Anatomic Reconstruction of Lateral Ankle Instability: A Masterclass in the Modified Brostrom-Gould Technique

Key Takeaway
This masterclass details the Modified Brostrom-Gould procedure for chronic lateral ankle instability. We meticulously cover surgical anatomy, preoperative planning, and a step-by-step intraoperative guide, emphasizing precise dissection, nerve protection, and ligamentous repair. Fellows will learn to identify and address pathology, manage complications, and ensure robust postoperative rehabilitation for excellent functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
Chronic lateral ankle instability represents a profound biomechanical and neuromuscular failure of the tibiotalar and subtalar articulations, fundamentally altering the kinematic chain of the lower extremity. While acute ankle sprains are ubiquitous—representing up to 40% of all athletic trauma and occurring at a staggering incidence of approximately 10,000 cases per day in the general population—the long-term sequelae of these injuries are often underestimated by primary care providers. As orthopedic surgeons, we recognize that what appears to be a simple inversion injury can precipitate a cascading cycle of microtrauma, ligamentous attenuation, and intra-articular derangement. Up to 50% of patients who sustain a significant acute lateral ankle sprain will eventually develop chronic symptoms, making this one of the most frequently encountered pathologies in a foot and ankle specialist's practice.
The pathogenesis of chronic lateral ankle instability is classically bifurcated into two distinct, yet frequently overlapping, clinical entities: functional instability and mechanical instability. Functional instability is characterized by the subjective sensation of the ankle "giving way" during dynamic loading, cutting, or pivoting maneuvers. This phenomenon is largely driven by proprioceptive deafferentation. When the lateral ligaments are ruptured, the embedded mechanoreceptors (Ruffini endings, Pacinian corpuscles, and Golgi tendon organs) are damaged, leading to delayed neuromuscular firing of the peroneal musculature and impaired postural control. Mechanical instability, conversely, is defined by objective, supra-physiologic laxity of the tibiotalar or subtalar joint complex, demonstrable through clinical stress testing or radiographic evaluation.
When mechanical and functional instability coalesce, the natural history of the joint is grim if left untreated. The repetitive episodes of subluxation generate abnormal shear forces across the articular cartilage of the talar dome, significantly increasing the risk of osteochondral lesions of the talus (OCLs). Furthermore, the chronic alteration in joint contact mechanics inevitably leads to asymmetric wear patterns, capsular hypertrophy, and the development of anterior tibiotalar impingement exostoses. Over time, this pathologic cascade culminates in irreversible post-traumatic osteoarthritis.
The primary objective of surgical intervention is to interrupt this degenerative cycle. The Modified Brostrom-Gould procedure—an anatomic reconstruction of the lateral ligamentous complex—has emerged as the gold standard for addressing mechanical instability. Unlike historical non-anatomic tenodesis procedures (such as the Chrisman-Snook or Watson-Jones) that sacrifice normal kinematics and peroneal function, the anatomic approach restores the native constraints of the joint. By imbricating the attenuated anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL), and augmenting the repair with the inferior extensor retinaculum, we can reliably restore stability while preserving physiological range of motion and dynamic evertor strength.
Detailed Surgical Anatomy and Biomechanics
