Comprehensive Surgical Management of Talar Head Fractures and Talar Vascular Anatomy

Key Takeaway
Talar head fractures account for 5% to 10% of all talar injuries, often resulting from axial loading. Because the talus relies on a tenuous retrograde blood supply, precise anatomical reduction and rigid internal fixation are critical to prevent osteonecrosis and post-traumatic arthrosis. This guide covers the complex vascular anatomy of the talus, indications for operative intervention, surgical approaches, and postoperative rehabilitation protocols for orthopedic surgeons.
INTRODUCTION TO TALAR OSTEOLOGY AND BIOMECHANICS
The talus is a unique biomechanical keystone within the human foot, responsible for transmitting the entire weight of the body from the tibia to the longitudinal arch. Approximately 60% of its surface is covered by articular cartilage, articulating with the tibia, fibula, calcaneus, and navicular. Notably, the talus is devoid of any direct muscular or tendinous attachments, relying entirely on ligamentous structures and joint capsules for its vascular supply. This anatomical peculiarity renders the talus exceptionally vulnerable to ischemic injury following trauma.
Understanding the intricate extraosseous and intraosseous vascular networks is paramount for the orthopedic surgeon. Surgical approaches and fixation strategies must be meticulously planned to preserve the remaining blood supply, thereby mitigating the catastrophic complication of osteonecrosis (avascular necrosis, AVN).

VASCULAR ANATOMY OF THE TALUS
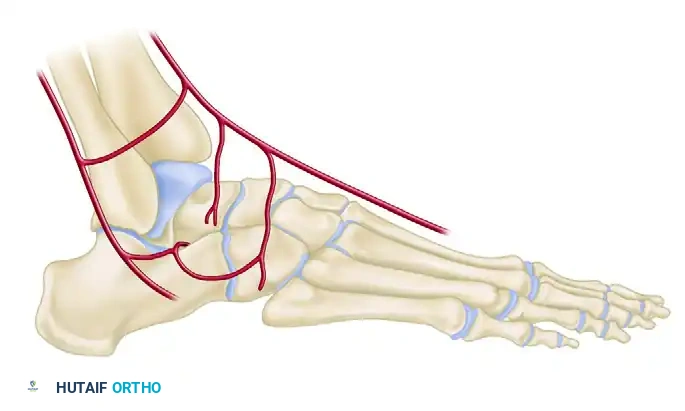
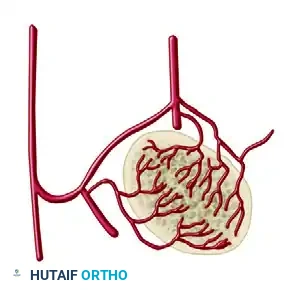
The vascular anatomy of the talus has been extensively studied and mapped, most notably by Mulfinger and Trueta. The three major arteries of the leg—the anterior tibial, posterior tibial, and peroneal arteries—contribute to a rich, extraosseous, anastomotic plexus that supplies blood to the head, neck, and body of the talus.
Clinical Pearl: The overall contribution of the blood supply to the talus is distributed as follows: posterior tibial artery (47.0%), anterior tibial artery (36.2%), and peroneal artery (16.9%). The anterior tibial artery is the primary supplier to the anteromedial quadrant, while the posterior tibial artery dominates the remaining three quadrants.
Extraosseous Arterial Supply
The extraosseous supply forms a vascular ring around the talar neck and sinus tarsi, sending intraosseous branches retrogradely into the talar body.
1. The Artery of the Tarsal Canal
Branching off the posterior tibial artery approximately 1 cm proximal to its division into the medial and lateral plantar arteries, the artery of the tarsal canal is the most consistent and major supplier of blood to the body of the talus. The tarsal canal itself is formed by the sulcus on the inferior surface of the talus and the superior sulcus of the calcaneus, containing both this artery and the talocalcaneal intraosseous ligament. The canal runs from posteromedial to anterolateral, opening into the tarsal sinus. Within the canal, the artery sends four to six direct vessels superiorly into the talar body.
2. The Deltoid Artery
Arising as a branch off the artery of the tarsal canal, the deltoid artery directly supplies the medial one-fourth to one-half of the talar body. Because of extensive intraosseous anastomoses, it possesses the potential to supply a much greater area if other sources are compromised.
