Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
Explanation
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted. Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Question 2
A 45-year-old woman has had progressive right shoulder pain for the past 6 months. She notes that the pain disrupts her sleep, she has pain at rest that requires the use of narcotic analgesics, and she has limited use of her left shoulder for most activities of daily living. History reveals the use of corticosteroids for systemic lupus erythematosus. Examination shows diminished range of motion. Radiographs of the right shoulder are shown in Figures 4a and 4b. Treatment should consist of


Explanation
Humeral arthroplasty provides excellent pain relief and function for stage IV osteonecrosis with humeral collapse. In late disease with glenoid involvement (stage V), total shoulder arthroplasty is preferred. Some authors have reported satisfactory results with core decompression of the humeral head for early stages of osteonecrosis, but results for stage IV osteonecrosis are less satisfactory when compared with those for humeral arthroplasty. Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. LePorte DM, Mont MA, Mohan V, Pierre-Jacques H, Jones LC, Hungerford DS: Osteonecrosis of the humeral head treated by core decompression. Clin Orthop 1998;355:254-260.
Question 3
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
Atraumatic subluxation or dislocation of the sternoclavicular joint typically occurs in individuals with generalized ligamentous laxity. It is generally not painful, has no long-term sequelae, and needs no treatment. In fact, it is more likely to be painful following surgery than if managed nonsurgically. Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 4
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 5
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
Peak embolization is observed during femoral stem insertion. Embolization is also observed during acetabular preparation and hip reduction. Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Question 6
A 63-year-woman has an elbow flexion contracture. History reveals that she underwent three previous surgeries to remove a malignant fibrous histiocytoma of the forearm. An MRI scan reveals a locally recurrent tumor at the site of the previous surgery. Which of the following is considered the most predictive factor for local recurrence?

Explanation
The greatest risk factor for local recurrence is an inadequate surgical margin. The tumor grade, histologic subtype, and size are predictive of systemic relapse. Sarcomas that arise in some anatomic sites, such as the forearm or retroperitoneum, may be more difficult to completely resect compared with other sites. The optimum margin is generally considered to be a cuff of normal tissue beyond the tumor. Bell RS, O'Sullivan B, Liu FF, et al: The surgical margin in soft-tissue sarcoma. J Bone Joint Surg Am 1989;71:370-375. Sadoski C, Suit HD, Rosenberg A, Mankin H, Efird J: Preoperative radiation, surgical margins, and local control of extremity sarcomas of soft tissues. J Surg Oncol 1993;52:223-230.
Question 7
A 25-year-old man underwent a Putti-Platt repair for recurrent anterior dislocation of his right shoulder 9 months ago. He reports no further episodes of instability but continues to have severely restricted motion, with external rotation limited to less than 0 degrees with the arm at the side. He has pain at the ends of range of motion and restricted activities of daily living despite undergoing nearly 9 months of physical therapy. Radiographs of the shoulder show no arthritic changes. Management should now consist of
Explanation
Open release allows lengthening of the shortened subscapularis and is preferred when there are extra-articular contractures. Arthroscopic release, combined with the use of an interscalene catheter postoperatively, is an excellent treatment for capsular contractures but is contraindicated after procedures that result in extracapsular shortening (ie, Magnuson-Stack, Putti-Platt). Additional physical therapy or manipulation under anesthesia is not likely to be helpful. Shoulder hemiarthroplasty is contraindicated with normal articular surfaces, but prosthetic arthroplasty is sometimes necessary for arthritis associated with instability or overly tight instability repairs. Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147. Warner JJ: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg 1997;5:130-140. Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Question 8
A patient with rheumatoid arthritis with both ankle and subtalar involvement was treated as shown in Figures 11a and 11b. What complication is unique to this type of fixation?


Explanation
The interlocking screws at the proximal end of the rod can act as a stress riser and lead to fracture. Postoperative pain at this level should prompt inclusion of this diagnosis in the differential. Removing the screws following bone union can decrease the chances of this occurring. A short rod that avoids the diaphyseal area may also be beneficial. Rotatory deformity is controlled by the perpendicularly oriented distal transfixion screws. Talar osteonecrosis would be unusual since the dissection can be minimized with an intramedullary rod. Any type of hardware can fail if the construct does not lead to a solid arthrodesis. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 236-237. Thordarson DB, Chang D: Stress fractures and tibial cortical hypertrophy after tibiotalocalcaneal arthrodesis with an intramedullary nail. Foot Ankle Int 1999;20:497-500.
Question 9
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the

Explanation
Capsular exposure for an inside-out lateral meniscal repair is performed by developing the interval between the iliotibial band and biceps tendon. Posterior retraction of the biceps tendon exposes the lateral head of the gastrocnemius. Posterior retraction of the gastrocnemius provides access to the posterolateral capsule. Miller DB Jr: Arthroscopic meniscus repair. Am J Sports Med 1988;16:315-320.
Question 10
In the initial evaluation of acute low back pain (duration of less than 4 weeks), plain radiographs are recommended in which of the following situations?

Explanation
Prolonged use of steroids is associated with compression fractures with minimal trauma. Indications for radiography with acute low back pain include possible tumor, fracture, infection, or cauda equina syndrome. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Question 11
Figures 21a and 21b show the radiographs of a 22-year-old man who was shot through the abdomen the previous evening. An exploratory laparotomy performed at the time of admission revealed a colon injury. Current examination reveals no neurologic deficits. Management for the spinal injury should include


Explanation
IV broad-spectrum antibiotics should be administered for 7 days. This regimen, when compared to fragment removal or other antibiotic regimens, has been shown to reduce the incidence of spinal infections and reduce the need for metallic fragment removal with perforation of a viscus. Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Question 12
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of

Explanation
The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
Question 13
A 25-year-old woman undergoes surgical treatment of a displaced proximal humeral fracture via a deltopectoral approach. At the first postoperative visit, she reports a tingling numbness along the anterolateral aspect of the forearm. What structure is most likely injured?
Explanation
Sensation along the anterolateral aspect of the forearm is supplied by the lateral antebrachial cutaneous nerve, the terminal branch of the musculocutaneous nerve. The musculocutaneous nerve can be injured by proximal humeral fractures or dislocations, and is also at risk during surgical exposure if excessive retraction is placed on the conjoint tendon. The musculocutaneous nerve enters the conjoint tendon 1 cm to 5 cm distal to the coracoid process. McIlveen SJ, Duralde XA, D'Alessandro DF, et al: Isolated nerve injuries about the shoulder. Clin Orthop 1994;306:54-63.
Question 14
A 10-year-old girl reports activity-related bilateral arm pain. Examination reveals no soft-tissue masses in either arm, and she has full painless range of motion in both shoulders and elbows. The radiograph and bone scan are shown in Figures 20a and 20b, and biopsy specimens are shown in Figures 20c and 20d. What is the most likely diagnosis?