A masterclass in lateral ankle reconstruction demands an intimate, three-dimensional understanding of the regional anatomy. The stability of the ankle mortise relies on an elegant interplay between osseous architecture, static ligamentous restraints, and dynamic musculotendinous units. The bony configuration—comprising the inherently stable mortise in dorsiflexion—provides approximately 30% of the joint's stability. The remaining 70% is entirely dependent on the integrity of the soft tissue envelope, which we must meticulously navigate and restore.
Static Stabilizers of the Lateral Ankle
The lateral collateral ligamentous complex of the ankle consists of three distinct bands: the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The ATFL is a flat, trapezoidal band that originates from the anterior border of the distal fibula and inserts onto the talar body, just anterior to the lateral articular facet. Biomechanically, it is the weakest of the lateral ligaments and is invariably the first to fail during a plantarflexion-inversion injury. It serves as the primary restraint against anterior translation of the talus within the mortise and limits internal rotation of the talus.
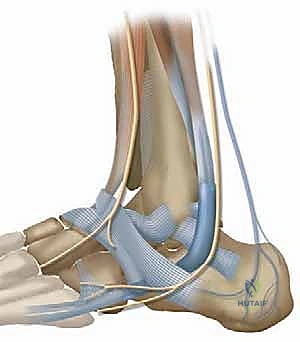
The CFL is a robust, cord-like structure originating just inferior to the ATFL footprint on the fibula. It courses obliquely in a posterior, inferior, and medial direction, passing deep to the peroneal tendons to insert on a small tubercle on the lateral calcaneal wall. Crucially, the CFL spans two joints—the tibiotalar and the subtalar joint—making it a critical stabilizer for both. It becomes taut in dorsiflexion and is the primary restraint against excessive varus tilt of the talus and calcaneus. The PTFL, conversely, is a thick, trapezoidal ligament originating from the posterior malleolus and inserting on the lateral talar tubercle. It is the strongest of the complex and is rarely torn except in cases of frank ankle dislocation.
Dynamic Stabilizers and Periarticular Musculature
Beyond the static ligaments, the dynamic stabilization of the lateral ankle is governed by the peroneal musculature. The peroneus brevis and peroneus longus tendons descend posterior to the lateral malleolus, housed within the retromalleolar groove and secured by the superior peroneal retinaculum. The peroneus brevis inserts onto the tuberosity of the fifth metatarsal base, acting as a powerful evertor and secondary plantarflexor. The peroneus longus traverses the plantar aspect of the foot through the cuboid tunnel to insert on the medial cuneiform and first metatarsal base, stabilizing the first ray during the terminal stance phase of gait.
These dynamic structures are paramount for protecting the lateral ligaments. In a healthy ankle, sudden inversion stress triggers a rapid reflex contraction of the peroneal muscles, resisting the deforming force. In the chronically unstable ankle, this reflex arc is often blunted due to proprioceptive loss, or the tendons themselves may be compromised by longitudinal split tears or subluxation secondary to superior peroneal retinaculum incompetence. During our surgical approach, careful inspection of the peroneal tendons is mandatory, as unaddressed tendinopathy can lead to persistent lateral ankle pain despite a successful ligament reconstruction.
Neurovascular Topography and High-Risk Zones
The lateral aspect of the ankle is a veritable minefield of superficial sensory nerves. Iatrogenic injury to these structures is the most common complication of lateral ankle surgery and can result in debilitating neuromas or complex regional pain syndrome (CRPS). The sural nerve courses subcutaneously along the posterolateral aspect of the ankle, typically running 1 to 1.5 centimeters posterior to the lateral malleolus before curving anteriorly along the lateral border of the foot. It is highly vulnerable during the posterior extension of our incision or during the placement of retractors.

