AMPUTATIONS OF THE THUMB
The thumb is the cornerstone of hand biomechanics, contributing to approximately 40% to 50% of overall hand function. Its unique carpometacarpal articulation allows for a wide arc of motion, enabling opposition, key pinch, and power grasp. Consequently, the surgical philosophy governing partial or complete amputations of the thumb differs fundamentally from that of the lesser digits.
In partial amputations of the thumb, reamputation at a more proximal level to obtain primary soft tissue closure must be universally condemned. The thumb should rarely, if ever, be shortened. Preservation of skeletal length is the absolute priority. When primary closure without tension is impossible, the surgical defect must be managed through alternative reconstructive modalities, including free skin grafting, advancement pedicle flaps, or regional/distant flaps.
Soft Tissue Coverage and Flap Selection
When a flap is deemed necessary for coverage of an exposed phalanx or vital structures, donor site selection is critical to functional outcome. Flaps harvested from the dorsum of the hand, or the dorsal aspects of the index or middle fingers, are highly preferable. These regional flaps provide a stable, durable touch pad. However, the surgeon and patient must acknowledge that while mechanical stability is achieved, these flaps do not regain normal tactile sensibility.
Surgical Warning: Covering the volar surface of the thumb with an abdominal pedicle flap is strictly contraindicated. Even when aggressively thinned, abdominal skin and subcutaneous fat provide a biomechanically inferior surface for pinch. Abdominal tissue lacks the specialized vertical fibrous septa (Cleland's and Grayson's ligaments) found in native palmar skin. Consequently, the tissue will roll, shear, or shift under the pressure of pinch and grasp. Furthermore, the aesthetic mismatch between abdominal skin and the native digits is significant.
When severe trauma results in the loss of volar skin and pulp—including all critical neural elements—over a significant area of the thumb, a neurovascular island graft is indicated. In acute settings, the primary defect may be temporarily closed with a split-thickness skin graft to achieve a healed, closed wound. Subsequently, a neurovascular island graft, or a local advancement flap, can be applied as a secondary reconstructive procedure to restore critical sensibility to the ulnar aspect of the thumb pad.
If the thumb has been amputated but a useful, functional segment of the proximal phalanx remains, complex reconstruction may not be required. Aside from primary wound closure, the only adjunctive surgery necessary to maximize function is deepening the first web space via a Z-plasty. This effectively increases the relative length of the thumb, enhancing the depth of the first web space and improving grasp mechanics. Conversely, when amputation occurs at the metacarpophalangeal (MCP) joint or at a more proximal level, formal osteoplastic reconstruction or toe-to-thumb transfer is indicated.
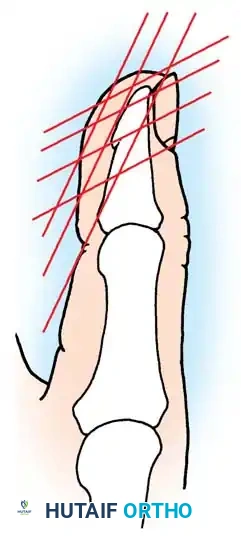
Fig. 14-17 Thumb tip amputation levels and acceptable reconstructive procedures by level: 1, split-thickness graft; 2, cross-finger flap or advancement flap; 3, advancement flap, cross-finger flap, or shorten thumb and close (rarely advised); 4, split-thickness skin graft; 5, shorten bone and split-thickness skin graft, advancement flap, or cross-finger flap; 6, advancement flap or cross-finger flap; 7, advancement flap and removal of nail bed remnant.
ADVANCEMENT PEDICLE FLAP FOR THUMB INJURIES
The volar advancement pedicle flap (often referred to as the Moberg flap) is a workhorse in thumb reconstruction. In the lesser digits, volar advancement flaps are fraught with the risk of dorsal skin necrosis if the volar incisions are extended proximal to the proximal interphalangeal (PIP) joint, due to the disruption of the delicate venous drainage.