Explanation
Based on these findings, the most likely diagnosis is fibrous dysplasia. Twenty percent of patients with fibrous dysplasia have multifocal disease. The lesions show a typical ground glass appearance. Fibrous dysplasia frequently involves the diaphysis of the long bones. There is no associated soft-tissue mass and no periosteal reactions to these lesions, suggesting a benign lesion. The histology shows proliferating fibroblasts in a dense collagen matrix. Trabeculae are arranged in an irregular or "Chinese letter" appearance. Osteogenic sarcoma and Ewing's sarcoma have a much different radiographic appearance of malignant osteoid and small round blue cells. Periosteal chondroma does occur in the proximal humerus but is not typically multifocal. It appears as a surface lesion with saucerization of the underlying bone and a bony buttress adjacent to the lesion. Some patients with multifocal lesions have associated endocrine abnormalities (McCune-Albright syndrome). Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 118-119.
Question 15
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
The maximum stress in a bone occurs at the periosteal surface (the greatest distance from the center of the bone). The magnitude of the stress is equal to the magnitude of the applied moment (M) multiplied by the distance to the surface (roughly the radius of the bone, r) divided by the area moment of inertia (I), so that stress = Mr/I. Of the possible answers, only area moment of inertia of the cross section contains any of these three items. The stress can also depend on the length of the bone, but it cannot be determined without knowing the location at which the bending load is applied, information that was not given in the problem. The type of structural support may influence local stresses where the support contacts the bone, but it has little effect on the maximum stress in the bone. The cross-sectional area is not as important as the area moment of inertia because the stress is not evenly distributed over the cross-section. Plastic modulus is a material property, not a geometric or structural property, and it does not affect stress. Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Question 16
Which of the following benign bone lesions can develop lung metastases?
Explanation
Although considered benign bone lesions, lung metastases can develop in giant cell tumors and chondroblastomas. These often can be treated with multiple thoracotomies, resulting in long-term survival. Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
Question 17
What is the relative amount of type II collagen synthesis in disease-free adult articular cartilage compared to developing teenagers?
Explanation
Adult articular cartilage has less than 5% of the synthesis rate of type II collagen than that seen in developing teenagers. Both synthesis and degradation of type II collagen in normal adult articular cartilage is very low compared to children. In osteoarthrosis, both synthesis and degradation are increased, but the collagen does not properly incorporate into the matrix. Lippiello L, Hall D, Mankin HJ: Collagen synthesis in normal and osteoarthritic human cartilage. J Clin Invest 1977;59:593-600.
Question 18
In the most common condition causing a winged scapula, which of the following nerves is affected?

Explanation
A winged scapula is most often associated with Parsonage-Turner syndrome, a condition thought to be due to an inflammatory or immune-mediated mechanism. Certain muscles are predisposed, particularly the serratus anterior muscle innervated by the long thoracic nerve. Other less common nerve lesions (eg, the spinal accessory and dorsal scapular nerves) may also cause winged scapulae. Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995.
Question 19
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of

Explanation
Children with spina bifida and bilateral symmetrical dislocation of the hips usually do not require treatment. A level pelvis and good range of motion of the hips are more important for ambulation than reduction of bilateral hip dislocations. Because the patient has good sitting and standing balance and good range of motion, maintenance of that range of motion and symmetry is more important than reduction. Surgery is not recommended.
Question 20
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of

Explanation
Although this is a fracture of the medial and lateral malleoli, the degree of displacement and comminution of the medial dome indicate that this injury is similar to a pilon fracture. Initial management should consistent of stabilization to allow for soft-tissue healing. The use of temporizing spanning external fixation should be the initial step, followed by limited or more extensive open reduction and internal fixation when the soft-tissue status will allow. Initial placement in either a short or long leg cast does not provide the needed stability and does not allow for care and monitoring of soft tissues. In addition, maintaining reduction of the talus may be very difficult. Immediate open reduction and internal fixation through an injured soft-tissue envelope adds the risk of difficulties with incision healing and a higher risk of deep infection. In the acute setting, a primary ankle fusion through this soft-tissue envelope is not indicated. Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509. Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 21
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?


Explanation
Glenoid dysplasia is an uncommon anomaly that usually has a benign course but may result in shoulder pain, arthritis, or multidirectional instability. Shoulder pain and instability often improve with shoulder strengthening exercises. Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Question 22
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?



Explanation
The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Question 23
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?

Explanation
It is critical to withhold active range of motion of the shoulder within the first 6 weeks after arthroplasty for acute fracture to prevent tuberosity avulsion. When radiographic and clinical findings show that the tuberosities are healed, active motion may be instituted, usually at 6 to 8 weeks. Immediate passive range-of-motion exercises, including external rotation with a stick, pendulum, and passive elevation, should begin within the limits of the repair on the day of surgery to prevent stiffness. Hartstock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humerus fractures. Orthop Clin North Am 1998;29:467-475.
Question 24
An active 36-year-old woman with rheumatoid arthritis has continued forefoot discomfort despite the use of orthotics and shoe wear modifications. A radiograph and a clinical photograph are shown in Figures 26a and 26b. Treatment at this point should consist of


Explanation
In a patient with inflammatory arthritis, advanced hallux valgus deformity in conjunction with lesser metatarsophalangeal joint destruction and subluxation warrants fusion of the first metatarsophalangeal joint and lesser metatarsal head resections. Hallux valgus correction will fail because of incompetent soft tissues. A Keller resection arthroplasty is not indicated in this age group. Synovectomy is contraindicated because of evidence of erosive changes of the lesser metatarsophalangeal joints. Ouzounian T: Rheumatoid arthritis of the foot & ankle, in Myerson MS (ed): Foot & Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 2, pp 1189-1204. Mann RA, Thompson FM: Arthrodesis of the first metatarsophalangeal joint for hallux valgus in rheumatoid arthritis. J Bone Joint Surg Am 1984;66:687-692.
Question 25
A study is designed that examines fractures in children with osteogenesis imperfecta after being treated with bisphosphonates compared with a placebo. A difference is found for which the P value is greater than what is considered to be statistically significant. What is the next appropriate statistical analysis?
Explanation
When a study yields a negative result between treatment groups, the next step is to perform a power analysis. The power, by definition, is the probability of rejecting the null hypothesis: in this example the null hypothesis would be that children treated with bisphosphonates would have fewer fractures than the untreated control population. The power analysis helps answer the question as to whether the null hypothesis should be rejected and the finding is real, or whether the sample size was too small or the effect of treatment too subtle to demonstrate a difference between the treatment and control groups. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 7.
Question 26
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Explanation
The superior gluteal artery is most at risk with a posterior iliac crest bone graft harvest. The artery leaves the pelvis through the sciatic notch and can be injured by retractors or other sharp instruments entering the sciatic notch area. The deep circumflex iliac, iliolumbar, and fourth lumbar arteries supply the iliacus and iliopsoas muscles and can be damaged during anterior bone graft harvest. The ascending branch of the lateral femoral circumflex artery is at risk during the anterior approach to the hip. Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Question 27
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
The most common side effect of an interscalene block is ipsilateral phrenic nerve blockade. The phrenic nerve arises chiefly from the fourth cervical ramus (with contributions from the third and fifth) and is the sole motor supply to the diaphragm. Phrenic nerve palsy usually is well tolerated in healthy patients but should be avoided in patients with limited pulmonary function (severe restrictive or obstructive lung disease, myasthenia gravis, or contralateral hemidiaphragmatic dysfunction). The incidence of ipsilateral phrenic nerve blockade afer interscalene block approaches 100%. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Question 28
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?