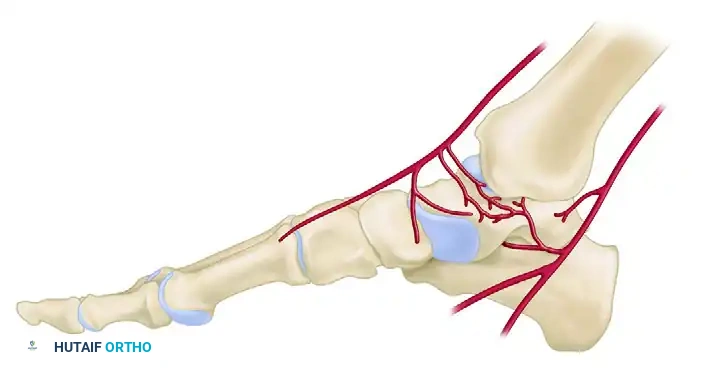
3. The Artery of the Sinus Tarsi
This vessel exhibits high variability in size and origin. It is typically formed by branches of the perforating peroneal artery, the dorsalis pedis (or anterior tibial) artery, or an anastomosis between the two. It supplies the lateral one-eighth to one-fourth of the talar body. Crucially, it forms an anastomosis with the artery of the tarsal canal, creating a vascular sling that can provide collateral flow to the talus.
4. Superior Neck Vessels
The head and neck regions are richly supplied by the superior neck vessels, which branch off the dorsalis pedis artery and the artery of the sinus tarsi. Because of this robust, redundant supply, osteonecrosis of the talar head and neck is extremely rare compared to the talar body.
5. Posterior Tubercle Vessels
The posterior tubercle is supplied by direct, albeit small, branches from the posterior tibial artery (most commonly) or the peroneal artery. Through intraosseous anastomoses, this region also has the potential to perfuse more of the talar body.
Recent Anatomical Discoveries
Recent gadolinium-enhanced MRI cadaveric studies have identified a previously underappreciated direct branch to the medial talar neck arising from the posterior tibial artery.
Surgical Warning: This newly described medial talar neck artery is at significant risk during a standard anteromedial approach for talar neck fractures. However, studies demonstrate that it is preserved if a medial malleolar osteotomy is utilized for exposure. Conversely, the anterolateral approach to the talar neck does not appear to disrupt any major blood supply.
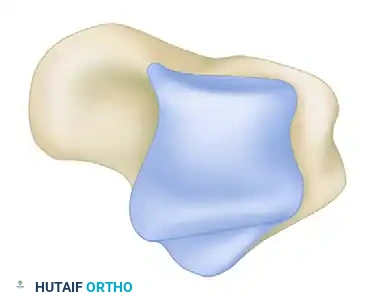
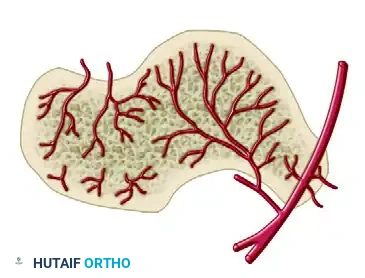
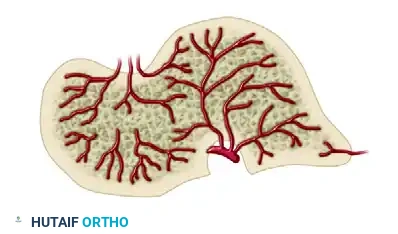
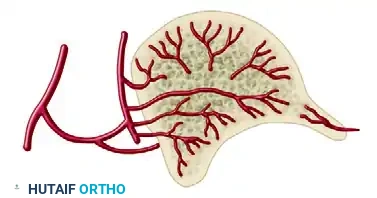
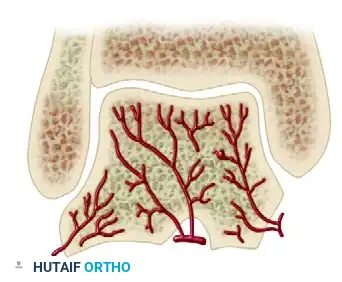
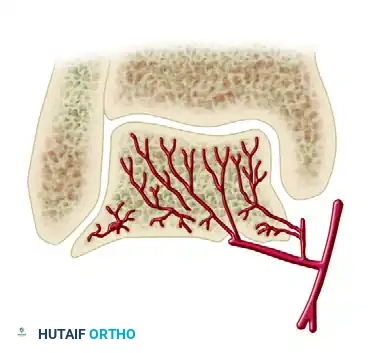
Cross-Sectional Intraosseous Vascular Mapping
The intraosseous distribution of these vessels is complex. The following series of diagrams illustrates the sagittal and coronal perfusion zones of the talus, highlighting the critical watershed areas within the talar body.





