Orthopedic Anatomy MCQs (Set 1): Spine, Upper & Lower Limb | AAOS ABOS 2002 Review

Key Takeaway
This high-yield question set (Set 1 from 2002) for AAOS/ABOS exams covers essential orthopedic anatomy. It features challenging MCQs on spinal column structures, upper limb bones and muscles, and lower limb musculature, crucial for board preparation and clinical understanding.
Orthopedic Anatomy MCQs (Set 1): Spine, Upper & Lower Limb | AAOS ABOS 2002 Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
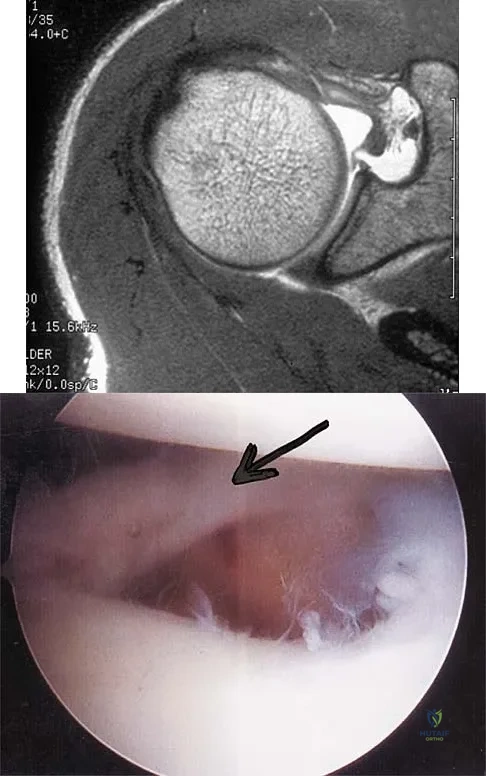
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?
Explanation
Question 2
What muscle attaches to the site shown by the arrow in Figure 2?

Explanation
Question 3
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?

Explanation
Question 4
Posterior sternoclavicular dislocations are most commonly associated with which of the following complications?

Explanation
Question 5
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?

Explanation
Question 6
A patient with an acromioclavicular dislocation has a very prominent distal clavicle. Examination reveals that the deformity increases rather than reduces with an isometric shoulder shrug. Which of the following structures is most likely intact?

Explanation
Question 7
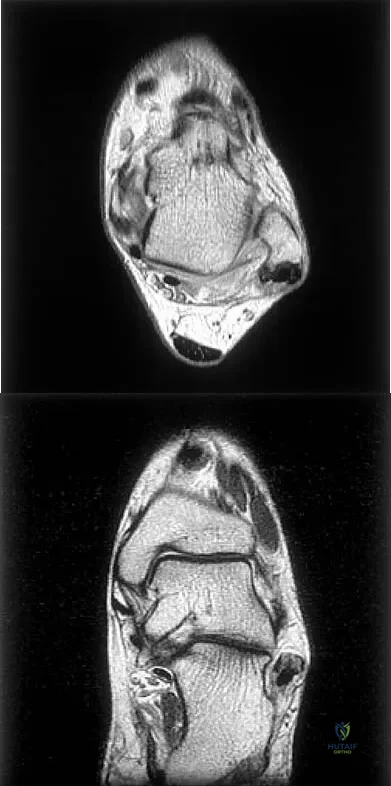
Figures 5a and 5b show axial and coronal MRI images of the left ankle of a patient with lateral ankle pain. What is the most likely diagnosis?
Explanation
Question 8
Which of the following anatomic structures is often difficult to visualize during elbow arthroscopy?

Explanation
Question 9
The quadrilateral space in the shoulder contains which of the following structures?

Explanation
Question 10
Based on the MRI scan shown in Figure 6, the abnormal signal is seen in what carpal bone?

Explanation
Question 11
The recurrent motor branch of the median nerve innervates which of the following muscles?

Explanation
Question 12
Which of the following nerves innervates the muscle that originates from the middle third of the dorsal surface of the lateral border of the scapula, as shown in Figure 7?

Explanation
Question 13
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?

