Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 17-year-old boy has had a mass in his right thigh for the past 6 months. He denies any history of trauma. Examination reveals that the mass is painless and firm. A radiograph and axial MRI scan are shown in Figures 49a and 49b. What is the most likely diagnosis?


Explanation
Osteochondroma typically occurs as a bony projection or a sessile growth on the bone, and there can be flaring of the metaphysis. The radiograph shows continuity from the adjacent cancellous bone into the lesion itself. There is no soft-tissue mass or bone destruction to suggest osteosarcoma or Ewing's sarcoma. Periosteal chondroma has a scalloped out radiographic appearance. Chondroblastoma typically is an epiphyseal-based lesion.
Question 2
Which of the following statements describing chordomas is false?

Explanation
Casali and associates provided a recent review of the treatment options for chordomas. These tumors are not radiosensitive; however, modern intensity modulated radiosurgery techniques may be of value. The combination of surgery and radiotherapy compared to surgery alone results in the same disease-free survival time. Complete surgical resection of the chondroma with clean margins offers the best survival; however, its location may make total removal impossible. Thus subtotal resection followed by radiotherapy results in better survival despite the tumor's lack of radiosensitivity.
Question 3
A 68-year-old man reports a 1-year history of debilitating neck pain without neurologic symptoms. History reveals a C5-6 anterior diskectomy and bone grafting 10 years ago that provided good relief of arm and neck pain. Radiographs show evidence of fibrous union at C5-6, spondylotic disk narrowing at C4-5 and C6-7, and a fixed 2-mm subluxation at C3-4. Examination reveals cervical stiffness and discomfort at the extremes of movement. His neurologic examination is normal. Treatment should now consist of

Explanation
Axial pain can be difficult to manage. Pain management is not always successful, and surgical approaches may provide disappointing results unless there is discrete pathology. Whereas planning of a surgical approach should consider prior approaches and preexisting laryngeal dysfunction, no compelling case for surgical intervention can be made for this patient. Therefore, management should consist of patient education, exercise, and nonnarcotic medication. Ahn NU, Ahn UM, Andersson GB, et al: Operative treatment of the patient with neck pain. Phys Med Rehabil Clin N Am 2003;14:675-692. Algers G, Pettersson K, Hildingsson C, et al: Surgery for chronic symptoms after whiplash injury: Follow-up of 20 cases. Acta Orthop Scand 1993;64:654-656.
Question 4
The sartorius muscle is innervated by which of the following nerves?

Explanation
The femoral nerve enters the thigh behind the inguinal ligament, lying on the surface of the iliopsoas muscle lateral to the femoral artery and vein. The nerve divides into numerous muscular and cutaneous branches in the femoral triangle. The first motor branch (sometimes two branches) is to the sartorius. There is a variable branch to the pectineus. Subsequent branches go to the rectus femoris and then the vastus muscles in variable order. The last motor branch is to the articularis genu. The muscular branches can be injured in anterior approaches to the hip, especially the middle window of the ilioinguinal approach. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 404.
Question 5
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?


Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 6
Figure 42 shows the radiograph of a 70-year-old woman who has had a painful near ankylosis of her dominant elbow for 1 year. Treatment should consist of

Explanation
The patient has arthritis and supracondylar nonunion of the elbow. Total elbow replacement has been shown to give almost immediate return of function as it can be performed while leaving the triceps intact and resecting the distal humerus fragment. Attempts at osteosynthesis are indicated in younger individuals with good joint surface. Resection arthroplasty yields poor function and is reserved as a salvage procedure. Ramsey ML, Morrey BF: Total elbow arthroplasty for nonunion and dysfunctional instability, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Question 7
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Question 8
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
Symptoms of activity-related low back pain, physical findings of pain with extension, lateral bending, and resuming an upright position, and relative hamstring tightness are consistent with spondylolysis. While the initial diagnostic work-up should include plain radiographs of the lumbosacral spine, the findings may be negative because it can take weeks or months for the characteristic changes to become apparent. SPECT has been a useful adjunct in the diagnosis of spondylolysis when plain radiographs are negative. Since the patient's pain is activity related and she is otherwise healthy, evaluation for infection is not indicated. Because the neurologic examination is normal, electromyography, nerve conduction velocity studies, and MRI are not indicated. CT can be used in those instances in which SPECT and bone scans are negative. Ciullo JV, Jackson DW: Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clin Sports Med 1985;4:95-110. Collier BD, Johnson RP, Carrera GF, et al: Painful spondylolysis or spondylolisthesis studied by radiography and single photon emission computed tomography. Radiology 1985;154:207-211. Jackson DW, Wiltse LL, Cirincione RT: Spondylolysis in the female gymnast. Clin Orthop 1976;117:68-73.
Question 9
In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?

Explanation
Acetabular cage reconstruction is indicated in severe disruption of acetabular bone stock when a cementless acetabular component cannot be stabilized in intimate contact with a sufficient bed of structurally sound and viable host bone, with or without a structural graft. Cages are used in pelvic discontinuity where they provide a bridge between the ilium and the ischium, while supporting a cemented cup. All of the other scenarios are amenable to achieving an adequate rim fit for a cementless component, using a jumbo cup if necessary. Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Question 10
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?



Explanation
The incidence of osteonecrosis following displaced talar neck fractures is most related to the extent of initial fracture displacement. With increasing fracture displacement, the tenuous vascular supply to the talar body is more at risk for damage, thereby increasing the risk of osteonecrosis. Although displaced talar neck fractures have historically been considered a surgical emergency, recent studies have shown that the timing of surgical intervention bears no impact on the development of osteonecrosis. While nicotine use has an influence on fracture healing, it has never been shown to be a factor in osteonecrosis, nor has posterior-to-anterior screw fixation or the quality of fracture reduction. Lindvall E, Haidukewych G, Dipasquale T, et al: Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am 2004;86:2229-2234.
Question 11
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?

Explanation
Recovery of upper extremity motor function after a cerebrovascular accident follows a predictable pattern. The greatest amount of recovery is seen within the first 6 weeks. Return of function proceeds from proximal to distal. Shoulder flexion occurs first, followed by return of flexion to the elbow, wrist, and fingers. Return of forearm supination follows the return of finger flexion.
Question 12
A 26-year-old rugby player injured his foot when tackled from behind. Radiographs are seen in Figures 35a through 35c. What is the most appropriate treatment?



Explanation
The patient has a ligamentous Lisfranc injury. Diastasis seen between the bases of the second metatarsal and medial cuneiform is pathognomonic for a rupture of the Lisfranc's ligament. This injury is best treated surgically with either open reduction and internal fixation or possibly closed manipulation and percutaneous screw fixation if anatomic alignment can be achieved closed. Pin fixation has been shown to be inferior to screw fixation due to the length of time that fixation is required for adequate ligament healing. Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries of the tarsometatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 13
Chronic anterior donor site pain following the harvest of autologous iliac crest bone graft for use during anterior cervical diskectomy and fusion is reported by approximately what percent of patients?
Explanation
Four years after surgery, more than 90% of patients are satisfied with the cosmetic appearance of the iliac donor site scar. Approximately 25% still have pain and/or functional difficulty, including 12.7% who still report difficulty with ambulation, 11.9% difficulty with recreational activities, 7.5% with sexual intercourse, and 11.2% require pain medication for iliac donor site symptoms. Silber JS, Anderson DG, Daffner SD, et al: Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion. Spine 2003;28:134-139.
Question 14
In the treatment of acetabular dysplasia, what type of pelvic osteotomy leaves the "teardrop" in its original position and redirects the acetabulum?