Equally critical is the superficial peroneal nerve (SPN), which pierces the deep fascia of the anterior compartment approximately 10 to 12 centimeters proximal to the ankle joint. It quickly arborizes into the medial and intermediate dorsal cutaneous nerves. The lateral branch of the intermediate dorsal cutaneous nerve frequently crosses the anterior aspect of the lateral malleolus, placing it directly in the path of our standard curvilinear incision. Meticulous blunt dissection through the subcutaneous tissues, utilizing mosquito hemostats to gently spread parallel to the nerve fibers, is essential to mobilize and protect these delicate branches throughout the procedure.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention must be predicated on a rigorous clinical evaluation, confirming both the presence of mechanical instability and the failure of exhaustive non-operative measures. Surgery is never the first-line treatment for an isolated, uncomplicated ankle sprain, regardless of the severity of the initial ligamentous disruption.
Clinical and Radiographic Indications
The primary indication for a Modified Brostrom-Gould reconstruction is chronic, symptomatic mechanical lateral ankle instability that has proven refractory to a minimum of three to six months of dedicated conservative management. Patients must report recurrent episodes of "giving way," particularly on uneven terrain or during athletic endeavors, accompanied by pain, swelling, and a subjective loss of confidence in the joint.
Clinically, these patients will demonstrate a positive anterior drawer test, indicating ATFL incompetency. This is performed with the knee flexed to 90 degrees to relax the gastrocnemius, drawing the heel forward while stabilizing the tibia. A positive test is characterized by excessive anterior translation (typically >10 mm) or a "soft" endpoint compared to the contralateral side. Similarly, a positive talar tilt test—applying a varus stress to the hindfoot—indicates CFL insufficiency. Radiographically, stress views are utilized to quantify this laxity, with an anterior translation difference of >3 mm or an absolute translation of >10 mm, and a talar tilt difference of >5 degrees compared to the uninjured side, serving as objective benchmarks for surgical intervention.
Absolute and Relative Contraindications
While highly successful in appropriately selected patients, the Modified Brostrom-Gould procedure is not a panacea and carries specific contraindications that must be respected to avoid catastrophic failure.
| Contraindication Category | Specific Condition | Rationale and Considerations |
|---|---|---|
| Absolute Contraindications | Active Infection | High risk of deep joint space infection and hardware seeding. |
| Charcot Arthropathy | Severe loss of protective sensation and neurotraumatic joint destruction will lead to immediate failure of any soft-tissue repair. | |
| Severe Peripheral Vascular Disease | Inadequate tissue perfusion precludes reliable wound healing and increases amputation risk. | |
| Relative Contraindications | Uncorrected Hindfoot Varus | A fixed varus alignment mechanically overloads the lateral ligamentous repair. Concomitant lateralizing calcaneal osteotomy is mandatory. |
| Generalized Ligamentous Laxity (e.g., Ehlers-Danlos, Marfan Syndrome) | Native tissue is inherently poor quality. Primary repair has a high failure rate; consider allograft reconstruction or synthetic augmentation (InternalBrace). | |
| Severe Osteoarthritis | Ligament repair will not alleviate arthritic pain. Arthrodesis or arthroplasty should be considered. | |
| Morbid Obesity / Non-compliance | Excessive mechanical loading or inability to adhere to strict post-operative weight-bearing protocols drastically increases the risk of early anchor pull-out or tissue stretching. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the foundation of surgical success. The surgeon must synthesize clinical findings, imaging data, and patient-specific anatomical variations to formulate a precise operative strategy. This is not a "cookie-cutter" operation; the degree of tissue attenuation, the presence of concomitant pathology, and the patient's functional demands dictate the nuances of the reconstruction.
Diagnostic Imaging and Templating
Standard weight-bearing radiographs (AP, lateral, and mortise views) of the ankle are mandatory to assess overall joint congruency, rule out degenerative changes, and identify subtle fractures such as avulsions of the lateral malleolus or anterior process of the calcaneus. We carefully evaluate the talocrural angle and the presence of any varus tilt on the weight-bearing AP view.
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the soft tissue envelope prior to surgery. MRI allows for direct visualization of the ATFL and CFL, detailing whether the ligaments are completely avulsed, chronically thickened and attenuated, or encased in scar tissue.
Crucially, the MRI must be scrutinized for associated intra-articular pathology that requires concurrent treatment. Up to 30% of patients with chronic instability will have a concomitant osteochondral lesion of the talus (OCL), which may necessitate debridement, microfracture, or grafting. Furthermore, the peroneal tendons must be evaluated for tenosynovitis, split tears, or subluxation, as failure to address peroneal pathology will compromise the clinical outcome of the ligament reconstruction.
Anesthesia, Positioning, and Tourniquet Application
The procedure is typically performed under general anesthesia or a regional block (popliteal and saphenous nerve blocks), the latter providing excellent post-operative analgesia. Once anesthetized, the patient is positioned supine on the operating table.
A crucial positioning maneuver is the placement of a large bump (e.g., a rolled blanket or sandbag) under the ipsilateral hip. This internally rotates the lower extremity, bringing the lateral malleolus prominently into the anterior surgical field and allowing the foot to rest in a neutral position. A well-padded pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, which is vital for identifying the delicate cutaneous nerves and precise anatomical dissection. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered 30 minutes prior to inflation of the tourniquet. The limb is then prepped and draped in a standard sterile orthopedic fashion, ensuring the entire foot and distal half of the leg are exposed for intraoperative manipulation.
Step-by-Step Surgical Approach and Fixation Technique
The Modified Brostrom-Gould technique is an elegant procedure that relies on precise anatomical identification, meticulous tissue handling, and robust mechanical fixation. The goal is to recreate the native footprints of the ATFL and CFL, restoring normal tension and kinematics to the lateral ankle complex.
Incision, Dissection, and Nerve Protection
We begin with a 4 to 6 centimeter curvilinear incision centered over the anterior border of the distal fibula. The incision starts approximately 2 centimeters proximal to the distal tip of the lateral malleolus, curving gently anteriorly and distally toward the sinus tarsi and the base of the fourth metatarsal.