Explanation
Question 14
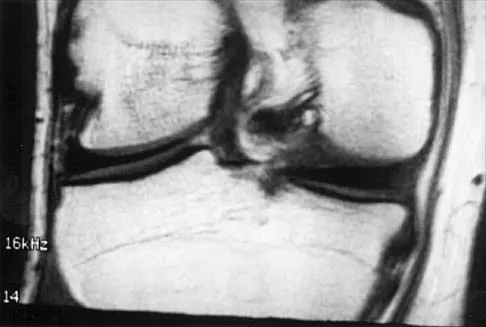
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?

Explanation
Question 15
The gluteus maximus is innervated by which of the following nerves?

Explanation
Question 16
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?

Explanation
Question 17
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?

Explanation
Question 18
A purulent flexor tenosynovitis of the thumb may communicate with the small finger flexor through which of the following structures?

Explanation
Question 19
Which of the following nerves travels with the deep palmar arch?

Explanation
Question 20
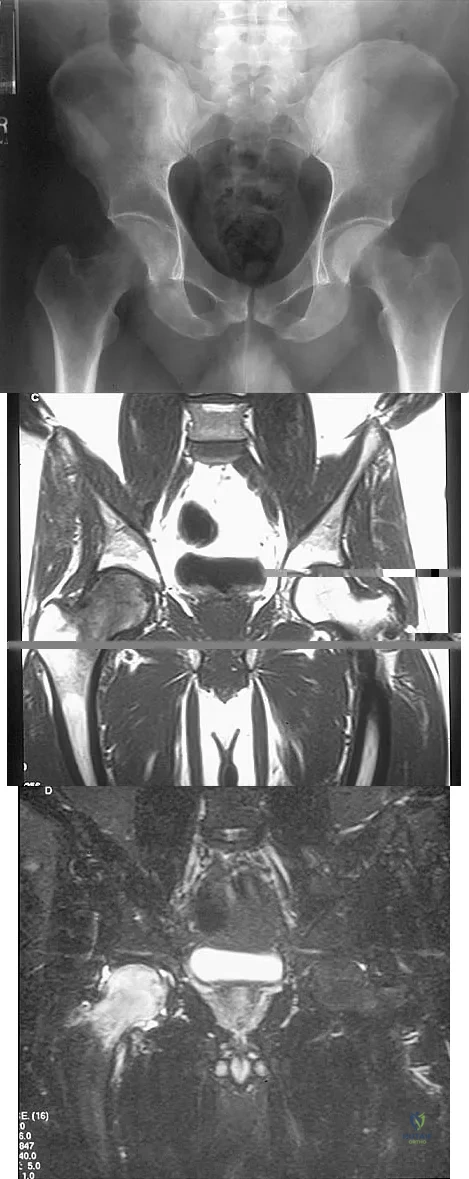
Figures 10a through 10c show the plain radiograph and MRI scans of a 41-year-old man who has right hip pain. What is the most likely diagnosis?
Explanation
Question 21
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?

Explanation
Question 22
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?

Explanation
Question 23
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?

Explanation
Question 24
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?

Explanation
Question 25
Which of the following findings is seen in the chest radiograph shown in Figure 13?

Explanation
Question 26
In the standard anterior Smith-Robinson approach to the cervical spine, the dissection interval relies on an internervous plane. Which of the following structures constitutes the medial boundary of this plane?
Explanation
Question 27
Figure 10 represents a cross-section of the shoulder. Which nerve exits the axilla posteriorly through the quadrilateral space?