Explanation
The dial or spherical osteotomy leaves the medial wall or teardrop in its original position and, as a result, is intra-articular. The other pelvic osteotomies (except Chiari) redirect the acetabulum, including the medial wall. The Chiari osteotomy improves coverage without redirecting the acetabulum within the pelvis, and it leaves the teardrop in the same place. Lack W, Windhager R, Kutschera HP, Engel A: Chiari pelvic osteotomy for osteoarthritis secondary to hip dysplasia: Indications and long-term results. J Bone Joint Surg Br 1991;73:229-234. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 15
Figure 31 shows the radiograph of an 8-year-old boy who has a swollen forearm after falling out of a tree. Examination reveals that all three nerves are functionally intact, and there is no evidence of circulatory embarrassment. Management should consist of

Explanation
The patient has a Bado type IV Monteggia lesion. It involves dislocation of the radial head and fractures of both the radial and ulnar shafts. These fractures are very difficult to manage by closed reduction alone. The radial and ulnar shafts first have to be stabilized surgically to give a lever arm to reduce the radial head. In this age group, intramedullary pins are easy to insert percutaneously and cause less tissue trauma than plates and screws. In these types of injuries, the focus is often on the forearm fracture; the radial head dislocation may not be appreciated as was the case with this patient. Gibson WK, Timperlake RW: Operative treatment of a type IV Monteggia fracture-dislocation in a child. J Bone Joint Surg Br 1992;74:780-781.
Question 16
A 3-year-old child has bilateral genu varum and short stature. Radiographs show physeal widening and generalized osteopenia. The femora and tibiae show anterolateral bowing. Laboratory studies show low normal serum calcium values, significantly decreased serum phosphate levels, and normal parathyroid hormone (PTH), alkaline phosphatase, and vitamin-D levels. These findings are consistent with
Explanation
Children with vitamin D-resistant rickets are short in stature and have genu varum, physeal widening, and generalized osteopenia. The abnormality in inherited vitamin D-resistant rickets is the renal tubule's inability to resorb phosphate leading to hypophosphatemia. Laboratory findings in the condition are normal or near normal serum calcium values, significantly decreased serum phosphate levels, elevated alkaline phosphatase levels, and normal PTH and vitamin-D levels. The most common form is inherited as an X-linked dominant trait. Nutritional rickets has a normal or low serum phosphate levels, normal or low serum calcium values, and decreased levels of 25(OH) vitamin D and 1,25-dihydroxyvitamin D. Hypophosphatasia is a rare condition characterized by a deficiency of alkaline phosphatase in the serum and tissues, leading to generalized abnormal mineralization of bone. Primary hyperparathyroidism usually is caused by a parathyroid adenoma, and the child generally has abdominal problems and hypercalcemic crisis. Laboratory findings include elevated serum calcium values, alkaline phosphatase levels, and PTH levels, and decreased serum phosphate levels. Children with renal osteodystrophy tend to have genu valgum, and laboratory findings include elevated serum phosphate, alkaline phosphatase, and PTH levels, and low serum calcium values. Findings of renal disease include elevated BUN and creatinine. Herring JA: Metabolic and endocrine bone diseases, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1686-1710.
Question 17
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in

Explanation
The surface hardness of titanium is low compared with that of cobalt-chromium alloys. Titanium articulations are easily scratched, resulting in a significantly increased rate of wear and debris production. The wear and resulting lysis can also result in an increased rate of loosening. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Question 18
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?

Explanation
The infant has a well-positioned hip in the Pavlik harness and treatment should be continued in the current position. The success rate is over 90% with the use of this device for a dislocatable hip. Ultrasound is a useful tool to confirm appropriate positioning of the cartilaginous femoral head during treatment. If the femoral head is not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 19
What joint always remains uninvolved in all stages of scapholunate advanced collapse (SLAC) deformity of the wrist?
Explanation
The development of arthritis in SLAC wrist follows a consistent pattern. Beginning at the radial styloid to the scaphoid articulation, it progresses through the entire radioscaphoid joint and the midcarpal joint. In all stages, the radiolunate joint is spared, which is the basis for a scaphoid excision and four-corner fusion performed as a motion-sparing procedure for treatment of this condition. Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281. Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Question 20
Figure 36 shows the radiograph of a patient who has hip pain and is unable to ambulate. What is the most appropriate management for this patient?

Explanation
The patient has a periprosthetic fracture of the greater trochanter - Vancouver A. The reason for the fracture of the greater trochanter is the extensive periarticular osteolysis that has occurred as a result of polyethylene wear. The latter is demonstrated by eccentric seating of the large femoral head in the acetabulum. The most appropriate management is to reverse the osteolysis process, which involves exchange of the acetabular liner with or without revision of the other components depending on their fixation and position. The greater trochanter can also be fixed during revision surgery. Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Question 21
A patient underwent anterior stabilization of the shoulder 6 months ago, and examination now reveals lack of external rotation beyond 0 degrees. The patient has a normal apprehension sign and normal strength, and the radiographs are normal. Based on these findings, the patient is at greater risk for the development of

Explanation
Because the patient's shoulders are overtensioned anteriorly, premature osteoarthritis may develop. This may create obligate translation posteriorly and increase the interarticular pressure of the humeral head against the glenoid. Patients should achieve 20 degrees to 30 degrees of external rotation with the elbow at the side. Late degenerative arthritis following a Putti-Platt procedure is associated with significant restriction of external rotation. This patient's shoulder has a reduced risk of anterior instability, rotator cuff tear, and internal impingement because of the limitation of motion. Hawkins RJ, Angelo RL: Glenohumeral osteoarthritis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 22
The load versus deformation curve of the functional spinal unit (FSU) is made up of the neutral zone, the elastic zone, and the plastic zone. What is the plastic zone of the curve believed to represent?
Explanation
Plastic deformation of viscoelastic tissues represents deformation of the soft tissues to the point of failure. The lining up of collagen fibers would be in the "toe region" of the curve, which, in the case of the FSU, would be mainly in the neutral zone. Elastin is a minor contributor to the composition of the ligaments and would be protected by the stiffer collagen fibers. The transition between flexion and extension occurs in the neutral zone, and reversible elongation occurs in the elastic zone. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 15-23.
Question 23
A 40-year-old carpenter has a 3-month history of right arm pain and neck pain that now leaves him unable to work. Examination reveals a positive Spurling test, weakness of the biceps, and a mildly positive Hoffman's sign on the right side. Electromyography and nerve conduction velocity studies show a right C6 deficit. Figures 27a through 27c show MRI scans that reveal two-level spondylotic disease at C5-6 and C6-7, a large herniated nucleus pulposus at C5-6, and a prominent ridge and hard disk at C6-7. Nonsurgical management fails to provide relief, so the patient elects surgical intervention. Which of the following surgical options would give the best long-term results?