Explanation
The flexor hallucis longus tendon provides the best, most direct route of transfer for filling Achilles tendon gaps. The tendon lies lateral to the neurovascular structures, making it safe for harvest and providing a direct route for transfer into the calcaneus without crossing these important structures. The flexor hallucis longus tendon also has muscle belly that extends distal on the tendon itself, often beyond the actual tibiotalar joint. When the tendon is transferred, this muscle belly brings excellent blood supply to the anterior portion of the reconstruction. Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Question 29
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
A muscle that lengthens as it is activated is an eccentric contraction. Isometric contraction involves no change in length. Concentric contraction occurs while the muscle is shortening. In isotonic contraction, the force remains constant through the contraction range. Isokinetic muscle contraction occurs at a constant rate of angular change of the involved joint. Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 12-13.
Question 30
Figure 37 shows a coronal T2-weighted MRI scan. What is the name of the labeled torn structure?

Explanation
The labeled structure is the LCL, and it is avulsed from the lateral humeral epicondyle. This is the most common site of injury for the LCL. The biceps and brachialis tendon insertions are not well visualized in this section. The MCL and flexor/pronator origin are intact. Potter HG, Weiland AJ, Schatz JA, et al: Posterolateral rotatory instability of the elbow: Usefulness of MR imaging in diagnosis. Radiology 1997;204:185-189.
Question 31
When evaluating articular cartilage, what extracellular matrix component is most closely associated with the deep calcified cartilage zone?
Explanation
Collagen type X is produced only by hypertrophic chondrocytes during enchondral ossification (growth plate, fracture callus, heterotopic ossification) and is associated with calcification of cartilage in the deep zone of articular cartilage. Collagen type I is the predominant collagen in bone, ligament, and tendon. Collagen type II is the predominant collagen in articular cartilage. Proteoglycan aggrecan and hyaluronic acid are components of the extracellular matrix and are involved in the compressive strength characteristics of articular cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Tissue design and chondrocyte matrix interactions. Instr Course Lect 1998;47:477-486.
Question 32
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of


Explanation
The MRI scans show a mesoacromion with tendonopathy of the supraspinatus. The history and physical findings indicate that the patient has a symptomatic os acromiale. Simple excision of the unstable os acromiale has not yielded consistently good results. Meticulous internal fixation using tension banding with cannulated screws and autologous bone grafting has shown good results for this problem. Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Question 33
The palmar cutaneous branch of the median nerve (PCBMN) originates from the
Explanation
The PCBMN originates from the median nerve proper between 3 and 21 cm proximal to the wrist with moderate variation. It virtually always originates from the radial side of the nerve and travels distally with the median nerve, radial to the palmaris longus, and ulnar to the flexor carpi radialis. Hobbs RA, Magnussen PA, Tonkin MA: Palmar cutaneous branch of the median nerve. J Hand Surg Am 1990;15:38-43.
Question 34
A 43-year-old woman has an enlarging mass in the left groin. A radiograph, CT scan, and a biopsy specimen are shown in Figures 42a through 42c. Treatment should consist of



Explanation
The patient has a pelvic chondrosarcoma. The radiograph shows a lytic bone lesion emanating from the left inferior pubic ramus and extending into the soft tissues. Punctate calcifications are revealed on the radiograph and CT scan. The histology is consistent with a malignant cartilage lesion. Appropriate treatment for a pelvic chondrosarcoma is wide resection. In this location, wide resection of the ischiopelvic region (type 3 internal hemipelvectomy) is the treatment of choice. A type 2 internal hemipelvectomy involves resection of the periacetabular region. A type 1 internal hemipelvectomy involves resection of the ilium. No reconstruction is required for a type 3 resection. A classic hemipelvectomy is not necessary because the tumor can be removed with an adequate margin while maintaining the neurovascular structures and hip joint. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 35
A 56-year-old woman has a painful mass on the bottom of her left foot, and orthotic management has failed to provide relief. Examination reveals that the mass is contiguous with the plantar fascia. An MRI scan shows a homogenous nodule within the plantar fascia. Resection of the tumor is shown in the clinical photograph in Figure 39. What type of cell is most likely responsible for the formation of this tumor?

Explanation
The history, examination, and surgical findings are most consistent with plantar fibromatosis. Plantar fibromatosis is a benign tumor of the plantar fascia that consists chiefly of fibromyoblasts. These cells produce excessive collagen and are similar to the cells found in the palmar fascia of patients with Dupuytren's contracture of the hand. The myocyte, synovial cell, and osteocyte all produce their respective individual tissue types but do not contribute to the formation of a plantar fibromatosis. The T-cell is an important immunologic cell that is most affected in patients with HIV.
Question 36
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?

Explanation
In an acute first-time dislocation, arthroscopy has been shown to reveal a Bankart lesion in most shoulders. The classic finding of labral detachment from the anterior inferior glenoid along with occasional hemorrhage within the inferior glenohumeral ligament is the most common sequelae of a traumatic anterior inferior dislocation. Acute treatment, if chosen, is repair of the labral tissue back to the glenoid plus or minus any capsular plication to address potential plastic deformation of the glenohumeral ligament. Acute treatment of a patient sustaining a first-time dislocation remains controversial. The potential indications may be patients whose dislocation occurs at the end of a season and when the desire to minimize risk of future instability outweighs the risks of surgical intervention. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311. DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Question 37
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?

Explanation
In the early 1990s, a transition was made from a two-incision ACL reconstruction to a single-incision ACL reconstruction, and there was concern over divergence of the femoral screws. It was shown radiographically that approximately 5% of the time, divergence of the screw was greater than 15 degrees from the bone plug. In a bovine model, there was significant loss of pull-out strength with an increase in divergence from 15 degrees to 30 degrees. Therefore, attempts should be made to minimize divergence to 15 degrees or less. Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Question 38
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?

Explanation
The patient sustained an injury to the long thoracic nerve, which supplies the serratus anterior. Branches of C5 and C6 enter the scalenus medius, unite in the muscle, and emerge as a single trunk and pass down the axilla. On the surface of the serratus anterior, the long thoracic nerve is joined by the branch from C7 and descends in front of the serratus anterior, providing segmental innervation to the serratus anterior.
Question 39
Figure 17 shows the radiograph of a 2-year-old girl who sustained a fracture of the femur in a fall while walking with her parents. History reveals that this is her third long bone fracture, having sustained a humerus fracture 1 year ago and a fracture of the opposite femur 9 months ago. There is no family history of any similar problem. Examination reveals distinctly blue sclerae, normal appearing teeth, and no skin lesions. What is the most likely cause of this patient's disorder?