Explanation
Question 28
The blood supply to the adult femoral head is predominantly provided by the lateral epiphyseal artery. This artery is a direct terminal branch of which of the following vessels?
Explanation
Question 29
When placing lumbar pedicle screws, accurate identification of the starting point is critical to avoid nerve root injury. The medial border of the lumbar pedicle correlates with which anatomic landmark on the posterior elements?
Explanation
Question 30
During a lateral approach to the proximal tibia and knee, the surgeon isolates a nerve that passes posterior to the biceps femoris tendon and wraps around the fibular neck. Injury to this nerve leads to severe weakness in which of the following movements?
Explanation
Question 31
Based on a normal cross-section of the forearm (as seen in Figure 6), the anterior interosseous nerve (AIN) courses distally along the interosseous membrane. Which of the following muscles is NOT innervated by the AIN?
Explanation
Question 32
In the standard posterolateral approach to the ankle for fixation of a posterior malleolus fracture, the internervous plane lies between the flexor hallucis longus and which of the following structures?
Explanation
Question 33
During a sacral laminectomy or decompression, the surgeon must be acutely aware of the termination of the dural sac. In the normal adult spine, the dural sac typically terminates at which vertebral level?
Explanation
Question 34
A patient presents with a deep penetrating injury to the palm and demonstrates an inability to forcefully cross the index and middle fingers. Which of the following nerves is most likely injured?
Explanation
Question 35
Figure 4 demonstrates a cross-section of the posterior thigh. The sciatic nerve generally divides into the tibial and common peroneal nerves proximally. Which muscle is exclusively innervated by the common peroneal division of the sciatic nerve?
Explanation
Question 36
During the Kocher approach to the radial head, the surgeon dissects through an internervous plane. This plane lies between the extensor carpi ulnaris and which other muscle?
Explanation
Question 37
The ilioinguinal approach is commonly used for anterior column acetabular fractures. Which nerve is at greatest risk of iatrogenic injury during the mobilization of the structures in the "middle window"?
Explanation
Question 38
When approaching the thoracic spine via a costotransversectomy, the artery of Adamkiewicz must be considered to avoid spinal cord ischemia. This critical vessel typically enters the spinal canal through an intervertebral foramen at which levels?
Explanation
Question 39
The deep motor branch of the ulnar nerve passes between the pisiform and the hook of the hamate in Guyon's canal. Which of the following structures forms the roof of this canal?
Explanation
Question 40
During open reduction and internal fixation of a calcaneus fracture via an extensile lateral approach, the surgeon elevates a full-thickness subperiosteal flap. Which nerve is at the highest risk of transection in the proximal vertical limb of the incision?
Explanation
Question 41
A patient exhibits marked lateral winging of the scapula following a lymph node biopsy in the posterior triangle of the neck. The patient struggles to abduct the shoulder past 90 degrees. Which nerve was most likely injured?
Explanation
Question 42
The vertebral artery is a critical vascular structure that ascends through the cervical spine. In the majority of the population, at which cervical vertebral level does the vertebral artery typically first enter the transverse foramen?
Explanation
Question 43
When evaluating injuries to the posterolateral corner of the knee, understanding the intricate capsuloligamentous anatomy is paramount. Which specific structure directly attaches the fibular head to the lateral meniscus?
Explanation
Question 44
During a Bankart repair, the surgeon must address the essential capsulolabral lesion. Which of the following structures serves as the primary static restraint to anterior translation of the humeral head when the shoulder is positioned in 90 degrees of abduction and maximal external rotation?
Explanation
Question 45
During a deltoid-splitting lateral approach to the proximal humerus, the axillary nerve is at significant risk of iatrogenic injury. What is the average anatomical distance from the lateral tip of the acromion to the axillary nerve in an adult?
Explanation
Question 46
A patient presents with a severe traction injury to the brachial plexus after a motorcycle collision. Physical examination reveals miosis, ptosis, and anhidrosis on the ipsilateral side. Avulsion of which nerve root is most likely responsible for these specific findings?
Explanation
Question 47
When decompressing Guyon's canal for ulnar nerve entrapment, a surgeon must be intimately aware of its boundaries. Which of the following structures forms the floor of Guyon's canal?
Explanation
Question 48
Compression of the posterior interosseous nerve (PIN) most commonly occurs at the Arcade of Frohse. This arcade is formed by the proximal aponeurotic edge of which muscle?
Explanation
Question 49
During anterior cervical spine surgery extending to the lower cervical segments, the vertebral artery is at risk. In the vast majority of the population, the vertebral artery enters the transverse foramen at which cervical level?
Explanation
Question 50
To properly place a lumbar pedicle screw, the surgeon must identify the correct starting point to avoid neurological injury. Anatomically, the standard starting point is defined by the intersection of the:
Explanation
Question 51
When performing a posterior approach to the hip (Kocher-Langenbeck), the medial femoral circumflex artery (MFCA) is at risk. The main ascending branch of the MFCA consistently runs deep to which muscle?
Explanation
Question 52