Explanation
The patient has a single-level deficit by clinical examination but an adjacent level that may be pathologic. Hilibrand and associates, in a review of 374 patients with myeloradiculopathy treated with single-level or multilevel anterior cervical diskectomy and fusion, showed that 25% of patients had an occurrence of new radiculopathy or myelopathy at an adjacent level within 10 years after surgery. Reoperation rates were highest in those patients where the adjacent nonfused segment was C5-6 or C6-7. Those patients who had multilevel fusions had a lower incidence of adjacent segment disease. The authors recommended incorporating an adjacent level in the initial procedure in patients with myelopathy or radiculopathy when significant disease was noted. Posterior keyhole foraminotomy is an excellent procedure for single-level radiculopathy but is not effective in relieving myelopathy. Anterior cervical diskectomy without fusion has an increased incidence of hypermobility and neck pain on long-term follow-up. In a later review, these authors reported improved fusion rates and better clinical outcomes with the use of strut fusions instead of multilevel interbody grafts. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH: Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519-528. Henderson CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Question 24
Which of the following lesions most closely resembles Ewing's sarcoma histologically?
Explanation
Ewing's sarcoma is characterized by small round blue cells. Lesions with a similar appearance include lymphoma, primitive neuroectodermal tumor, rhabdomyosarcoma, small cell lung tumor, and metastatic neuroblastoma. Karyotyping, immunohistochemistry, and electron microscopy can help differentiate these lesions.
Question 25
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
Injury to the sciatic nerve is a relatively rare but serious complication of THA. Dissection of the sciatic nerve is not typically done during primary THA, although the nerve can be identified during the surgical approach. An anterolateral approach to THA would not necessarily be associated with any greater incidence of sciatic nerve injury than other approaches. Screw fixation for the acetabular component is often a matter of surgeon preference. Provided that the anatomic safe zones for screw fixation (posterior inferior and posterior superior) are recognized, injury to the sciatic nerve from acetabular screws can be minimized. Restoration of anatomic length is important in primary THA. Overlengthening can result in sciatic nerve palsy. Developmental dysplasia of the hip can lead to a congenitally shortened extremity with concomitant congenital shortening of the associated neurovascular structures. Overlengthening of the extremity during THA for developmental dysplasia of the hip can lead to sciatic palsy. Osteonecrosis is not an associated risk factor for sciatic nerve palsy. DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
Question 26
An 18-month-old child sustains a crush amputation of the tip of the index finger. Bone is exposed, but the nail is intact. Management should consist of

Explanation
Children have a much greater capacity to heal soft-tissue injuries than adults. Most crush or avulsion fingertip amputations in children, particularly those younger than age 2 years, can be treated with serial dressing changes, even with bone exposed. Das SK, Brown HG: Management of lost finger tips in children. Hand 1978;10:16-27.
Question 27
Which of the following describes the correct proximal to distal progression of the annular and cruciform pulleys of the digits?
Explanation
The correct progression of the annular and cruciform pulley in the digits is A1, A2, C1, A3, C2, A4, C3. The two cruciform pulleys are collapsible elements adjacent to the more rigid annular pulleys of the flexor tendon sheath. This arrangement enables unrestricted flexion of the proximal interphalangeal joint. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Question 28
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
In Charcot-Marie-Tooth disease, the posterior tibialis and peroneus longus tendons remain strong, serving to invert the hindfoot and depress the first metatarsal head thus causing the cavovarus foot associated with this disease. In contrast, the tibialis anterior and peroneus brevis are less functional and therefore cannot dorsiflex the ankle, elevate the first metatarsal, or evert the foot, contributing to the deformity.
Question 29
A 64-year-old man who underwent an L4-5 decompression approximately 1 year ago reported relief of his claudicatory leg pain initially, but he now has increasing low back pain and recurrent neurogenic claudication despite nonsurgical management. Radiographs show new asymmetric collapse and spondylolisthesis at the decompressed segment, and MRI scans show lateral recess stenosis. The next most appropriate step in management should consist of

Explanation
When radiographic findings reveal postlaminectomy instability, procedures that do not include some type of fusion will fail to solve the problem. In fact, wider decompression or diskectomy alone will only further destabilize the segment. Because there is radiographic evidence of recurrent lateral recess stenosis and symptomatic neurogenic claudication, a revision decompression should be included. Since access to the canal involves a posterior approach, the stabilization should be performed through that same approach. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
Question 30
An olecranon fracture-dislocation of the elbow in which the fracture line exits distal to the coronoid process is best managed by open reduction and
Explanation
Fracture-dislocations of the elbow present difficult management problems. Standard olecranon fractures normally are not associated with a dislocation; however, the surgeon needs to recognize that some fractures that have a dislocation, in particular a posterior dislocation, represent a Monteggia equivalent. These injuries are not ulnar shaft fractures because they are fractured at or just distal to the coronoid; however, because of the unstable fracture-dislocation, the forces across this reduction are high. Two Kirschner wires and a tension band wire provide inadequate fixation. Therefore, the preferred method of fixation is plate osteosynthesis with a 3.5-mm low-contact dynamic compression plate or reconstruction plate. Jupiter JP, Kellam JF: Fractures of the forearm, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 421-454. Quintero J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Question 31
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?

Explanation
Instability is a leading cause of failure following total knee arthroplasty. Instability can present as global instability, extension gap (varus/valgus) instability, or flexion gap (anterior/posterior) instability. Treatment options are numerous based on the exact pathology. The radiograph reveals anterior/posterior instability with dislocation consistent with flexion gap instability. A loose flexion gap can allow the femoral component to ride above the tibial cam post mechanism, resulting in dislocation. Distal femoral augments treat extension gap instability, whereas tibial augments can treat both flexion and extension gap instability. Posterior condyle augments at the distal femur can also be used to treat flexion gap instability. Flexion gap instability is further aggravated by extension mechanism incompetence. Note the excessively thin patella on the lateral radiograph. Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.
Question 32
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to

Explanation
The arrow identifies a transverse dark line that represents primary trabeculae of the physeal scar. A similar finding is seen in the proximal tibia. These lines may persist indefinitely. They do not represent ongoing growth, an abnormally open physeal plate, a stress fracture, or Looser's line (fatigue fracture in osteomalacia).
Question 33
A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotation. Plain radiographs are normal, and an MRI scan is shown in Figure 21. Management should consist of

Explanation
A stress fracture of the hip is a relatively common problem in endurance sports. These fractures are classified as compression-side, tension-side, and displaced femoral neck fractures. The MRI scan shows a compression-side stress fracture. Compression-side fractures usually occur in the inferior or calcar area of the proximal femur, and non-weight-bearing crutch ambulation for 6 to 7 weeks will most likely result in healing. Once the patient is walking without pain or a limp, activities can be slowly increased. Because tension-side fractures have a high risk of displacement, treatment should consist of immediate internal fixation. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 239-253.
Question 34
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?