Explanation
Osteogenesis imperfecta (OI) is a genetically determined disorder of type I collagen synthesis that is characterized by bone fragility. This patient has had three fractures of the long bones by age 2 years, with the last one occurring after relatively minor trauma. The patient's history and clinical features are consistent with a diagnosis of Sillence type IA OI. Type I OI is the mildest and most common form. Inheritance is autosomal-dominant; however, as in this patient, new mutations are frequent. Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). The sclerae are blue, and the first fractures usually occur in the preschool years after walking has begun. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. Qualitative mutations that lead to an abnormal type I procollagen molecule result in more severe types of the disorder. There are no indications that this child has been abused. Radiographs of the femur show no evidence of rickets, pyknodysostosis, or osteopetrosis. Morquio syndrome, characterized by excess excretion of keratin sulfate in the urine, is not associated with bone fragility. Kocher MS, Shapiro F: Osteogenesis imperfecta. J Am Acad Orthop Surg 1998;6:225-236. Sillence DO, Senn A, Danks DM: Osteogenesis imperfecta: An expanding panorama of variants. Clin Orthop 1981;159:11-25.
Question 40
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?


Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 41
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?

Explanation
Hypertrophic cardiomyopathy (HCM) accounts for up to 50% of cases of sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH ("athlete's heart") from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm). Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete's heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436. Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Question 42
A 40-year-old man underwent an ankle arthroscopy 6 months ago for a talus osteochondral defect. He continues to have pain and burning on the lateral portal but states that the pain is now more superficial than his original pain. Examination reveals that he has shooting pain to his medial foot and ankle when his lateral portal is tapped. A previous injection around the lateral portal gave him relief for about 2 weeks. What treatment will best eliminate his pain?
Explanation
The patient clearly has entrapment of the superficial peroneal nerve in the lateral portal. It is most likely only the medial branch by examination. If the nerve is in good condition, it can simply be released. If the nerve is cut or severely thinned, it is better excised and buried. The sural nerve most likely would be caught in a posterior-lateral portal. Jobe MT, Wright PE: Peripheral nerve injuries, in Canale ST (ed): Campbell's Operative Orthopaedics. St Louis, MO, Mosby, 1998, pp 3839-3844.
Question 43
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
The best method of evaluating the acuity of osteoporotic compression fractures is to look for edema in the vertebral body. This is best accomplished with a STIR-weighted MRI scan. Bone scans can show increased uptake at the site of fracture for many months after the fracture. T1-weighted MRI scans show loss of normal marrow fat that may not necessarily correspond with acuity of the fracture. CT scans and radiographs show fracture deformity but cannot be used to judge acuity. Phillips FM: Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28:S45-S53.
Question 44
High Yield
What vessel is marked with an asterisk in Figure 44?

Explanation
The superior gluteal artery is a branch of the posterior division of the internal iliac artery and exits the pelvis through the greater sciatic notch. It can be injured as a result of a pelvic ring fracture or acetabular fracture that has a fracture of the posterior column. Agur AM, Dalley AF (eds): Grant's Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Question 45
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include

Explanation
The patient may have Beckwith-Wiedemann syndrome (BWS), which consists of exophthalmos, macroglossia, gigantism, visceromegaly, abdominal wall defects, and neonatal hypoglycemia. Hemihypertrophy develops in approximately 15% of patients with BWS. Patients with hemihypertrophy that is the result of BWS have a 40% chance of developing malignancies such as Wilms' tumor or hepatoblastoma; therefore, frequent ultrasound screening is recommended until about age 7 years. The absence of nevi and vascular markings helps to rule out other causes of hemihypertrophy, such as neurofibromatosis, Proteus syndrome, and Klippel-Trenaunay syndrome. Bone age estimations are not accurate at this young age but may become more useful later to help predict the timing of epiphysiodesis procedures. DeBaun MR, Tucker MA: Risk of cancer during the first four years of life in children from The Beckwith-Wiedemann Syndrome Registry. J Pediatr 1998;132:398-400. Ballock RT, Wiesner GL, Myers MT, et al: Hemihypertrophy concepts and controversies. J Bone Joint Surg Am 1997;79:1731-1738.
Question 46
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?

Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate. Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
Question 47
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include


Explanation
The findings are consistent with a neurapraxia of the anterior interosseous branch of the median nerve. This is the most common nerve palsy seen with supracondylar humerus fractures, followed closely by radial nerve palsy. Nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies and surgery are not indicated. Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
Question 48
A 47-year-old woman underwent a distal chevron bunionectomy 2 months ago. Her postoperative recovery had been uneventful until 1 week ago. She now has new onset pain and dorsal swelling in the area of the third metatarsal. A radiograph is shown in Figure 27. What is the most likely diagnosis?

Explanation
Based on findings of a sudden increase in pain with associated swelling, the most likely diagnosis is a stress fracture. The initial radiographic findings usually will be negative. Morton's neuroma and transfer metatarsalgia are not associated with swelling. Metatarsophalangeal synovitis usually involves the second metatarsophalangeal joint. Freiberg's infraction is seen clearly on a radiograph.
Question 49
What additional percentage of energy expenditure above baseline is required for ambulation after an above-the-knee amputation?
Explanation
Patients with an above-the-knee amputation have a 65% increase in energy expenditure. A patient with a transtibial amputation requires 25% more energy above baseline values; however, bilateral transtibial amputations are associated with a 40% increase in energy expenditure. Otis JC, Lane JM, Kroll MA: Energy cost during gait in osteosarcoma patients after resection and knee replacement and after above-the-knee amputation. J Bone Joint Surg Am 1985;67:606-611.
Question 50
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include

Explanation
The patient has a rupture of the long head of the biceps; however, patients older than age 45 years are at greater risk of having an associated rotator cuff tear. An MRI scan should be ordered to avoid missing concomitant rotator cuff pathology. While patients may report pain radiating down the arm at the time of the tendon rupture, an EMG is not indicated. The short head of the biceps is intact and needs no further work-up, even though the muscle descends in most cases. The anterior labrum can be injured but is not associated with this deformity. Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Question 51
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?