TALAR HEAD FRACTURES: PATHOPHYSIOLOGY AND DIAGNOSIS
Fractures of the head of the talus are relatively uncommon, constituting 5% to 10% of all talar injuries. The talar head articulates with the navicular anteriorly, forming the talonavicular joint—a critical component of the triple joint complex (coxa pedis) responsible for hindfoot inversion and eversion.
Mechanism of Injury
Two primary mechanisms of injury have been suggested in the literature:
1. Axial Loading and Compression: A longitudinally directed force transmitted through the midfoot, compressing the talar head against the navicular. This often results in an impacted or comminuted fracture pattern.
2. Dorsal Compression: A forced dorsiflexion injury causing the anterior tibial plafond to shear or compress the dorsal aspect of the talar head.
Clinical Evaluation and Imaging
Because recognition of this fracture can be difficult, a high index of suspicion must be maintained for any patient presenting with posttraumatic tenderness in the anterior ankle or dorsal midfoot region.
- Physical Examination: Patients typically present with swelling, ecchymosis, and inability to bear weight. Palpation over the talonavicular joint elicits severe pain. The clinician must assess for clinical instability of the triple joint complex, as loss of support at the talonavicular joint compromises the entire medial column.
- Associated Injuries: Injuries to the calcaneocuboid and subtalar joints are highly common and must be actively ruled out.
- Radiographic Evaluation: Plain radiographs (AP, lateral, and oblique views of the foot and ankle) may define the fracture clearly. However, overlapping osseous structures often obscure the true extent of the injury.
- Advanced Imaging: Computed Tomography (CT) is considered mandatory for definitive diagnosis, evaluation of displacement, assessment of intra-articular comminution, and preoperative planning.

SURGICAL MANAGEMENT OF TALAR HEAD FRACTURES
The primary goals of treatment are to restore the congruity of the talonavicular joint, maintain the length of the medial column, and preserve the tenuous vascular supply to the talus.
Indications for Operative Intervention
- Displaced Fractures: Any displacement greater than 1-2 mm, particularly shear-type injuries, warrants Open Reduction and Internal Fixation (ORIF).
- Impacted Fractures: Articular impaction leading to joint incongruity requires elevation and bone grafting.
- Instability: Fractures associated with subluxation or dislocation of the talonavicular joint.
Patient Positioning and Preparation
- The patient is placed in the supine position on a radiolucent operating table.
- A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, bringing the medial column of the foot into direct view.
- A thigh tourniquet is applied to ensure a bloodless surgical field.
- Fluoroscopy is positioned to allow for intraoperative AP, lateral, and oblique views of the foot.
Surgical Approaches
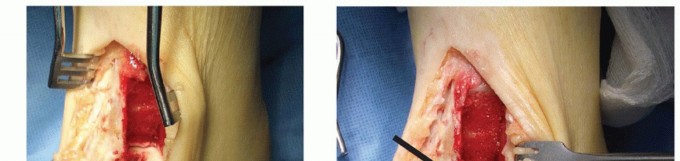
Shear fractures of the talar head, although usually medial, can often be adequately exposed through a dorsomedial incision.
- Incision: A longitudinal incision is made centered over the talonavicular joint, just medial to the tibialis anterior tendon.
- Superficial Dissection: Care must be taken to identify and protect the terminal branches of the superficial peroneal nerve and the saphenous nerve.
- Deep Dissection: The capsule of the talonavicular joint is incised longitudinally. Crucial Step: The surgeon must strictly avoid stripping any remaining soft tissue attachments from the talar neck and head to preserve the superior neck vessels and the artery of the sinus tarsi.
Step-by-Step Operative Technique (ORIF)
- Joint Inspection and Debridement: The fracture hematoma is evacuated. Small, avascular, non-articular osteochondral fragments that cannot be fixed are excised.