Explanation
The radiographs reveal a predominantly lytic, destructive lesion of the distal femur, although there is a hint of some blastic change as well. The lesion has violated the cortex, and there is mineralization outside the cortex laterally. The lateral radiograph suggests a soft-tissue density. These aggressive changes on radiographs in this age group are strongly suggestive of osteosarcoma. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 35
Which of the following is considered the most useful screening method for the evaluation of protective foot sensation in a patient with diabetes mellitus?
Explanation
Patients with diabetes mellitus should be screened for the presence of protective foot sensation. In the absence of protective foot sensation, patients are at increased risk for the development of neuropathic ulcerations and neuropathic arthropathy. The most reliable screening tool for the presence of protective sensation is the ability to feel the 5.07 Semmes-Weinstein monofilament. Pinzur MS, Shields N, Trepman E, Dawson P, Evans A: Current practice patterns in the treatment of Charcot foot. Foot Ankle Int 2000;21:916-920.
Question 36
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15 degrees of valgus, and forefoot supination can be corrected to 10 degrees from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of

Explanation
The most important determining factor for correction of an adult flatfoot without an arthrodesis is the flexibility of the subtalar and transverse tarsal joints. Rigid deformities cannot be corrected with a medial sliding calcaneal osteotomy with FDL transfer or a subtalar arthroereisis. Isolated subtalar or talonavicular arthrodesis does not correct the deformities entirely. If the patient has forefoot supination that can be corrected to less than 7 degrees, an isolated subtalar fusion is a possible alternative.
Question 37
Figures 5a and 5b show the radiograph and MRI scan of a patient who has severe mechanical neck pain but no neurologic problems. Biopsy and work-up show the lesion to be a solitary plasmacytoma. Treatment should consist of


Explanation
Plasmacytoma is very sensitive to radiation therapy and given the complexity of the resection and complications of surgery in the given location, radiation therapy is preferred. However, the patient has clear loss of bony structural integrity, and resultant instability would persist even with tumor irradiation; therefore, posterior stabilization is warranted. Chemotherapy and bone marrow transplant are reserved for systemic disease with multiple myeloma. Corwin J, Lindberg RD: Solitary plasmacytoma of bone vs. extramedullary plasmacytoma and their relationship to multiple myeloma. Cancer 1979;43:1007-1013.
Question 38
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
In the adolescent population, a lumbar herniated disk is characterized by a paucity of clinical findings, with a positive straight leg raising test the only consistently positive finding. This may result in a prolonged period of nonsurgical management that fails to provide relief. Activities that place a significant shear load on the lumbar spine, such as the dead lift, are associated with an increased risk of central disk herniation. An adolescent who lifts weights and has a history of back pain that fails to respond to a short period of active rest should undergo MRI evaluation for the diagnosis of a lumber herniated disk. Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Question 39
A 45-year-old man reports right shoulder pain with overhead activities only. Figures 47a through 47d show the radiographs, bone scan, and MRI scan of a lesion of the proximal shoulder. What is the most appropriate treatment?




Explanation
The figures show a lesion of the proximal humerus consistent with an enchondroma. The lesion is calcified on the radiographs. There is no cortical destruction, significant endosteal scalloping, or soft-tissue mass. The bone scan shows mild uptake in the area of the proximal humerus, and the T2-weighted MRI scan shows a lesion with high uptake, suggesting a lesion with high water content. A CT scan could also be obtained to rule out bone destruction or periosteal reaction. Pain with overhead activities is likely related to the rotator cuff. A biopsy is unlikely to add information because of inherent difficulties interpreting low-grade cartilaginous lesions. Curettage and grafting and en bloc resection are excessive treatments for a benign lesion that is apparently asymptomatic. Observation with a follow-up radiograph in 3 to 6 months is appropriate. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 40
A 47-year-old woman has had medial ankle pain and swelling for the past 3 months. She recalls no specific injury, and casting and nonsteroidal anti-inflammatory drugs have failed to provide relief. Examination reveals a pes planus with heel valgus that is passively correctable. Radiographs show no evidence of arthritis. An MRI scan is shown in Figure 16. What is the most appropriate surgical procedure to alleviate her pain?

Explanation
The patient has a stage II posterior tibial tendon tear with a supple foot; therefore, the treatment of choice is flexor digitorum longus transfer with medial displacement calcaneal osteotomy. Triple arthrodesis is not indicated, and isolated tendon transfer will stretch out in the face of persistent heel valgus. Direct repair of the posterior tibial tendon or repair of the spring ligament is not sufficient to correct the deformity. Myerson MS, Corrigan J: Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon transfer and calcaneal osteotomy. Orthopedics 1996;19:383-388.
Question 41
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
Lateral scapular winging is characteristic of trapezius palsy, whereas medial scapular winging is characteristic of long thoracic nerve palsy. During sports activity, injury to the spinal accessory nerve is rare but may occur with blunt or stretching trauma. Patients often report an asymmetric neckline, drooping shoulder, winging of the scapula, and weakness of forward elevation. Evaluation should include a complete electrodiagnostic examination. Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16. Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27. Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546. Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Question 42
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?

Explanation
The injury shown is a fracture-dislocation and it is highly unstable. In addition to this concern, spinal epidural hematomas have a much higher incidence in people with ankylosing spondylitis following knee fracture. It is felt to be due to disrupted epidural veins, with hypervascular epidural soft tissue in the setting of a rigid spinal canal. Patients with ankylosing spondylitis may have other significant comorbidities, especially cardiac and pulmonary, and these should be carefully assessed. Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004, pp 279-290.
Question 43
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
V-Y advancement flaps are ideal for fingertip amputations that are transverse or dorsal oblique in nature. Healing by secondary intention is contraindicated with exposed bone. Shortening of exposed bone to allow primary skin closure is a possible alternative, as long as significant shortening of the index finger is avoided. A Moberg flap is useful only for distal amputations of the thumb. The first dorsal metacarpal artery-island pedicled flap uses tissue from the dorsum of the proximal index finger, and is typically used to resurface defects of the thumb. Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 44
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
Locked plating is becoming more common. Some biomechanical data comparing locked plating to standard plating have been reported for osteoporotic distal femoral fractures and humeral shaft fractures. Significant differences were seen mainly for osteoporotic fractures without cortical contact. Not all osteoporotic fractures and all comminuted fractures have been shown to demonstrate significant mechanical improvement with locked plating compared to standard plating. Spiral fractures often can be repaired with a lag screw, obtaining adequate cortical contact. Osteoporotic fractures with a torsion mode of failure failed earlier with locked plating systems than with standard plating systems. Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Question 45
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?

Explanation
Wear in total hip arthroplasty is a very complex phenomenon. The radial mismatch of the femoral head to the acetabular component has been shown in multiple studies to be a significant factor in wear. The mismatch can neither be too small nor too large. When the mismatch is too small, seizing of the implants can occur. When the mismatch is too large, contact stresses increase and produce exceptionally high wear. The ideal radial mismatch should be approximately 50 microns. Surface roughness and ball sphericity are two items that are extremely important with respect to wear. High carbon content has been shown to decrease wear. This device has a very large head-to-neck ratio, so impingement-related wear is unlikely. Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34. Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.
Question 46
What is the most common secondary malignancy arising in pagetic bone?

Explanation
The incidence of malignant transformation or the formation of a secondary malignancy in pagetic bone is estimated to be less than 1%. Osteosarcoma is the most common secondary malignancy, followed by fibrosarcoma and chondrosarcoma. Ewing's sarcoma arising in pagetic bone has not been reported. Grimer RJ, Carter SR, Tillman RM, et al: Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81:796-802.
Question 47
Which of the following properties apply to the human meniscus when compared with articular cartilage?