Explanation
All of the answers are possible complications of meniscal repair. There are large volumes of literature evaluating the results of meniscal repair, both for the all-inside technique, as well as the inside-out technique. Failure rates are similar. Intra-articular synovitis occurs with absorbable sutures and absorbable implants. Peroneal nerve injuries are more common with the lateral-sided repairs. Saphenous nerve injuries are more common with medial-sided tears. Because of the incision required and the technique of tying over soft tissue, the risk of a saphenous nerve injury is greater with an inside-out technique than with an all-inside technique. Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
Question 52
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
A total hip arthroplasty using the posterior approach has resulted in hip dislocation under certain circumstances. Reconstruction of the external rotator/capsular complex is recognized as a stability-enhancing mechanism for the posterior approach. During the procedure, the acetabular component should be placed in 15 to 20 degrees of anteversion and approximately 45 degrees of abduction. Relative retroversion is a risk factor for posterior dislocation. High abduction angles result in edge loading of the polyethylene and possible early failure, as well as an increased risk of dislocation. Smaller diameter heads and skirted neck extensions used together decrease the range of motion that is allowed before impingement occurs, and this can result in dislocation. Shorter neck lengths generally result in soft-tissue envelope laxity. If laxity occurs, increased offset, neck length, or both can improve stability. Pellicci PM, Bostrom M, Poss R: Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop 1998;355:224-228.
Question 53
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
The most important consequence of a displaced talar neck fracture after closed or open treatment is malunion. Because displacement of the talar neck is associated with displacement of the subtalar joint, any malunion leads to intra-articular incongruity or malalignment of the subtalar joint. Varus malunion is common when there is comminution of the medial talar neck. This results in pain, osteoarthritis, and hindfoot deformity that requires further treatment. Because of these complications, it is imperative that all displaced talar neck fractures are reduced anatomically; fragmented fractures may require bone grafting to maintain the length and rotation of the neck. Tile M: Fractures of the talus, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1996, pp 563-588. Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Question 54
A 60-year-old woman reports anterior knee pain 2 years after undergoing primary total knee arthroplasty for rheumatoid arthritis. A Merchant view of the patella is shown in Figure 16. What is the most likely cause of her pain?

Explanation
Patellar complications commonly occur after primary total knee arthroplasty; therefore, proper component positioning is critical in obtaining a successful result. This patient has lateral tilting and subluxation of the patellar component. Internal rotation of the femoral component has the most deleterious effect on patellar tracking. Lateral placement of the femoral component, medial placement of the patellar component, and external rotation of the tibial component have beneficial effects on patellar tracking. Elevation of the joint line, if not excessive, should not impact patellar tracking. Rand JA: Patellar resurfacing in total knee arthroplasty. Clin Orthop 1990;260:110-117.
Question 55
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a "foot" fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
Stress fractures in female long distance runners are frequently associated with the Female Athletic Triad. The triad consists of osteoporosis, amenorrhea, and altered eating habits. A thorough menstrual history, including age of menarche, history of amenorrhea, and use of oral contraceptives, is imperative. Amenorrhea leads to osteoporosis and predisposes the athlete to fractures. An MRI of the hip is not necessary because a fracture is evident on the radiograph. Serum calcium levels are normal in osteoporosis, a family history would be noncontributory, and it is highly unlikely that a contralateral hip radiograph will yield useful information. Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Question 56
In a longitudinal study of children with spastic diplegia, analysis of long-term function will most likely reveal
Explanation
In a longitudinal study of 18 patients with spastic diplegia over a period of 32 months, three-dimensional gait analysis revealed a deterioration of gait stability with increases in double support time and decreases in single support time. Kinematic data also identified a loss of excursion about the knee, ankle, and pelvis. Interestingly, the static examination of the children showed a decrease in the popliteal angle over time. The authors concluded that ambulatory ability tends to worsen over time in children with spastic diplegia.
Question 57
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Question 58
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of


Explanation
The radiographs show fragmentation of the inferior pole of the patella. This finding, along with the clinical presentation, is most consistent with Sindig-Larsen-Johansson disease. This is an overuse syndrome commonly seen in boys ages 9 to 11 years. The differential diagnosis includes bipartite patella and patellar sleeve fracture. Like most overuse syndromes, Sindig-Larsen-Johansson disease responds to activity modification and nonsteroidal anti-inflammatory drugs. While symptoms usually resolve with short periods of activity restriction, radiographic findings may persist. Stanitski CL: Anterior knee pain syndromes in the adolescent. J Bone Joint Surg Am 1993;75:1407-1416.
Question 59
A 19-year-old football player who sustained three traumatic anterior shoulder dislocations underwent surgery to repair a Bankart lesion. Nine months after surgery, examination reveals stability, elevation to 150 degrees, external rotation to 0 degrees with the elbow at his side and to 50 degrees at 90 degrees of abduction, and internal rotation to T12. If his range of motion does not improve, he is at most risk for
Explanation
Loss of external rotation can lead to degenerative joint disease following an anterior stabilization procedure. A tight anterior capsule will prevent internal impingement. Risk of thoracic outlet syndrome should not be increased. Subscapularis detachment is a risk following open anterior repair; however, a gain in external rotation would be noted. In time, this patient's shoulder may show increased posterior glenohumeral wear but should not have symptoms of recurrent subluxation unless multidirectional instability is present. Hawkins RJ, Angelo RL: Glenohumeral osteoarthrosis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 60
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
Long-term survivorship studies have attempted to clarify patient factors related to good outcomes in HTO. One particular study showed that a patient age of less than 50 years was related to good outcomes in those who had good preoperative knee flexion. The same study found no relation between HTO failure and the presence of postoperative infection or deep venous thrombosis. The presence of a lateral tibial thrust is a contraindication to performing this surgery. As expected, good patient selection is critical to obtaining good long-term results with HTO. Naudie D, Borne RB, Rorabeck CH, Bourne TJ: Survivorship of the high tibial valgus osteotomy: A 10- to 22-year followup study. Clin Orthop 1999;367:18-27. Rinonapoli E, Mancini GB, Corvaglia A, Musiello S: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 61
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?

Explanation
The radiograph shows tuberosity malposition. The effect of improper prosthetic placement has also been associated with poor outcomes. However, the malposition of the tuberosity seen on the radiograph clearly explains loss of motion in this patient. It has been demonstrated that the functional results after hemiarthroplasty for three- and four-part proximal humeral fractures appear to be directly associated with tuberosity osteosynthesis. The most significant factor associated with poor and unsatisfactory postoperative functional results was malposition and/or migration of the tuberosities. Factors associated with a failure of tuberosity osteosynthesis in a recent study were poor initial position of the prosthesis, poor position of the greater tuberosity, and women older than age 75 years (most likely with osteopenic bone). Greater tuberosity displacement has been identified by Tanner and Cofield as being the most common complication after prosthetic arthroplasty for proximal humeral fractures. Furthermore, Bigliani and associates examined the causes of failure after prosthetic replacement for proximal humeral fractures and found that although almost all failed cases had multiple causes, the most common single identifiable reason was greater tuberosity displacement. Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748. Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Question 62
Initial postoperative management after repair of an acute rotator cuff tear includes
Explanation
In the immediate postoperative period following repair of an acute rotator cuff tear, passive forward elevation and external rotation should be performed within the safe zone determined at surgery. Early active range of motion (prior to tendon healing), internal rotation behind the back, and resistive exercises increase the risk of rupture of the repair. Iannotti JP: Full-thickness rotator cuff tear: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Question 63
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
With subscapularis tendon ruptures that have biceps tendon pathology, treatment with tenodesis or tenotomy has improved clinical results. Subluxation or dislocation of the biceps tendon is common with subscapularis rupture. Dislocation of the biceps can occur either beneath the tendon, within the tendon, or extra-articularly. In all cases, the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 64
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?