However, the vascular anatomy of the thumb provides a distinct surgical advantage. The venous drainage of the thumb is not as strictly dependent on the volar flap. This anatomical variance makes the advancement pedicle technique significantly safer in the thumb, allowing the flap to be designed much longer—often extending to the MCP joint crease—without compromising venous outflow or arterial inflow.
Surgical Technique: Advancement Pedicle Flap
This technique is specifically indicated for deep thumb pad defects where bone, tendon, or neurovascular structures are exposed, and a large area of thumb pulp has been lost.
Clinical Pearl: Meticulous dissection under loupe magnification is mandatory to ensure the neurovascular bundles are included within the flap while preserving the integrity of the flexor pollicis longus (FPL) tendon sheath.
- Preparation and Incision: Under strict tourniquet control and appropriate regional or general anesthesia, design the flap. Make a midlateral incision on both the radial and ulnar sides of the thumb. These incisions should begin at the distal tip of the defect and extend proximally to the level of the metacarpophalangeal (MCP) joint flexion crease.
- Flap Elevation: Carefully elevate the volar flap from distal to proximal. It is imperative that the flap contains both the radial and ulnar neurovascular bundles. The plane of dissection is directly superficial to the flexor tendon sheath.
- Preservation of the Sheath: Do not disturb or incise the flexor tendon sheath (A1, Oblique, and A2 pulleys). Preserving the sheath prevents bowstringing of the FPL tendon and provides a smooth gliding surface.
- Advancement and Closure: Once the flap is fully mobilized to the MCP joint, flex the interphalangeal (IP) and MCP joints of the thumb. This flexion reduces tension, allowing the flap to be advanced distally over the defect.
- Suturing: Carefully suture the advanced flap to the distal nail bed or remaining distal skin using interrupted non-absorbable sutures (e.g., 5-0 or 6-0 nylon). Ensure there is no excessive tension on the skin edges, which could compromise capillary perfusion.
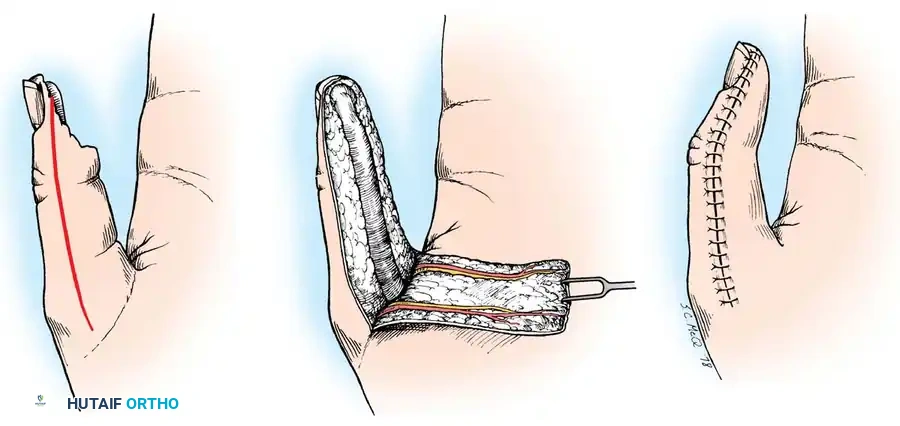
Fig. 14-18 Advancement pedicle flap for thumb injuries. A, Deep thumb pad defects exposing bone can be covered with an advancement pedicle flap. B, Elevation and advancement of the neurovascular pedicle. C, Flexion of the distal joint of the thumb is necessary to permit tension-free placement of the flap.
Postoperative Protocol for Advancement Flaps
Postoperative immobilization is critical to the survival of the flap. The thumb joints (IP and MCP) must be maintained in a flexed position using a dorsal blocking splint for exactly 3 weeks. This prevents tension on the advanced neurovascular bundles and the healing skin edges. After 3 weeks, the splint is removed, and a structured rehabilitation program is initiated to gradually restore active extension and prevent flexion contractures.