Explanation
The meniscal cartilage, like articular cartilage, possesses viscoelastic properties. The extracellular matrix is a biphasic structure composed of a solid phase (collagen, proteoglycan) that acts as a fiber-reinforced porous-permeable composite, and a fluid phase that may be forced through the solid matrix by a hydraulic pressure gradient. Although these properties are shared with articular cartilage, the meniscus is more elastic and less permeable than articular cartilage. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
Question 48
Which of the following best describes the function of the notochord?
Explanation
The notochord is the anatomic structure that defines the phylum Chordata. The notochord plays a fundamental role in the development of the skeleton, and it exists only for a short period of time. During its temporary existence, the notochord serves as a transient axis of support, provides for the initial axis of orientation of the developing embryo, and most importantly, plays a vital role in the induction of the tissues that eventually form the vertebral column.
Question 49
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?


Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 50
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of


Explanation
Open reduction and internal fixation of distal humeral fractures in elderly patients often fails. These fractures characteristically have a very small distal segment and poor bone quality, resulting in failure of fixation and nonunion. Nonunion is often painful and functionally debilitating. Total elbow arthroplasty provides good results when used for distal humeral fractures in elderly patients with osteopenic bone and fracture patterns thought to be irreconstructable. Long arm casting may result in union, but the resulting stiffness is unacceptable for an active patient. Elbow arthrodesis has few indications. A sling and range-of-motion exercises will often result in a painful and debilitating nonunion at the fracture site. Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Question 51
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?

Explanation
The presence of synchronous bone disease in young patients carries a dismal prognosis, one that is even worse than the presence of resectable pulmonary metastasis. Many osteosarcomas cross the physis; therefore, this has not been shown to be of prognostic importance. Similarly, the presence of the soft-tissue mass has less prognostic significance.
Question 52
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?


Explanation
The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Question 53
Figures 45a through 45c show the radiograph, CT scan, and MRI scan of a 15-year-old boy who has lateral ankle pain. What is the most likely diagnosis?



Explanation
The elongated anterior process of the calcaneus reaching distally toward the navicular is an abnormal finding. Instead of viewing the rounded, blunt distal anterior process of the calcaneus, a bridge extends to the navicular, albeit incomplete. These findings are consistent with a fibrous coalition. CT can reveal a stress fracture of the calcaneus, arthritis of the subtalar joint with subchondral cysts, or an os peroneal bone disruption in the peroneus longus, but those entities are not shown here. The plantar fascia is intact. Richardson EG: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 702-732.
Question 54
The dose of the chemotherapeutic agent doxorubicin (Adriamycin) is limited by which of the following factors?

Explanation
Doxorubicin is a chemotherapeutic agent that is best known for dose-limiting cardiotoxicity. This is related not only to the cumulative dose, but also the rate of infusion.
Question 55
In children with isolated zone II lacerations of the flexor tendon, poor digital motion is best correlated with
Explanation
In a recent study on restoration of motion following zone I and zone II flexor tendon repairs in children, age was found to have no effect on the results of zone II tendon repairs. Early passive motion offered no better results than immobilization for 3 weeks. Immobilization for more than 4 weeks correlated with poorer results.
Question 56
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of

Explanation
The radiograph reveals posterolateral rotatory subluxation of the radiohumeral and ulnohumeral joints. The space between the ulna and trochlea is enlarged, particularly posteriorly at the olecranon. These findings are diagnostic of posterolateral rotatory instability, which causes recurrent subluxation and reduction as the elbow is flexed from an extended and supinated position with valgus load. The posterolateral rotatory instability apprehension test was performed on this patient and the result was positive. The lateral pivot-shift test causes a clunk as the elbow reduces but is more difficult to perform, even under general anesthesia. The patient does not have isolated subluxation of the radial head, although these findings can be mistakenly diagnosed as such. The radial head is normally shaped and does not represent a congenital dislocation. There are no findings here to suggest osteochondritis dissecans or loose bodies. O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446. Burgess RC, Sprague HH: Post-traumatic posterior radial head subluxation: Two case reports. Clin Orthop 1984;186:192-194.
Question 57
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?

Explanation
The modified Hardinger approach includes a partial anterior trochanteric osteotomy creating a trochanteric wafer (as seen on the radiograph) that is displaced anterior and medial in continuity with the gluteus medius and vastus lateralis. Failure of abductor reattachment, migration of the trochanter, nonunion of the osteotomy site, and excessive splitting of the gluteus medius muscle causing injury to the inferior branch of the superior gluteal nerve can result in weakness of the abductor mechanism. Abductor strength should be evaluated with the patient lying on the opposite side and elevating the affected limb. Although slight weakness may manifest itself as a limp only after prolonged muscular activity, significant weakness results in a constant limp without associated discomfort. Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
Question 58
What structure provides the most static stability for valgus restraint in the elbow?
Explanation
The anterior band of the ulnar collateral ligament provides the greatest restraint to valgus stress in the elbow. The posterior band is taut in flexion and resists stress between 60 degrees and full flexion. The annular ligament stabilizes the radial head. The flexor/pronator mass are important dynamic stabilizers of the medial elbow. Ahmad CS, ElAttrache NS: Elbow valgus instability in the throwing athlete. J Am Acad Orthop Surg 2006;14:693-700. Regan WD, Korinek SL, Morrey BF, et al: Biomechanical study of ligaments around the elbow joint. Clin Orthop Relat Res 1991;271:170-179.
Question 59
A 57-year-old man with type II diabetes mellitus was successfully treated for a first occurrence forefoot full-thickness (Wagner II) diabetic foot ulcer underlying the third metatarsal head with associated hammertoe with a series of weight-bearing total contact casts. There was no evidence of osteomyelitis. The ulcer is now fully healed. He is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. What is the next most appropriate step in management?

Explanation
This is the first occurrence of diabetic foot-specific morbidity. The patient has a foot deformity, a history of a diabetic foot ulcer, and is insensate to the monofilament. He is at moderate risk for the development of a recurrent ulcer. This is best avoided with therapeutic footwear. Commercially available depth-inlay shoes should be combined with a custom accommodative foot orthosis to accommodative the deformity. Pinzur MS, Slovenkai MP, Trepman E, et al: Guidelines for diabetic foot care: Recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int 2005;26:113-119.
Question 60
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Explanation
The elbow usually is stable after reduction in most elbow dislocations. Ross and associates reported that supervised motion begun immediately after reduction was effective in uncomplicated dislocations. The elbow will become stiff if immobilization is applied for an extended period of time. Immediate open treatment is not indicated for a simple elbow dislocation. Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
Question 61
Arthrodesis of which of the following joints has the greatest cumulative effect on midfoot/hindfoot motion?
Explanation
Arthrodesis of the talonavicular joint eliminates almost all hindfoot motion. Arthrodesis of the subtalar joint eliminates 74% of talonavicular motion and 44% of calcaneocuboid motion. Arthrodesis of the calcaneocuboid joint eliminates 33% of talonavicular motion and 8% of subtalar motion. Arthrodesis of the naviculocuneiform or cuboid-fifth metatarsal joint has limited effect on hindfoot motion. Astion DJ, Deland JT, Otis JC, et al: Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am 1997;79:241-246.
Question 62
A 46-year-old woman has bilateral groin pain, with more severe pain on the left side than on the right side. Figures 44a and 44b show a radiograph and a T1-weighted MRI scan. What is the most likely diagnosis?