Explanation
Excessive hindfoot valgus can lead to abutment between the calcaneus and fibula. This valgus force can lead to a stress fracture of the distal fibula. Surgery may be required if an insufficiency fracture recurs despite orthotic management. Of the choices listed, a subtalar arthrodesis is most likely to achieve rebalancing of the foot at the level of the deformity. Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
Question 65
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
Sports hernias may be one of the most common causes of groin pain in athletes. Resisted hip adduction is painful in the case of groin disruption. Radiation of pain into the testicles and/or adductor region is often present. Sports hernias are associated with weakening of the posterior inguinal wall. In contrast with sports hernias, traditional or classic hernias can be readily detected on physical examination. Diagnostic imaging studies are not helpful and only serve to help exclude other diagnoses. Systemic high-dose steroids or sacroiliac joint injections have no role in treatment. High success rates have been reported for laparoscopic hernia repair in athletes. Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949. Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Question 66
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?

Explanation
Following a radial nerve neurapraxia above the elbow, muscle recovery can be expected in a predictable pattern. Although variations will occur, the return of function or reinnervation usually occurs in the following order: brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum comminus, extensor digiti minimi, extensor indicis proprious, extensor pollicis longus, abductor pollicis longus, and extensor pollicis brevis. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, p 53.
Question 67
A 38-year-old woman who tripped and fell on her outstretched arm reports pain with movement. Examination reveals swelling. AP and lateral radiographs are shown in Figures 43a and 43b. Management should consist of


Explanation
The patient has a type I (Hahn-Steinthal) capitellar fracture that is best seen on the lateral radiograph. If a fracture fragment is seen proximal to the radial head, a capitellar fracture is the most likely injury because radial head fractures do not migrate proximally. The fragment is large enough for fixation. Excision is the preferred treatment for small shear osteochondral type II (Kocher-Lorenz) capitellar fractures. Closed reduction usually is not successful because of rotation of the displaced fragment. Mehdian H, McKee M: Management of proximal and distal humerus fractures. Orthop Clin North Am 2000;31:115-127.
Question 68
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?

Explanation
The image shows a view of the radiocapitellar joint from an anterior medial portal. The radial nerve lies on the elbow capsule at the midportion of the capitellum. It is at risk for injury when capsular excision is performed in this region. Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 69
A 57-year-old man with type I diabetes mellitus has had a tender, erythematous right sternoclavicular joint for the past 2 weeks. Radiographs reveal mild osteolysis without arthritic changes, within normal limits. Management should consist of

Explanation
Sternoclavicular joint sepsis is a rare condition that is most often restricted to patients who are immunocompromised, diabetic, or IV drug abusers. Examination commonly reveals a tender, painful, and possibly swollen sternoclavicular joint. If suspicion remains high following a thorough history, physical examination, radiographs, and routine blood tests, joint aspiration should be performed prior to incision and drainage or administration of antibiotics. Bremner RA: Monarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Question 70
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 71
What muscle is most often encountered during surgical approaches to C5-6?
Explanation
The omohyoid muscle crosses the surgical field from inferior lateral to anterior superior traveling from the scapula to the hyoid bone and may need to be transected. The posterior digastric crosses the field as well but higher near C3-4. The other muscles run longitudinally. Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.
Question 72
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness?
Explanation
Chronic subscapularis tendon ruptures preclude primary repair. In such instances, subcoracoid pectoralis major tendon transfers may improve function and diminish pain. The subcoracoid position of the transfer allows redirection of the pectoralis major in a direction recreating the vector of the subscapularis tendon. Shoulder fusion is a salvage procedure, and corticosteroid injection may reduce pain but will not improve function. Jost B, Puskas GJ, Lustenberger A, et al: Outcome of pectoralis major transfer for the treatment of irreparable subscapularis tears. J Bone Joint Surg Am 2003;85:1944-1951.
Question 73
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
When attempting a revision anterior cervical approach from the side opposite the original approach, it is important to evaluate the function of the vocal cords. If this evaluation reveals dysfunction of the vocal cord on the side of the original approach, then an approach on the contralateral side should not be attempted. Injury to the stellate ganglion, which causes a Horner's syndrome, should not preclude an approach on the contralateral side. While the side of the symptomatology can influence the surgeon's choice as to the side of an anterior approach, it does not preclude a certain approach. When approaching the lower cervical spine from the right side, the recurrent laryngeal nerve can cross the surgical field and should be preserved. Excessive intraoperative pressure on the esophagus can increase the incidence of dysphagia, but its incidence is no different with either approach. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
Question 74
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by

Explanation
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level. Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Question 75
Figure 49 shows an acute axial MRI scan of a left knee. What is the most likely diagnosis?

Explanation
The MRI scan shows bone bruises in the medial aspect of the patella and the lateral aspect of the lateral femoral condyle. Both of these signs are typical for a lateral dislocation of the patella with spontaneous reduction. In addition, there may be associated tearing of the medial retinaculum or distal aspect of the vastus medialis. Elias DA, White LM, Fithian DC: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Question 76
Figure 35 shows the radiograph of a 44-year-old woman with rheumatoid arthritis who reports neck pain. Below what threshold number is surgical stabilization warranted for the interval shown by the arrow?

Explanation
The posterior atlanto-dens interval represents the space available for the spinal cord and a distance of less than 14 mm is predictive of neurologic progression, thus warranting consideration for fusion, even in the absence of symptoms.
Question 77
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?




Explanation
Synovial chondromatosis results from chondroid metaplasia within the synovium. Male to female ratio is 2:1, with a peak incidence in early adult life. Radiographs can show speckled cal
Question 78
Hamstring lengthening and posterior transfer of the rectus femoris will be most successful in a patient with cerebral palsy who has which of the following gait abnormalities?
Explanation
Children with cerebral palsy typically ambulate with a crouched gait characterized by excessive flexion of the hips and knees during stance. Many patients exhibit co-contracture of the quadriceps and hamstrings, causing a stiff-knee gait. Normally, the rectus femoris fires at the initiation of swing and in terminal swing through initial contact. Prolonged activity of the rectus femoris throughout the swing phase interferes with normal knee flexion. This contributes to a stiff knee during swing phase and prevents clearance of the foot. Lengthening of the hamstrings alone will not improve foot clearance. Hamstring lengthening is contraindicated when there is hyperextension during stance. Transfer of the rectus femoris to one of the knee flexors has been shown to improve knee flexion during swing by an average of 15 degrees. This allows improved foot clearance. Gage JR, Perry J, Hicks RR, Koop S, Werntz JR: Rectus femoris transfer to improve knee function of children with cerebral palsy. Dev Med Child Neurol 1987;29:159-166.
Question 79
A 50-year-old woman has a painful hallux valgus and a painful callus beneath the second metatarsal head. A radiograph is shown in Figure 46. To correct these problems, treatment of the great toe deformity should consist of

Explanation
The patient has a significant hallux valgus and instability of the first ray, causing transfer metatarsalgia to the second metatarsal head. Therefore, the best procedure is fusion of the metatarsal cuneiform joint with soft-tissue realignment of the first metatarsophalangeal joint. This procedure provides the best chance of relieving symptoms under the second metatarsal head, as well as correcting the hallux valgus.
Question 80
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 81
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?