The posterolateral corner (PLC) of the knee provides critical rotatory stability. Which structure is the primary restraint to external rotation of the tibia at 30 degrees of knee flexion?
Explanation
Question 53
During a posterolateral approach to the ankle for fixation of a posterior malleolus fracture, the sural nerve must be protected. The sural nerve typically courses in close proximity to which structure in the distal leg?
Explanation
Question 54
During an ilioinguinal approach for an anterior column acetabular fracture, severe hemorrhage is encountered upon dissection over the superior pubic ramus. This bleeding is most likely from the corona mortis, an anastomosis between the:
Explanation
Question 55
The superficial radial nerve is at risk during the distal extent of the Henry approach to the forearm. Anatomically, it emerges from beneath which muscle in the distal third of the forearm to become subcutaneous?
Explanation
Question 56
A patient sustains a deep laceration to the palm, severing the deep branch of the ulnar nerve. Which of the following functional deficits is most likely to be observed?
Explanation
Question 57
When placing iliosacral screws for pelvic ring injuries, the surgeon must remain within the osseous safe zone of the sacral ala. The anterior limit of this safe zone in S1 is defined by the risk of injury to which structure?
Explanation
Question 58
A 25-year-old male develops acute compartment syndrome of the deep posterior compartment of the leg after a tibial fracture. Which of the following neurovascular structures is contained within this compartment?
Explanation
Question 59
During a medial subvastus approach to the distal femur, the adductor canal (Hunter's canal) is visualized. Which of the following nerves runs within the adductor canal?
Explanation
Question 60
A 28-year-old overhead athlete presents with isolated weakness in external rotation of the shoulder. An MRI reveals a paralabral cyst in the spinoglenoid notch. Which muscle is predominantly denervated?
Explanation
Question 61
The adult spinal cord typically terminates distally as the conus medullaris. In the majority of adults, this termination occurs at which vertebral body level?
Explanation
Question 62
The Master Knot of Henry is an important anatomical landmark in the plantar aspect of the midfoot. It refers to the intersection where the:
Explanation
Question 63
During a posterior cervical foraminotomy at C5-C6, the surgeon is mindful of the boundaries of the intervertebral foramen. The vertebral artery is typically located in which relation to the exiting C6 nerve root?
Explanation
Question 64
A 28-year-old volleyball player presents with insidious onset of vague posterior shoulder pain and profound weakness in external rotation, with preserved abduction. At what anatomical site is the injured nerve most likely compressed?
Explanation
Question 65
Figure 4 shows an anatomic dissection of the lateral aspect of the knee.
The primary restraint to external rotation of the tibia at 30 degrees of knee flexion inserts on which of the following structures?
Explanation
Question 66
When placing a pedicle screw at the L4 level, the optimal starting point is at the intersection of the pars interarticularis, the superior articular facet, and the transverse process. What nerve root is most at risk if the screw breaches the pedicle inferiorly?
Explanation
Question 67
A patient sustains a deep laceration over the volar aspect of the index finger metacarpophalangeal joint. The first lumbrical muscle is injured. What is its precise origin and innervation?
Explanation
Question 68
During a Kocher-Langenbeck approach to the hip, the surgeon must protect the primary blood supply to the femoral head. Which structure serves as a critical landmark to protect the deep branch of the medial femoral circumflex artery?
Explanation
Question 69
Figure 10 demonstrates standard portals for ankle arthroscopy.
When establishing the posterolateral portal, the sural nerve is at risk. What is its normal anatomical relationship to the portal site?
Explanation
Question 70
When placing Sacral Alar Iliac (SAI) screws for spinopelvic fixation, the trajectory crosses the SI joint. Which anterior structure is most at risk with an overly anterior and superior trajectory breach of the sacral ala?
Explanation
Question 71
A 45-year-old mechanic complains of chronic, aching pain in the proximal lateral forearm without overt motor weakness, exacerbated by resisted forearm supination. The most common site of compression for the involved nerve is the:
Explanation
Question 72
Figure 13 displays a cross-section of the midfoot.
The true Lisfranc ligament connects which two osseous structures?
Explanation
Question 73
During a deltopectoral approach for a proximal humerus fracture, identifying and protecting the axillary nerve is paramount. At what distance distal to the lateral acromial edge does the main trunk of the axillary nerve typically cross the humerus?
Explanation
Question 74
A spine surgeon evaluates a pre-operative CT scan for a T8 burst fracture. Compared to the lumbar spine, which of the following is true regarding the anatomy of mid-thoracic pedicles?
Explanation
Question 75
Figure 19 highlights an arthroscopic view of a meniscus.
Which of the following describes a key anatomical difference between the medial and lateral menisci?
Explanation
Question 76
A 21-year-old collegiate baseball pitcher is diagnosed with an ulnar collateral ligament (UCL) tear. The anterior bundle of the UCL inserts on the sublime tubercle. Which specific portion of the anterior bundle is most taut in extension?
Explanation
Question 77
Figure 25 details the anterior thigh musculature.
A patient requires a femoral nerve block. Which of the following accurately describes the position of the femoral nerve within the femoral triangle?