Explanation
The radiograph reveals bilateral patchy sclerosis of the femoral heads without evidence of collapse. The MRI scan shows bilateral head involvement with a common serpentine-like low-intensity signal of the superior femoral head that is common to osteonecrosis. Changes confined to the femoral head effectively exclude rheumatoid arthritis and osteoarthritis. Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3160-3162.
Question 63
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of


Explanation
The underlying diagnosis is multiple myeloma. Because the patient has a large lucent lesion in the peritrochanteric region of the left proximal femur, the risk of pathologic fracture is high. Consideration should be given to prophylactic internal fixation with a locked intramedullary rod. The lesion does not appear to be a sarcoma requiring wide resection and endoprosthetic reconstruction. Neither chemotherapy nor radiation therapy alone is likely to result in long-term stabilization of the proximal femur. Postoperative treatment with bisphosphonates and radiation therapy is indicated to decrease the risk of future pathologic fractures. The patient should also be referred to a medical oncologist for medical management. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Question 64
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of

Explanation
The CT scan shows a stress fracture of the olecranon. This injury is the result of repetitive abutment of the olecranon into the olecranon fossa, traction from triceps activity during the deceleration phase of the throwing motion, and impaction of the medial olecranon onto the olecranon fossa from valgus forces. Fractures may be either transverse or oblique in orientation. Initial treatment consists of rest and temporary splinting. Electrical bone stimulation may also be considered. Open fixation with a large compression screw is recommended when nonsurgical management has failed to provide relief. Ahmad CS, ElAttrache NS: Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med 2004;23:665-676.
Question 65
After excising a mass from the thigh that was thought to be a lipoma, the pathology reveals that the mass is a high-grade sarcoma. Subsequent treatment should include

Explanation
Following excision of a suspected benign soft-tissue tumor that proves to be malignant, repeat excision of the tumor bed is recommended. The initial surgical margins are inadequate after an intralesional or marginal excision, necessitating additional surgery for more definitive local control. While radiation therapy and/or chemotherapy may help to reduce the risk of local recurrence in patients with microscopic residual disease, local control is improved following repeat excision. Radiation therapy alone is inadequate to address poor surgical margins, and would likely be given postoperatively. Bisphosphonates have no current role in the treatment of soft-tissue sarcoma. Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 66
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?




Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 67
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on

Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 68
Which of the following is considered the treatment of choice for a 3-cm chondroblastoma of the distal femoral epiphysis with no intra-articular extension?
Explanation
Curettage and bone grafting typically are the preferred treatment of chondroblastoma, yielding acceptable local recurrence rates of less than 10%. Some surgeons advocate adjuvant therapies such as phenol, liquid nitrogen, or argon beam coagulation. Untreated, these lesions can destroy bone and invade the joint to a significant degree. Large intra-articular lesions may require major joint reconstruction. Wide local excision is rarely required to control the tumor. Radiation therapy is indicated only in unresectable lesions. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748.
Question 69
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?

Explanation
The indications for high tibial valgus osteotomy include a physiologically young age, arthritis confined to the medial compartment, 10 to 15 degrees of varus alignment on weight-bearing radiographs, a preoperative arc of motion of at least 90 degrees, flexion contracture of less than 15 degrees, and a motivated, compliant patient. Contraindications include lateral compartment narrowing of the articular cartilage, lateral tibial subluxation of greater than 1 cm, medial compartment bone loss, ligamentous instability, and inflammatory arthritis. Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Question 70
Figures 25a and 25b show the radiograph and MRI scan of a 48-year-old man who reports increasing unsteadiness in his gait and hand clumsiness. Examination reveals a positive Hoffmann's reflex bilaterally, positive clonus, and a spastic gait. Management should consist of


Explanation
The patient has a congenitally small spinal canal with secondary multilevel degenerative changes causing stenosis and cord compression across multiple segments, including directly posterior to the vertebral bodies. A multilevel diskectomy may address the cord compression at the disk level, but not posterior to the bodies, and most likely would be inadequate. The patient has significant stenosis distal to C5, necessitating a more extensive surgical approach than simply C3-C5. Because the patient's cervical lordosis is preserved, a posterior procedure such as laminoplasty or laminectomy would allow the cord to fall away from the anterior pathology and afford decompression. Cervical myelopathy does not tend to resolve, and there is a significant risk for progression; therefore, surgical management usually is recommended. Edwards CC II, Riew KD, Anderson PA, et al: Cervical myelopathy: Current diagnostic and treatment strategies. Spine J 2003;3:68-81.
Question 71
The patient shown in Figure 44 reports that her toes hurt when she walks. Management should consist of

Explanation
Brachymetatarsia is a congenital hypoplasia of one or more metatarsals. Shortening of the fourth metatarsal is the most common form of brachymetatarsia and is often bilateral. Taping and manipulative reduction attempts are ineffective, and extensor tenotomy and capsulotomy are not likely to sufficiently correct the deformity. Fusion or metatarsal lengthening result in complications and generally are not indicated. Shoe modifications, such as extra-depth or extra-wide shoes, generally will improve symptoms. If pressure and trauma persist in the older child, metatarsal lengthening or amputation may be indicated. Stevens PM: Toe deformities, in Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, p 195.
Question 72
Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of

Explanation
Bisphosphonates are indicated in the treatment of osteoporosis. They have been shown to reduce the incidence of vertebral and extremity fractures in patients with a T-score of less than -1.
Question 73
High Yield
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

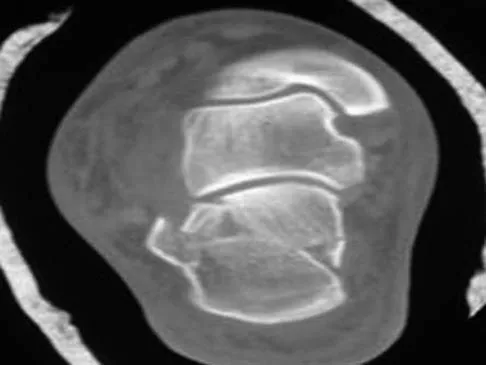
Explanation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744. Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 74
A 38-year-old man underwent a transtibial amputation for chronic posttraumatic foot and ankle pain and chronic calcaneal osteomyelitis. Postoperative radiographs are seen in Figures 41a and 41b. What is the proposed purpose of the surgical modification seen in the radiographs?


Explanation
The Ertl modification of a below-knee amputation has been proposed to create a more stable "platform" to aid in transferring the load of weight bearing between the residual limb and the prosthetic socket. It is felt that a stable platform allows total contact loading over an enlarged stable surface area. Early studies have suggested that this modification may enhance the patient's perceived functional outcome. Pinzur MS, Pinto MA, Saltzman M, et al: Health-related quality of life in patients with transtibial amputation and reconstruction with bone bridging of the distal tibia and fibula. Foot Ankle Int 2006;27:907-912.
Question 75
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management?