Explanation
Half pins placed in the AIIS are an alternative to pins placed in the iliac crest. A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated "over the top" of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 82
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?

Explanation
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humeral fractures in patients older than age 70 years. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight of more than 5 pounds must be followed to avoid loosening. Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Question 83
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?

Explanation
Emboli are created during TKA. Usually there is an increased incidence with the use of intramedullary rods that disrupt the marrow contents. These are not fat emboli per se. They are material composed of fat cells and marrow that act like pulmonary emboli to obstruct small arterioles in the lung. They are different from free fat emboli that are seen in fractures and that lead to chemical injury to the lung rather than obstructive injury. Markel DC, Femino JE, Farkas P, et al: Analysis of lower extremity embolic material after total knee arthroplasty in a canine model. J Arthroplasty 1999;14:227-232. Pell AC, Christie J, Keating JF, et al: The detection of fat embolism by transoesophageal echocardiography during reamed intramedullary nailing: A study of 24 patients with femoral and tibial fractures. J Bone Joint Surg Br 1993;75:921-925.
Question 84
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
The pectoralis major tendon inserts lateral to the biceps tendon, which runs in the bicipital groove. The primary vascular supply of the articular surface of the humeral head is derived from the anterior circumflex humeral artery, which continues into the arcuate artery once it enters the bone. The entry point is on the anterolateral aspect of the humerus just medial to the greater tuberosity within the bicipital groove. To avoid compromising circulation, the blade plate should be placed lateral to the bicipital groove and pectoralis major tendon insertion. Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Question 85
High Yield
What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?
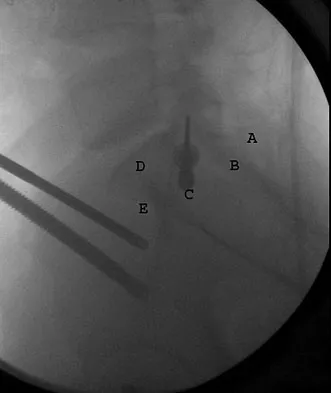
Explanation
Iliosacral screws cannot always be placed safely due to variations in pelvic anatomy. Transiliac bars are an alternative method for fixation but are placed using an open technique. A screw can be placed percutaneously through both iliac wings posterior to the posterior border of the sacrum. The starting point is visualized using a lateral C arm shot and is located on the posterior iliac crest at about the level of the S1 body where the crest has its largest area posterior to the sacrum. This area is labeled A in the figure, B represents the sacral canal, C is S1, D is the area cephalad to the iliocortical density, and E is the anterior border of the sacrum. The radiograph demonstrates a well-placed sacroiliac screw. Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: Cadaver feasibility study and preliminary clinical results. J Trauma 2007;62:357-364.
Question 86
Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
Explanation
The end point of resuscitation is adequate tissue perfusion and oxygenation. Blood lactate is the end point of anaerobic metabolism. The level of blood lactate reflects global hypoperfusion and is directly proportional to oxygen debt. Two separate prospective studies have verified a significant difference in mortality when blood lactate was used as a measure of resuscitation when compared to traditional parameters (mean arterial pressure, urine output, central venous pressure, and heart rate). Base deficit is a direct measure of metabolic acidosis and an indirect measure of blood lactate levels. It correlates well with organ dysfunction, mortality, and adequacy of resuscitation. It is easy to measure, can be obtained rapidly, and is an excellent assessment of the adequacy of resuscitation. Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Question 87
Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?



Explanation
Injury to the spinal accessory nerve can occur after penetrating trauma to the shoulder. Blunt trauma may also cause loss of trapezius function. Most commonly, surgical dissection in the posterior triangle of the neck, such as lymph node biopsy, may expose the nerve to possible damage. Surgical repair of the nerve may be considered up to 1 year after injury; after this time muscle transfer is usually associated with a better functional outcome. Steinman SP, Spinner RJ: Nerve problems in the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1013-1015.
Question 88
A 25-year-old patient who sustained multiple bilateral rib fractures, a pulmonary contusion, a left nondisplaced transtectal acetabular fracture, and a closed humerus fracture in a motor vehicle accident 2 weeks ago is transferred from another hospital. The humerus fracture has been surgically treated. There are no signs of infection, and the trauma surgeon wants to mobilize the patient as soon as possible. Radiographs are shown in Figures 15a and 15b. Management of the humerus fracture should consist of


Explanation
The radiographs show a distal third humerus fracture that is angulated, rotated, and not rigidly fixed. Rigid fixation is needed because mobilization is highly desirable to improve pulmonary function. The acetabular fracture is through the weight-bearing dome but is nondisplaced. Nonsurgical management of the acetabular fracture requires at least 6 weeks of touchdown weight bearing to minimize the forces across the hip joint. Open reduction and plate fixation would achieve anatomic reduction and immediate mobilization. A single posterolateral 4.5-mm plate or two 3.5-mm plates at 90 degrees are possible alternatives. Immediate weight bearing on a plated humerus fracture with the use of crutches or a walker has been shown to be safe and would allow touchdown weight bearing, protecting the hip. None of the other options would achieve this goal for this distal fracture.
Question 89
Figures 43a and 43b show the T1- and T2-weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?


Explanation
Osteonecrosis of the tibial plateau occurs infrequently. The symptoms are similar to those of idiopathic osteonecrosis of the medial femoral condyle and include pain and tenderness of the medial aspect of the knee and a slight synovitis. The range of motion of the knee remains within normal limits, and no gross deformity is present. Osteonecrosis of the tibial plateau is easily misdiagnosed as degenerative meniscus or osteoarthritis of the compartment of the knee. Review of lateral radiographs may reveal an osteopenic area in the subchondral bone of the medial tibial plateau. The diagnosis is more easily established with a bone scan where increased uptake of radionucleides is shown over the medial tibial plateau. In osteoarthritic involvement of the medial compartment, uptake is over both the medial femoral condyle and the medial tibial plateau, whereas if osteoarthritis involves the entire knee, uptake is diffuse over the entire joint. Radiographic findings in complex regional pain syndrome are normal as opposed to the findings for osteonecrosis or osteoarthritis. Osteosarcoma has a characteristic radiographic appearance of a bone-forming tumor. Loose bodies can derive from osteochondral fractures; a history of trauma is usually elicited. Osteoarthritis usually presents with joint space narrowing accompanying the weight-bearing pain. Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.
Question 90
A 17-year-old patient sustained a closed calcaneal fracture when he jumped off of a roof 2 years ago, and he underwent nonsurgical management at the time of injury. The patient now reports lateral hindfoot pain that is worse with weight-bearing activities. Anti-inflammatory drugs and orthoses have failed to provide relief. Coronal and sagittal CT scans are shown in Figures 36a and 36b. What is the best course of action?