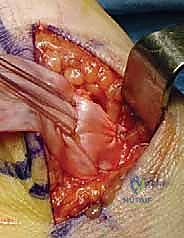
Superficial dissection is performed with extreme caution. We utilize blunt spreading techniques with a hemostat or tenotomy scissors to part the subcutaneous fat, remaining vigilant for the lateral branch of the superficial peroneal nerve superiorly and the sural nerve inferiorly. Once identified, these nerves are gently mobilized and protected with small vessel loops or blunt retractors. The deep fascia is then incised in line with the skin incision, exposing the lateral capsule and the inferior extensor retinaculum.

The inferior extensor retinaculum is a critical structure in the Gould modification. It is carefully sharply dissected off the underlying joint capsule and mobilized anteriorly. This layer will later be advanced proximally and sutured to the fibula to reinforce the ligament repair, provide a check-rein against inversion, and potentially restore proprioceptive mechanoreceptors to the lateral ankle.
Arthrotomy and Joint Inspection
Before addressing the ligaments, an anterior arthrotomy is performed to inspect the tibiotalar joint. An incision is made through the anterolateral capsule, extending from the distal fibula toward the talar neck.

A thorough intra-articular inspection is mandatory. We utilize a small rongeur or curette to excise any hypertrophic synovitis or scar tissue (the "meniscoid lesion") in the lateral gutter, which is a common source of chronic impingement pain. The talar dome is meticulously probed to ensure there are no occult osteochondral lesions that were missed on preoperative MRI. Any anterior tibial osteophytes that may contribute to anterior impingement are excised with an osteotome or rongeur. Once the joint is cleared of pathology, we turn our attention to the lateral ligamentous complex.

The Modified Brostrom-Gould Reconstruction
The remnants of the ATFL and CFL are identified. Often, these ligaments are stretched, attenuated, and scarred into the lateral capsule. We sharply detach the capsuloligamentous flap from its origin on the anterior border of the distal fibula, leaving a small cuff of tissue if possible.

The fibular footprint is then aggressively decorticated using a rongeur, curette, or a small burr to expose bleeding subchondral bone. This creates a biologically active bed that promotes robust ligament-to-bone healing.

We typically utilize two suture anchors for the repair. The first anchor (often a 3.0mm or 3.5mm biocomposite or PEEK anchor loaded with high-strength non-absorbable suture) is placed at the anatomic origin of the ATFL, approximately 1.5 cm proximal to the distal tip of the fibula along its anterior border. The second anchor is placed at the origin of the CFL, closer to the distal tip of the fibula.

The sutures are then passed through the proximal edge of the attenuated ATFL and CFL complex using a horizontal mattress configuration.

Crucially, before tying the sutures, the ankle must be positioned correctly. The foot is held in maximum dorsiflexion and slight eversion to appropriately tension the ligaments and reduce the talus within the mortise. While an assistant maintains this position, the sutures are tied, imbricating the ligaments in a "pants-over-vest" fashion directly onto the decorticated fibula.

Finally, the Gould modification is executed. The mobilized lateral border of the inferior extensor retinaculum is pulled proximally and posteriorly over the primary repair.

It is secured to the anterior border of the fibula using the remaining suture tails from the anchors or separate interrupted sutures. This step significantly augments the mechanical strength of the repair and limits deleterious inversion forces during the healing phase.