Explanation
The patient has necrotizing fasciitis, a rare and sometimes fatal disease that has many different etiologies. Signs that this is not a normal infection are the worsening clinical symptoms despite IV antibiotics and the systemic symptoms. He needs urgent surgical care before he becomes completely septic and unstable. He needs very aggressive debridement of his tissues. Hyperbaric oxygen and immunoglobulins are only anecdotally helpful, and would only be used after surgery. Fontes RA, Ogilvie CM, Miclau T: Necrotizing soft-tissue infections. J Am Acad Orthop Surg 2000;8:151-158.
Question 76
A 10-year-old boy with spastic diplegic cerebral palsy walks in a crouched position with the hips and knees flexed. Maximum knee flexion is 15 degrees during early swing phase. Instrumented gait analysis shows quadriceps activity from terminal stance throughout swing phase. Treatment should consist of
Explanation
The rectus femoris muscle spans two joints and is active during running, sprinting, and walking at a fast pace during the preswing and early swing phase of gait. In these situations, the muscle helps to generate power to initiate hip flexion while absorbing or controlling the rate of knee flexion during early swing phase. Quadriceps activity, including the rectus femoris, is not normally needed when walking at a routine cadence. However, rectus femoris activity is commonly noted during preswing and the swing phase in patients with cerebral palsy, particularly those with diplegia. In an effort to initiate swing phase, the rectus femoris is "overactive." As a result, the knee flexion that commonly occurs at terminal stance and initial swing is restricted. Instead of achieving the normal 50 to 60 degrees of flexion during early swing, this patient's knee flexion is limited to 15 degrees. The goal of treatment is to retain rectus femoris activity for initiation of hip flexion but to diminish its restraint on knee flexion. Studies have shown that transfer of the distal rectus femoris tendon provides more flexion of the knee during the swing phase of gait than simply releasing the tendon. V-Y lengthening of the quadriceps tendon or a Z lengthening of the patellar tendon causes too much weakening of the quadriceps muscle and worsens the crouch deformity. In addition to transfer of the rectus femoris tendon, other procedures are often done concomitantly to obtain the best balance and realignment of hip-knee-ankle activity. Aiona MD: Guidelines for managing lower extremity problems in cerebral palsy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1534-1541. Chambers H, Laure A, Kaufman K, Cardelia M, Sutherland D: Prediction of outcome after rectus femoris surgery in cerebral palsy: The role of cocontraction of the rectus femoris and vastus lateralis. J Pediatr Orthop 1998;18:703-711.
Question 77
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
In review of 154 patients with nonrhabdomyosarcoma, Rao reported that histologic grade, tumor invasiveness, and adequate surgical margin were the most important prognostic factors. Histologic subtype, use of adjuvant chemotherapy, and patient age were not as important. Size related to degree of invasiveness was not statistically significant. Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531. Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 78
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of



Explanation
Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture. Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Question 79
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?



Explanation
Dickman and associates classified injuries of the transverse atlantal ligament into two categories. Type I injuries are disruptions through the substance of the ligament itself. Type II injuries render the transverse ligament physiologically incompetent through fractures and avulsions involving the tubercle of insertion of the transverse ligament on the C1 lateral mass. Type I injuries are incapable of healing without supplemental internal fixation. Type II injuries can be treated with a rigid cervical orthosis with a success rate of 74%. Surgery may be required for type II injures that fail to heal with 3 to 4 months of nonsurgical management. Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.
Question 80
The carpal tunnel canal is narrowest (smallest cross-sectional area) at what level?
Explanation
The carpal tunnel canal has an hourglass shape in the coronal plane and is narrowest at the level of the hook of the hamate. Cobb TK, Dalley BK, Posteraro RH, et al: Anatomy of the flexor retinaculum. J Hand Surg Am 1993;18:91-99.
Question 81
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with


Explanation
An isolated avulsion of the lesser tuberosity occurs very rarely and usually is found in 12- and 13-year-old adolescents. The MRI scans reveal a tear of the humeral attachment of the inferior glenohumeral ligament, a so-called HAGL lesion. This injury to the inferior glenohumeral ligament occurs much less commonly than the classic Bankart lesion (anterior inferior labral tear). A tear of the subscapularis occurs with a similar mechanism of injury but generally occurs in older individuals. Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96.
Question 82
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?




Explanation
Synovial chondromatosis results from chondroid metaplasia within the synovium. Male to female ratio is 2:1, with a peak incidence in early adult life. Radiographs can show speckled cal
Question 83
Etanercept is a recombinant genetically engineered fusion protein used to treat rheumatoid arthritis. What is its mode of action?
Explanation
Etanercept is a molecule consisting of the Fc portion of IgG fused to the extracellular domain of the p76 human THF-a receptor. It is soluble and binds TNF-a. Infliximab is the monoclonal antibody that binds TNF-a. IL-1 receptor antagonists are still in development. Leflunomide is a drug that inhibits pyrimidine synthesis and is similar to methotrexate as an antimetabolite.
Question 84
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?

Explanation
While it is possible to damage any of these structures, unrecognized intraoperative laceration without adequate coagulation of the superior lateral geniculate artery is common. This can result in significant postoperative hemarthrosis and a return to surgery when bleeding cannot be controlled. Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Question 85
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results?



Explanation
The radiographs and CT scan reveal osteoarthritis with posterior subluxation and posterior bone loss. Total shoulder arthroplasty with reaming of the high side to neutralize the glenoid surface has been shown to yield better results than hemiarthroplasty. The amount of bone loss in this patient does not require posterior glenoid augmentation. Reverse total shoulder arthroplasty is indicated for rotator cuff tear arthropathy; therefore, it is not applicable. Arthroscopic debridement has yielded poor results with advanced osteoarthritis and posterior subluxation. Results from glenoid osteotomy have been variable and glenoid osteotomy is not indicated with associated osteoarthritis. Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Question 86
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?


Explanation
PVNS is a rare inflammatory granulomatous condition of unknown etiology, and causes proliferation of the synovium of joints, tendon sheaths, or bursa. The disorder occurs most commonly in the third and fourth decades but can occur at any age. MRI provides excellent delineation of the synovial disease. Characteristic features of PVNS on MRI include the presence of intra-articular nodular masses of low signal intensity on T1- and T2-weighted images and proton density-weighted images. Synovial biopsy should be performed if there is any doubt of the diagnosis. Total synovectomy (open or arthroscopic) is required for the diffuse form, although recurrence is common. Rheumatoid arthritis and synovial chondromatosis are not typically associated with hemorrhagic effusions. De Ponti A, Sansone V, Malchere M: Result of arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602-607. Chin KR, Barr SJ, Winalski C, et al: Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am 2002;84:2192-2202.
Question 87
Fixed hyperextension of the metatarsophalangeal joint is associated with
Explanation
Claw toe and hammer toe deformities are associated with dorsal subluxation of the interossei, which can no longer serve to flex the metatarsophalangeal joint. The extensor digitorum longus then loses its tenodesing effect on the proximal interphalangeal and distal interphalangeal joints and works unopposed to extend the metatarsophalangeal joint and the proximal phalanx. Without the antagonistic action of the extensor digitorum longus, the extrinsic flexors become unopposed flexors of the proximal and distal interphalangeal joints. Marks RM: Anatomy and pathophysiology of lesser toe deformities. Foot Ankle Clin 1998;3:199-213.
Question 88
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?