- Reduction of Impacted Fractures: If the articular surface is impacted, a small osteotome or dental pick is used to carefully elevate the articular fragment to match the contour of the navicular.
- Bone Grafting: Once elevated, a void is inevitably created behind the articular fragment. This must be filled with cancellous bone graft (autograft from the distal tibia or calcaneus, or allograft) to provide subchondral support and minimize postoperative collapse.
- Reduction of Shear Fractures: Large shear fragments are reduced anatomically using pointed reduction forceps.
- Fixation: Stable fixation is accomplished using 2.0 mm to 3.0 mm partially threaded cancellous lag screws, headless compression screws, or bioabsorbable pins. Fixation can be placed directly through the dorsal incision or percutaneously from the medial side as dictated by the fracture geometry. All screw heads must be countersunk beneath the articular cartilage to prevent impingement on the navicular.
- Joint Stability Assessment: Care must be taken to ensure the talonavicular joint is concentrically reduced. If the joint remains unstable after fracture fixation, it may be necessary to place a temporary Kirschner wire (K-wire) across the talonavicular joint to hold it reduced.
- Medial Column Restoration: In cases of fracture-dislocation with shortening of the medial column, an intraoperative external fixator (spanning from the medial cuneiform to the medial talar body or calcaneus) may be required to distract the joint, gain length, and facilitate reduction.

Management of Severe Comminution and Arthrodesis
In cases of severe, non-reconstructible comminution of the talar head, primary arthrodesis of the talonavicular joint may be indicated. Arthrodesis is reserved as a salvage procedure because it effectively eliminates motion in the entire triple joint complex (subtalar, talonavicular, and calcaneocuboid joints).
Pitfall: If an isolated talonavicular arthrodesis is performed, the surgeon must absolutely avoid shortening the medial column of the foot. Shortening leads to a fixed varus deformity of the hindfoot and lateral column overload.
The Adelaar Inlay Tricortical Graft Technique:
To prevent medial column shortening, an inlay tricortical bone graft, as described by Adelaar, is highly recommended.
1. A tricortical structural graft is harvested from the ipsilateral anterior iliac crest.
2. The comminuted talar head fragments are excised back to bleeding, viable bone on the talar neck.
3. The articular cartilage of the proximal navicular is denuded.
4. The foot is distracted to its anatomic length, and the tricortical graft is contoured and impacted into the defect.
5. Rigid fixation is achieved with crossed lag screws or a medial column spanning plate.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
Rehabilitation
The postoperative rehabilitation protocol is dictated by the security of the internal fixation and the quality of the patient's bone.
- Secure Fixation:
- 0-2 Weeks: The patient is placed in a bulky Jones splint and remains strictly non-weight bearing (NWB).
- 2-6 Weeks: If secure fixation was obtained, early active and passive range of motion (ROM) of the ankle and subtalar joints can be initiated at approximately 2 weeks. The patient remains NWB in a removable controlled ankle motion (CAM) boot.
- 6-12 Weeks: Delayed, progressive weight bearing is initiated at a minimum of 6 weeks, contingent upon radiographic evidence of bridging callus.
- Marginal Fixation:
- If fixation is tenuous or bone quality is poor, the patient is placed in a rigid short-leg cast for a full 6 weeks with strict non-weight bearing. ROM exercises are delayed until clinical and radiographic stability is assured.
Complications
1. Osteonecrosis (AVN):
Despite the rich blood supply to the talar head relative to the body, osteonecrosis of the head segment has been reported to occur in approximately 10% of cases. This is usually secondary to aggressive surgical stripping or severe initial displacement. Serial radiographs should be monitored for the Hawkins sign (subchondral radiolucency indicating revascularization), though this is less reliable in the head than in the talar body.
2. Post-Traumatic Arthrosis:
Degenerative arthrosis of the talonavicular joint is the most common long-term complication, arising from initial cartilage impact damage or subtle residual incongruity. If symptomatic conservative management (orthotics, bracing, injections) fails, a secondary talonavicular arthrodesis is the definitive treatment of choice.
3. Nonunion / Malunion:
Failure to restore the medial column length results in a malunion characterized by a varus hindfoot and midfoot collapse. Treatment requires a complex reconstructive osteotomy and structural bone grafting. Nonunion is rare but may occur if the vascular supply is severely compromised; it is managed with revision fixation and autologous bone grafting.
You Might Also Like