AMPUTATIONS OF MULTIPLE DIGITS
The functional devastation of multiple digit amputations requires a highly strategic reconstructive approach. In partial amputations involving all fingers, preserving the absolute maximum remaining length of the digits is exponentially more important than in an isolated single-finger amputation.
The human hand relies heavily on the natural "hinge action" between the first (thumb) and fifth (little finger) metacarpals to achieve cupping of the palm and effective prehension. When the central digits are lost, any remaining stump of the little finger becomes a vital post for the intact thumb to act against.
Enhancing Metacarpal Mobility
To maximize the functional capacity of a severely mutilated hand, the surgeon must focus on relatively lengthening the remaining digits and increasing their mobility.
* Transverse Metacarpal Ligament Release: The natural hinge action of the fifth ray can be increased by approximately 50% simply by surgically dividing the transverse metacarpal ligament between the fourth and fifth rays.
* Web Space Deepening: Function of the thumb is vastly improved by deepening the first web space using a standard or four-flap Z-plasty.
* Metacarpal Osteotomies: In cases where the digits are amputated at the proximal phalangeal or metacarpal neck level, function can be dramatically improved by osteotomizing the first and fifth metacarpals. The distal fragments are rotated toward each other to create a functional pincer mechanism. If advantageous, the fifth metacarpal can also be tilted radially toward the thumb.
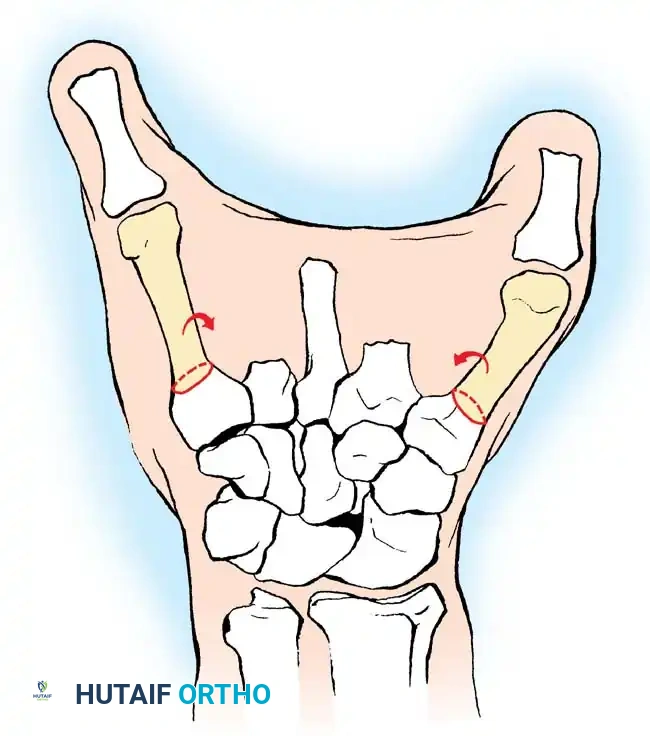
Fig. 14-19 In multiple amputations including the thumb, function can be improved by osteotomizing the first and fifth metacarpals and rotating their distal fragments toward each other to restore prehension.
Metacarpal Transposition and Phalangization
If the first carpometacarpal (CMC) joint remains functional but the first metacarpal shaft is severely shortened, the second metacarpal can be transposed onto the first. This complex osteosynthesis lengthens the thumb ray while simultaneously widening and deepening the first web space.
In the catastrophic event of complete amputation of all fingers at the metacarpophalangeal level, the intact thumb may not be able to easily reach the fifth metacarpal head for opposition. In this scenario, phalangization of the fifth metacarpal is highly beneficial. This procedure involves resecting the fourth metacarpal to liberate the fifth, followed by osteotomy and rotation of the fifth metacarpal to separate it from the central palm, effectively turning it into a mobile, opposable digit.