Explanation
Question 78
In atlas (C1) lateral mass screw fixation, the surgeon must avoid both vascular structures. Which anatomic trajectory and starting point minimizes the risk to both the vertebral artery and the internal carotid artery?
Explanation
Question 79
A patient complains of ulnar-sided wrist pain after a fall. MRI shows a tear of the foveal attachment of the Triangular Fibrocartilage Complex (TFCC). This specific attachment is critical for:
Explanation
Question 80
A patient develops an isolated acute compartment syndrome of the lateral compartment of the lower leg. Which of the following physical exam findings is most expected?
Explanation
Question 81
Figure 30 demonstrates the osseous landmarks of the scapula.
The coracoacromial ligament attaches to the acromion and the coracoid process. Which variation of the acromion morphology is most strongly associated with full-thickness rotator cuff tears?
Explanation
Question 82
During an anterior intrapelvic (modified Stoppa) approach for an acetabular fracture, significant hemorrhage occurs near the superior pubic ramus. The most likely source is the corona mortis, which represents an anastomosis between:
Explanation
Question 83
A surgeon is performing a lateral transpsoas approach to the L4-L5 disc space. To avoid injury to the lumbar plexus, the retractor should be placed carefully, as the nerve responsible for quadriceps function is located in which region of the psoas muscle at this level?
Explanation
Question 84
During a standard deltopectoral approach to the shoulder, the cephalic vein is identified in the interval. To optimally preserve its venous drainage, what is the standard recommended handling of this structure?
Explanation
Question 85
A 24-year-old athlete requires surgical reconstruction for a posterolateral corner knee injury. Identifying and protecting the common peroneal nerve is critical. Which of the following describes its most reliable anatomical position in the posterolateral knee?
Explanation
Question 86
An anterior cervical discectomy and fusion (ACDF) is planned at the C6-C7 level. A right-sided approach is historically considered to have a higher risk of recurrent laryngeal nerve (RLN) injury compared to a left-sided approach due to which anatomical variant?
Explanation
Question 87
A patient presents with weakness in flexing the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which anomalous structure is most commonly responsible for compressing the nerve involved?
Explanation
Question 88
During a Kocher-Langenbeck (posterior) approach to the acetabulum, identifying the sciatic nerve is essential. The nerve classically exits the greater sciatic foramen in what relation to the short external rotators?
Explanation
Question 89
The deep palmar arch of the hand provides significant collateral blood flow. It is primarily formed by the anastomosis of which of the following vessels?
Explanation
Question 90
When performing an anterior approach for a thoracolumbar corpectomy, the surgeon must be aware of the artery of Adamkiewicz to prevent anterior spinal cord syndrome. This vessel most commonly arises from the aorta at which levels?
Explanation
Question 91
An anterolateral approach to the distal tibia is used for pilon fracture fixation. The superficial peroneal nerve is at risk in this exposure. Where does this nerve predictably pierce the deep fascia to become subcutaneous?
Explanation
Question 92
A patient sustains an injury resulting in medial winging of the scapula. Which nerve is injured, and what are its correct nerve root origins?
Explanation
Question 93
A surgeon is performing a midfoot reconstruction and exploring the plantar aspect of the foot. The Master Knot of Henry is identified. This anatomical landmark represents the intersection of which two structures?
Explanation
Question 94
During placement of an S1 iliosacral screw for a displaced sacral fracture, an anterior extraosseous screw trajectory risks injuring which neural structure passing over the sacral ala?
Explanation
Question 95
When utilizing a dorsal approach to the wrist, Lister's tubercle is a key osseous landmark. It serves as a mechanical pulley for which tendon?
Explanation
None