The wound is thoroughly irrigated, the subcutaneous tissues are closed with absorbable sutures, and the skin is reapproximated with a subcuticular closure or nylon sutures.
Complications, Incidence Rates, and Salvage Management
Despite high success rates (often exceeding 90% in primary cases), the Modified Brostrom-Gould procedure is not immune to complications. A profound understanding of these potential pitfalls is required to mitigate risks and manage adverse outcomes effectively.
Intraoperative and Early Postoperative Complications
The most frequent and frustrating complication is iatrogenic nerve injury, occurring in up to 10% of cases. The superficial peroneal nerve (specifically the intermediate dorsal cutaneous branch) and the sural nerve are highly susceptible to traction neuropraxia from retractors or direct sharp transection. Injury manifests as localized numbness, burning pain, or the development of a painful stump neuroma. Careful surgical technique is the only true prevention. If a nerve is inadvertently transected, it should be buried deep into muscle or bone away from the incision site to prevent symptomatic neuroma formation.
Early postoperative complications include wound dehiscence and superficial infection, which occur in roughly 2-4% of patients. These are typically managed successfully with local wound care and oral antibiotics. Deep space infections are exceedingly rare but require immediate operative irrigation and debridement, and potentially anchor removal if the hardware is seeded. Deep vein thrombosis (DVT) is uncommon in isolated ankle surgery, but appropriate chemical prophylaxis should be considered in high-risk patients or those with a history of hypercoagulability.
Late Complications and Salvage Strategies
Late complications primarily involve recurrent instability or problematic stiffness. Recurrent mechanical instability occurs in 5-10% of patients, often due to premature return to high-impact activities, unaddressed underlying varus malalignment, or poor intrinsic tissue quality. Over-tightening of the repair, conversely, can lead to a loss of subtalar inversion and persistent lateral joint pain.
| Complication | Incidence | Etiology | Salvage Management Strategy |
|---|---|---|---|
| Nerve Injury / Neuroma | 5 - 10% | Iatrogenic traction or transection of SPN or Sural nerve. | Gabapentinoids, diagnostic injections. Surgical excision of neuroma and proximal burying into muscle/bone. |
| Recurrent Instability | 5 - 10% | Trauma, non-compliance, unaddressed fixed varus, poor tissue quality. | Revision anatomic reconstruction with allograft (e.g., semitendinosus) or synthetic augmentation. Concomitant calcaneal osteotomy if varus is present. |
| Subtalar Stiffness | 3 - 5% | Over-tensioning of the CFL or excessive scarring of the retinaculum. | Aggressive physical therapy. Rarely requires arthroscopic or open capsular release. |
| Anchor Pull-out | < 2% | Osteoporotic bone, technical error during placement, early weight-bearing. | Revision surgery with larger diameter anchors, different trajectory, or conversion to a bone-tunnel tenodesis technique. |
When primary anatomic repair fails, salvage strategies must be employed. Historically, non-anatomic tenodeses (Evans, Chrisman-Snook) were utilized, routing the peroneus brevis through fibular tunnels. However, these severely restrict subtalar motion and weaken eversion power. Today, the preferred salvage is an anatomic reconstruction utilizing a free tendon allograft (such as a semitendinosus or gracilis graft) routed through precise osseous tunnels in the talus, fibula, and calcaneus to recreate the ATFL and CFL anatomically.
Phased Post-Operative Rehabilitation Protocols
The success of a lateral ligament reconstruction is as dependent on the postoperative rehabilitation protocol as it is on the surgical execution. The delicate balance between protecting the healing soft tissue and preventing debilitating joint stiffness requires a strictly phased, multidisciplinary approach involving the surgeon, physical therapist, and patient.
Acute Phase and Immobilization
Immediately postoperatively, the ankle is placed in a bulky Jones dressing and a posterior splint, locking the ankle in neutral dorsiflexion and slight eversion. This position completely unloads the newly repaired ATFL and CFL. The patient is instructed to remain strictly non-weight-bearing on the operative extremity for the first two weeks, utilizing crutches or a knee scooter. Elevation above the level of the heart is mandatory to control edema, which can compromise wound healing