When amputation has occurred transversely through all metacarpal necks, phalangization of selected metacarpals can salvage function. The fourth metacarpal is resected entirely to increase the range of motion of the fifth. The fifth metacarpal is then osteotomized, with the distal fragment rotated radialward and flexed. The second metacarpal is resected at its base; however, the third metacarpal base is preserved to maintain the origin of the adductor pollicis muscle, which is critical for thumb power.
Surgical Warning: The thumb should not be lengthened by osteoplastic reconstruction (e.g., iliac crest bone graft covered by a tubed pedicle flap) unless protective sensibility can be reliably added to its volar surface via a neurovascular island flap. An insensate thumb post is prone to recurrent ulceration, infection, and eventual resorption.
If the amputation level is through the middle of the metacarpal shafts, restoring true prehension is likely impossible. However, a functional "hook" can be accomplished by utilizing active wrist flexion. This wrist motion can be optimized by fitting the patient with a specialized artificial platform prosthesis to which the palmar surface of the metacarpal stump can actively oppose.
SURGICAL TECHNIQUE: PHALANGIZATION OF THE FIFTH METACARPAL
This procedure effectively converts the forearm and remaining carpus/metacarpus into a biological forceps, where the radial ray (thumb) acts against the mobilized ulnar ray (fifth metacarpal).
- Incision and Exposure: Make dorsal and volar longitudinal incisions over the fourth metacarpal ray, joining them distally over the amputated stump.
- Ligament Release: Deepen the dissection to expose the transverse metacarpal ligament on both the radial and ulnar sides of the fourth metacarpal head. Resect this ligament entirely to free the fifth ray.
- Neurovascular Management: Identify the digital nerves to the ring finger. Divide them sharply under tension as far proximally as possible to allow the stumps to retract deep into the intrinsic musculature, preventing painful neuroma formation. Ligate and divide the corresponding digital vessels.
- Metacarpal Resection: Dissect the interosseous muscles away from the fourth metacarpal. Resect the entire fourth metacarpal shaft just distal to its carpometacarpal joint.
- Fifth Metacarpal Osteotomy: Through the same surgical exposure, perform a transverse or slightly oblique osteotomy of the fifth metacarpal near its base.
- Realignment and Fixation: Slightly abduct and flex the distal fragment of the fifth metacarpal, rotating it radially toward the thumb to optimize opposition. Fix the osteotomy securely with crossed Kirschner wires or a low-profile mini-fragment plate.
- Soft Tissue Reconstruction: The resection of the fourth ray creates a large dead space and raw surfaces between the third and fifth metacarpals. Cover these raw surfaces meticulously with thick split-thickness skin grafts or full-thickness grafts, creating a new, deep web space at the junction of the proximal and middle thirds of the remaining bones.
- Padding and Sensibility: Ensure that the soft tissue padding over the newly positioned fifth metacarpal head is robust. It is paramount that the skin at the point of maximal contact with the thumb possesses normal sensation to allow for effective, blind prehension.
Postoperative Considerations and Outcomes
Following phalangization, the hand is immobilized in a bulky dressing and splint until the osteotomy achieves clinical union (typically 4 to 6 weeks) and the skin grafts have fully taken. Kirschner wires are removed once radiographic union is confirmed.
The functional outcomes of this procedure can be profound. Swanson famously compared the function of this reconstructed, two-pronged limb to the adept use of chopsticks. Because native skin is shifted during closure, normal sensibility between the tips of the newly created rays is preserved.
This operation is exceptionally valuable in blind patients with bilateral amputations, as it restores not only mechanical prehension but also vital tactile sensibility at the terminal parts of the limb—something a mechanical prosthesis cannot provide. It is also highly recommended in environments where access to modern, myoelectric prosthetic services is unavailable or economically unfeasible.
