(a) the cord may or may not be transected,
(b) the nerve roots may be undamaged, partly divided or completely divided.
15
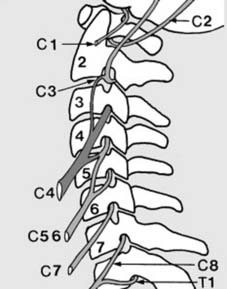
Anatomical features (b): Cervical cord:
Note:
1. The phrenic nerve arises from C4, with minor contributions from C3 and C5. Cord section proximal to the phrenic nerve will lead to rapid death from respiratory paralysis. Those with lesions at C4-5, and more distal, are capable of respiration without external support.
2. C2 and C3 supply the vertex and occiput (accounting for pain here in upper cervical lesions).
C5–T1 contribute to the brachial plexus. (The illustration is diagrammatic.)
16
Assessing the neurological level of cord or nerve root injury:
Cord or root damage is reflected in disturbance of myotomes or dermatomes.
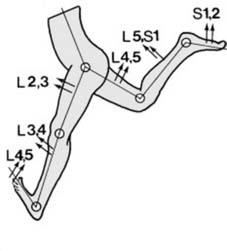
Myotomes (a):
As a rule, motion in each joint is logically controlled by four myotomes in sequence: viz. Hip flexion, L2, 3, extension L4, 5. Knee extension, L3, 4 (including knee jerk), flexion L5, S1. Ankle dorsiflexion L4, 5, plantar flexion S1, S2 (including ankle jerk). (In addition, inversion is controlled by L4 and eversion by L5, S1.)
17
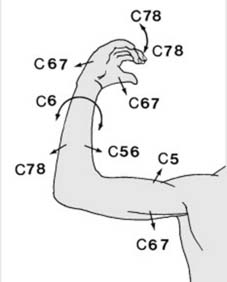
Myotomes (b):
In the upper limb, the arrangement is less regular:
Shoulder abduction
C5, adduction C6, 7.
Elbow flexion
C5, 6 (including biceps jerk), extension C7, 8 (including triceps jerk).
Wrist flexion and extension
; both C6, 7.
Finger flexion and extension
, C7, 8.
Pronation and supination
C6 (including supinator jerk).
Hand intrinsic muscles
T1.
18.
MRC grading:
Muscle activity should be assessed using the MRC scale:
M0
– No active contraction
M1
– a flicker of movement can be seen or palpated, but this is not enough to produce movement
M2
– weak contraction which can produce movement if gravity is eliminated
M3
– contraction weak, but can produce movement against gravity
M4
– strength not full, but can produce movement against gravity and some resistance
M5
– full strength
Motor index score:
This is useful for assessing the extent of motor loss, and for gauging any improvement or deterioration. In the upper limb, biceps, the wrist extensors, triceps, flexor digitorum profundus and the hand, intrinsics are each assessed using the MRC Grading system and added together. The totals for the right upper extremity and left upper extremity (RUE and LUE) are noted (25 in each normal limb). The procedure is repeated in the lower limb, using the hip flexors, quadriceps, tibialis anterior, extensor hallucis longus, and gastrocnemius.
19
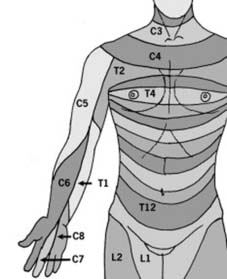
Dermatomes (a):
In the upper limb, the anterior axial line follows the line of the second rib from the angle of Louis, and continues down the anterior aspect of the arm, splitting near the middle finger which is supplied by C7. The other dermatomes are arranged in a regular fashion on either side of the axial line. If indicated, a
sensory index score
may be made for each limb (0 = absent sensation; 1 = impaired; 2 = normal).
20
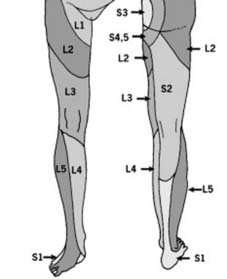
Dermatomes (b):
The lumbar and sacral dermatomes have a complex arrangement which is difficult to commit to memory. Remember by the facts that: 1. The outer border of the foot is supplied by S1; 2. The medial part of the foot and the lateral part of the leg by L5; 3. The ‘stocking top’ area is supplied by L2 and 4. the saddle area by S3. ‘We kneel on L3, stand on S1, and sit on S3.’
NEXT
DETERMINING THE SEVERITY OF NEUROLOGICAL INVOLVEMENT
Vital Anatomical Features (b) of the Cervical Cord: Understand Paralysis Risk
Updated: Feb 2026
62 Views
Key Medical Takeaway
This article provides essential research regarding Vital Anatomical Features (b) of the Cervical Cord: Understand Paralysis Risk. Anatomical features b primarily refer to the cervical cord and its associated nerve roots. In injuries, the cord may or may not be transected, potentially impacting vital functions like respiration if proximal to the C4 phrenic nerve origin. Nerve roots within these anatomical features b can be undamaged, partly divided, or completely divided, affecting myotomes and dermatomes.
Table of Contents

Keywords