Explanation
Crossover second toes are attributed to attenuation or rupture of the plantar plate and lateral collateral ligament and are associated with varying degrees of instability. Flexor-to-extensor transfer (Girdlestone/Taylor procedure) can provide intrinsic stability to the toe. Although plantar metatarsal head condylectomy can increase stability by resulting in scarring of the plantar plate, excision of the entire second metatarsal head carries a high risk of transfer metatarsalgia. Removal of the base of the proximal phalanx destabilizes the toe and should be reserved as a salvage procedure. Simple flexor tenotomy alone will not improve stability, and arthrodesis of the second metatarsophalangeal joint will limit motion and impair function. Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Question 89
What is the most likely cause of the lesion shown in Figures 35a and 35b?


Explanation
The most common cause of myositis ossificans is contusion. Certain regions, including the quadriceps and brachialis, are more commonly affected. The mechanisms of development have not been clearly established. Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Question 90
According to the Third National Acute Spinal Cord Injury Study (NASCIS 3), what is the recommended protocol for a patient who sustained a spinal cord injury 7 hours ago?
Explanation
NASCIS 2 established the recommended doses of methylprednisolone for spinal cord injury. This included an initial bolus of 30 mg/kg over 1 hour, followed by an infusion of 5.4 mg/kg/h for an additional 23 hours. If the injury was more than 8 hours old, the methylprednisolone was not recommended. NASCIS 3 changed the dosing schedule based on the time from injury. If the time from injury to treatment was less than 3 hours, the standard protocol was followed (30 mg/kg bolus followed by 5.4 mg/kg/h for 23 hours). If the time from injury to treatment was between 3 and 8 hours, the infusion was continued at 5.4 mg/kg for an additional 23 hours (48 hours total). In this situation with a time of injury 7 hours ago, treatment should consist of a bolus and further steroid therapy for 48 hours. Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 91
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70 degrees of the right knee. The active arc of motion is from 70 degrees to 90 degrees, and the opposite knee has a flexion contracture of 10 degrees. Both hips are dislocated with flexion contractures of 10 degrees, passive hip motion is from 10 degrees to 90 degrees of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
Most children with amyoplasia are ambulatory and when a decrease in function occurs because of a severe contracture, it must be addressed. A radical posterior soft-tissue release, including the posterior knee capsule and often the collateral ligaments and the posterior cruciate ligament, is needed to obtain extension. After the age of 1 year, aggressive physical therapy will do little to correct a contracture. Botulinum toxin A is indicated for spasticity and is contraindicated with severe contractures. Supracondylar femoral extension osteotomy works well, but will remodel at an average rate of 1 degree per month, which is not considered ideal in a young patient. Gradual correction with a circular ring external fixator is an option, but a soft-tissue release will also most likely be needed for a contracture of this severity. Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469. DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Question 92
Figure 26a shows the radiograph of a 55-year-old woman who has pain in her right leg after falling. Laboratory studies reveal an elevated alkaline phosphatase level. A biopsy specimen from the proximal tibia is shown in Figure 26b. What is the most likely diagnosis?


Explanation
Paget's disease of bone is a metabolic disorder of bone remodeling. The normally coupled process of bone resorption and deposition is lost, resulting in excessive localized bone resorption and compensatory increased bone formation. Pagetic bone tends to be more brittle; therefore, it is susceptible to pathologic fractures and subsequent deformities. Lander PH, Hadjipavlou AG: A dynamic classification of Paget's disease. J Bone Joint Surg Br 1986;68:431-438.
Question 93
A 58-year-old woman with rheumatoid arthritis has progressive neck pain, upper extremity and lower extremity weakness, and difficulty with fine motor movements. Examination reveals hyperreflexia with mild to moderate objective weakness but the patient has no difficulty with ambulation for short distances. What is the most important preoperative imaging finding that predicts full neurologic recovery with surgical stabilization?
Explanation
Boden and associates' article presents compelling evidence that patients with rheumatoid arthritis and neurologic deterioration in C1-2 instability are more likely to achieve some improvement if the posterior atlanto-dens interval is greater than 10 mm on preoperative studies. All the patients in their series who had neurologic deterioration and a preoperative posterior atlanto-dens interval of greater than 14 mm achieved complete motor recovery. Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297. Boden SD, Clark CR: Rheumatoid arthritis of the cervical spine, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Scientific References
-
:
Question 94
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?

Explanation
While injury of the distal radial metaphysis is a rather common occurrence, the incidence of physeal arrest is only about 4% to 5% of patients. While injury of the distal physis of the ulna is rare, the incidence of physeal arrest is greater than 50% in fractures of this structure. These patients need to be followed closely both clinically and radiographically to look for the signs of distal ulnar/physeal arrest such as loss of the prominence of the ulna and ulnar deviation of the hand. Radiographically, progressive shortening of the ulna is observed. Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Question 95
What is the most commonly reported complication following elbow arthroscopy?

Explanation
The complication rate following elbow arthroscopy is reported at 5%. The most commonly reported complication is transient neurapraxia, with nerve transection remaining an unfortunate and rare event. While infection remains the most common serious complication, it is uncommon (0.8%). Synovial cutaneous fistula and compartment syndrome, while reported, are the least frequent complications of elbow arthroscopy. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 96
Figure 12 shows the radiograph of a 15-year-old boy with cerebral palsy who has pain at the first metatarsophalangeal joints. He is a community ambulator. Management consisting of accommodative shoes has failed to provide relief. What is the treatment of choice?

Explanation
While other surgeries have provided some success, first metatarsophalangeal joint arthrodesis has the highest overall success rate compared to other surgeries in ambulatory and nonambulatory children with cerebral palsy. The recurrence rate is unacceptably high with the other procedures listed above. In contrast, neurologically normal children are amenable to osteotomies and soft-tissue procedures. Davids JR, Mason TA, Danko A, et al: Surgical management of hallux valgus deformity in children with cerebral palsy. J Pediatr Orthop 2001;21:89-94.
Question 97
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?



Explanation
The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 98
Figure 2a shows the radiograph of a 48-year-old man who was involved in a motorcycle accident. A CT scan is shown in Figure 2b. The patient underwent pelvic angiography for persistent hypotension despite resuscitation. What vessel is most likely to be injured?


Explanation
The pelvic injury is a severe anterior-posterior compression III or Tile C injury. The vessel most likely injured is the superior gluteal artery, but several arterial bleeding sources are likely. Vertical shear injuries can also injure this vessel, but it is much less common. When arterial injury follows a lateral compression injury, it is usually related to injury of a more anterior vessel like the obturator artery or a branch of the external iliac artery. O'Neill PA, Riina J, Sclafani S, et al: Angiographic findings in pelvic fractures. Clin Orthop 1996;329:60-67.
Question 99
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should

Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 100
A 10-year-old child with cerebral palsy undergoes bilateral hamstring lengthening for severe knee flexion contractures, and knee immobilizers are applied postoperatively. Examination at the initial postoperative check 2 hours after surgery reveals that she can dorsiflex her toes on the right foot, but not on the left foot. The physician should now
Explanation
Children with cerebral palsy are often difficult to examine. However, this patient clearly has a peroneal nerve deficit, most likely from the acute stretch after the hamstring lengthening. The nerve has the best chance of recovery if it is relaxed by flexing the knee. Once the nerve has recovered, gradual knee extension can be accomplished. Aspden RM, Porter RW: Nerve traction during correction of knee flexion deformity: A case report and calculation. J Bone Joint Surg Br 1994;76:471-473.