Explanation
The CT scans show evidence of a lateral wall blowout and malunion without significant arthrosis of the subtalar joint. In a young patient, it is preferable to avoid a fusion and allow residual motion by performing an exostectomy that decompresses the lateral subtalar joint and peroneal tendons. Chandler JT, Bonar SK, Anderson RB, et al: Results of in situ subtalar arthrodesis for late sequelae of calcaneus fractures. Foot Ankle Int 1999;20:18-24.
Question 91
Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?

Explanation
Only three thromboembolic treatment protocols have reached Grade 1A status for the American College of Chest Physicians Guidelines for thromboembolic prophylaxis after total hip arthroplasty and total knee arthroplasty. Grade 1A evidence shows a clear benefit/risk improvement with supportive data from randomized clinical trials, which are strongly applicable in most clinical circumstances. Warfarin is recommended but at an INR level of 2 to 3. Low-molecular-weight heparin and fondaparinox are also acceptable treatment options. Aspirin, adjusted dose unfractionated heparin, and elastic compressive stockings are not recommended as stand-alone options. Colwell C: Evidence based guidelines for prevention of venous thromboembolism: Symposia. Proceedings of the 2005 AAOS Annual Meeting. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-18.
Question 92
A 77-year-old woman who underwent total knee arthroplasty 16 years ago now reports pain, swelling, and notable crepitation with range of motion. AP, lateral, and Merchant radiographs are shown in Figures 54a through 54c. What is the most likely diagnosis?



Explanation
The Merchant radiograph shows a lateral patellar shift with total polyethylene failure, resulting in a metal-on-metal bearing. This problem is associated with metal-backed patellar components. Component fixation appears solid, and no osteolysis is evident. Poss R (ed): Orthopaedic Knowledge Update 3. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 590-593. Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed metal-backed patellar component. J Arthroplasty 2000;15:938-943.
Question 93
Figure 38 shows the radiograph of a 40-year-old woman who reports severe groin pain and lack of motion of the right hip. History reveals that the patient underwent a femoral osteotomy for hip dysplasia approximately 30 years ago. Treatment should include

Explanation
Although the patient is young, a total hip arthroplasty will provide pain relief and improve her range of motion. The arthritis is too advanced for the patient to benefit from an osteotomy. In addition, periacetabular osteotomy and hip arthrodesis do not improve range of motion of the hip. It has not been established that patients with severe osteoarthritis will benefit from arthroscopic debridement of the hip.
Question 94
Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of



Explanation
The radiographs reveal a severely comminuted distal humerus fracture. A long arm cast, functional bracing, and closed reduction and percutaneous pin fixation all have a poor outcome and could result in a nonunion that will be very difficult to treat. Open reduction and internal fixation is indicated in most supracondylar humerus fractures, but total elbow arthroplasty is a good alternative in elderly patients who have multiple medical problems and when the fracture pattern may preclude stable enough internal fixation to allow postoperative motion. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Question 95
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 96
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
The acromial branch of the thoracoacromial artery courses along the medial aspect of the coracoacromial ligament and may be encountered when performing an open or arthroscopic subacromial decompression. Bleeding can be controlled by ligation of its branch from the thoracoacromial artery. The other arteries may be injured in other surgical exposures of the shoulder. Esch JC, Baker CL: The shoulder and elbow, in Whipple TL (ed): Arthroscopic Surgery. Philadelphia, PA, JB Lippincott, 1993, pp 65-66.
Question 97
A 21-year-old man with neurofibromatosis and multiple cutaneous neurofibromas has a rapidly enlarging painless mass on his buttock. Examination reveals a nontender, well-defined 6- x 6-cm soft-tissue mass that is deep to the fascia. The best course of action should be to order
Explanation
Patients with neurofibromatosis are at risk for development of soft-tissue sarcomas (most commonly malignant peripheral nerve sheath tumors). Clinical indications of development of a neurofibrosarcoma include a rapidly enlarging soft-tissue mass; therefore, this patient should be considered to have a neurofibrosarcoma until proven otherwise. MRI is superior to CT in characterizing the anatomic location of soft-tissue masses and the signal characteristics of the lesion. Areas of necrosis within the tumor may be apparent on MRI that cannot be appreciated on CT, suggesting a malignant tumor. Local imaging studies of suspected malignant tumors should be performed prior to needle or open biopsy so that the biopsy site can be excised at the time of definitive resection. Additionally, postbiopsy changes may lead to MRI artifacts that alter the interpretation of the MRI. Demas BE, Heelan RT, Lane J, Marcove R, Hajdu S, Brennan MF: Soft-tissue sarcomas of the extremities: Comparison of MR and CT in determining the extent of disease. Am J Roentgenol 1988;150:615-620.
Question 98
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the

Explanation
For the fibula (or any bone) to bow, a long-standing process needs to be present. Pressure from a rapid process would cause erosion, not allowing the bone to remodel. The other features are helpful confirmatory findings but also may be associated with aggressive processes. In this patient, the fibular deformity is caused by a sessile osteochondroma of the tibia. Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
Question 99
A 72-year-old man has had persistent pain after undergoing a hemiarthroplasty 18 months ago. Radiographs are shown in Figures 50a and 50b. What is the most likely cause of his problem?


Explanation
The radiographs demonstrate a rapid erosion of the bipolar component into the acetabulum. Although acetabular erosion is more common with unipolar hip arthroplasties, it can occur with bipolar components. Haidukewych and associates noted a very low erosion rate but none in the first 2 years. The second finding on the radiographs is the linear radiolucency progressing from the joint toward the end of the stem at the cement-bone interface suggesting chronic infection or diffuse loosening. The persistent pain since implantation also suggests chronic infection. High activity levels and osteoporosis do not lead to acetabular erosion in the first 2 years after hemiarthroplasty. While the cement technique is suboptimal, loosening and erosion should not be expected from this alone. An oversized bipolar head would extrude and not erode. Haidukewych GJ, Israel TA, Berry DJ: Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res 2002;403:118-126. Lestrange NR: Bipolar hemiarthroplasty for 496 hip fractures. Clin Orthop Relat Res 1990;251:7-19.
Question 100
A 21-year-old man has had right groin pain for the past year. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 50a through 50e. What is the most likely diagnosis?





Explanation
The pathology demonstrates a very cellular chondroid matrix with multinucleated forms, atypia, and myxomatous regions. This is most consistent with a myxoid chondrosarcoma. The radiograph shows a well-circumscribed lesion in the superior and medial aspect of the right acetabulum. The CT and MRI scans confirm these same findings with no evidence of matrix mineralization or significant surrounding edema. Unfortunately, in this location with this appearance, the radiographic differential diagnosis includes all the diagnoses listed. Terek RM: Recent advances in the basic science of chondrosarcoma. Orthop Clin North Am 2006;37:9-14. Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
