positioning technique, the repair is secured with 8-0 nylon, meticulously aligning the superficial epineurial vasculature to ensure correct rotational topography. Postoperatively, the limb must be rigidly immobilized in flexion to protect the neurorrhaphy.
Complications, Incidence Rates, and Salvage Management
Despite meticulous microsurgical technique, peripheral nerve surgery is fraught with potential complications, primarily due to the unpredictable nature of axonal regeneration and the dense fibrotic response of surrounding traumatized tissues. The most common complication is the failure of functional regeneration, which occurs in up to 30% to 40% of proximal nerve repairs (e.g., high sciatic lesions). This failure is typically secondary to the inability of regenerating axons to reach the distal motor endplates before irreversible muscle fibrosis occurs, or due to severe topographic mismatch at the repair site.
A particularly devastating complication is the development of a painful neuroma or Complex Regional Pain Syndrome (CRPS) Type II, historically termed causalgia. This occurs in approximately 5% to 10% of major nerve injuries, most frequently involving the sciatic or tibial nerves. CRPS Type II is characterized by severe, burning neuropathic pain, allodynia, hyperpathia, and profound autonomic dysregulation (sudomotor and vasomotor changes). Management is incredibly challenging and requires a multidisciplinary approach involving aggressive pharmacological management (gabapentinoids, tricyclic antidepressants), serial sympathetic ganglion blocks, and in refractory cases, the implantation of spinal cord stimulators or peripheral nerve stimulators.
When nerve repair definitively fails, or when the patient presents beyond the critical limit of delay, salvage management relies heavily on regional tendon transfers to restore functional biomechanics. For irreversible common peroneal nerve palsy (permanent foot drop), the gold standard salvage procedure is the transfer of the Posterior Tibial Tendon (PTT). The PTT is harvested from its insertion on the navicular, routed through a large window created in the interosseous membrane, and inserted into the middle cuneiform (or split to the tibialis anterior and peroneus brevis in a "Bridle" configuration) to restore balanced, active ankle dorsiflexion. For tibial nerve failure, salvage is more complex, often requiring specialized orthoses (e.g., rigid ankle-foot orthoses) and vigilant, lifelong podiatric care to prevent neuropathic plantar ulcerations and subsequent osteomyelitis.
| Complication | Estimated Incidence | Pathophysiology | Salvage Management / Treatment |
|---|---|---|---|
| Failure of Motor Regeneration | 30% - 40% (Proximal lesions) | Motor endplate fibrosis; topographic mismatch; excessive gap distance. | Tendon transfers (e.g., PTT for foot drop); Arthrodesis; AFO bracing. |
| Painful Neuroma | 10% - 15% | Disorganized axonal sprouting trapped in dense scar tissue. | Neuroma excision and burying stump in deep muscle or bone; Targeted Muscle Reinnervation (TMR). |
| CRPS Type II (Causalgia) | 5% - 10% | Abnormal sympathetic-somatic coupling; central nervous system sensitization. | Sympathetic blocks; Gabapentinoids; Physical therapy; Spinal Cord Stimulation (SCS). |
| Neurorrhaphy Dehiscence | < 5% | Excessive tension at the repair site; premature aggressive postoperative stretching. | Re-exploration and autologous cable grafting; strict adherence to tension-free principles. |
| Neuropathic Ulceration | 15% - 20% (Tibial nerve injuries) | Loss of protective plantar sensation combined with altered foot biomechanics. | Total contact casting; custom orthotics; meticulous daily skin inspection; surgical offloading. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following peripheral nerve repair or autologous grafting is a highly structured, phased process designed to protect the fragile microscopic neurorrhaphy while simultaneously preventing joint contractures and maximizing ultimate functional recovery. Phase I (0 to 4 weeks postoperatively) is the strictly protective phase. The affected limb is rigidly immobilized in a custom orthosis, cast, or splint in a position that completely eliminates tension on the repair site. For example, following a tibial nerve repair achieved with knee flexion, the knee is locked in 90 degrees of flexion. During this phase, absolute immobilization of the involved joints is mandatory, though adjacent un-involved joints must be aggressively mobilized to prevent regional stiffness.
Phase II (4 to 8 weeks postoperatively) marks the initiation of gradual mobilization. The primary objective is to slowly stretch the surrounding soft tissues without
