Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?

Explanation
The child has an up-to-date tetanus; therefore, a booster is not recommended. Pseudomonas coverage is most likely not needed because the child was barefoot. It is too early to evaluate for abscess or osteomyelitis with MRI, and a formal debridement is rarely indicated without signs of an abscess or a retained foreign body. Radiographs with soft-tissue penetration should be obtained to check for a retained foreign body. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-205.
Question 2
Figures 25a and 25b show the radiograph and MRI scan of a 7 1/2-year-old boy who has been limping for 1 year. His pain has worsened over the past 2 weeks, and his parents note swelling over the dorsum of the foot for the past 4 days. Examination reveals no fever, and laboratory studies show a WBC of 6,700/mm3, an erythrocyte sedimentation rate of 26 mm/h, and a normal C-reactive protein level. What is the most likely diagnosis?


Explanation
The diagnosis of tuberculous osteomyelitis in children is often delayed. In one series of 23 children, the average interval between the onset of symptoms and definite diagnosis was 4.3 months. In these patients, the presenting signs and symptoms were found to be mild, with the most common signs being localized swelling (69.6%) and a painful disability of the involved limbs (65.2%). A mild elevation of the erythrocyte sedimentation rate may be present, but the C-reactive protein level is usually normal. In patients who have osteoarticular tuberculosis, an MRI scan generally shows large intra-articular effusions, periarticular osteoporosis, and gross thickening of the synovial membrane. Differential diagnosis between tuberculosis and pyogenic arthritis is difficult, and an accurate diagnosis usually requires biopsy of synovial tissue. Aspiration of synovial fluid often results in insufficient information to make a diagnosis. Treatment generally consists of surgical debridement and combined antituberculous chemotherapy with isoniazid, ethambutol, and rifampin. Wang MN, Chen WM, Lee KS, Chin LS, Lo WH: Tuberculous osteomyelitis in young children. J Pediatr Orthop 1999;19:151-155.
Question 3
Figures 37a and 37b show radiographs of a 24-year-old man who has a humeral bone lesion that was found during a screening chest radiograph. He denies any symptoms despite leading a very active lifestyle. What is the most likely diagnosis?


Explanation
The radiographs reveal a geographic, diaphyseal lesion with very subtle cortical expansion, cortical thinning, relatively sharp demarcation, and angular rather than rounded borders, suggesting a fibrous bone lesion. This lesion demonstrates the classic ground glass appearance of fibrous dysplasia. Ewing's sarcoma, metastases, and aneurysmal bone cyst all typically have a more aggressive appearance. Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Question 4
Figures 18a and 18b show the radiographs of a patient who has pain with walking. On careful questioning, it is determined that the discomfort occurs at push-off, or when the patient attempts to climb stairs. What nonsurgical option is most likely to ameliorate the symptoms?


Explanation
The patient has a malunion of an attempted open reduction of a Lisfranc dislocation. The pain occurs during the terminal stance phase of gait as load is being transferred from the hindfoot to the forefoot. The bending moment can be best neutralized with shoe modification with a cushioned heel and rocker sole, which best unloads the tarsal-metatarsal junction. Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Question 5
An 8-year-old boy sustains nondisplaced midshaft fractures of the tibia and fibula after being struck by a car while he was riding his bicycle. No other injuries are noted, but the patient reports pain with passive motion of his toes. His neurovascular examination is otherwise normal. What is the best course of action?

Explanation
Pain with passive motion of the toes is a recognized early sign of increased compartment pressures. At a minimum, a baseline evaluation of the leg compartment pressures should be obtained. While it is normal for the patient to have pain related to the associated muscle contusions, any significant concerns should be addressed immediately in light of the severe consequences likely when a compartment syndrome occurs. Mubarak SJ, Owen CA, Hargens AR, et al: Acute compartment syndromes: Diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am 1978;60:1091-1095.
Scientific References
-
:
Question 6
A 58-year-old woman has a fracture through a metacarpal lesion after a motor vehicle accident. She denies any preinjury symptoms and the fracture heals uneventfully. Based on the radiograph and MRI scans shown in Figures 22a through 22c obtained following fracture healing, follow-up management should consist of



Explanation
Enchondromas are the most common benign skeletal lesions identified in the bones of the hand. Most are incidentally found or initially become clinically evident after a pathologic fracture. If the patient has a fracture, the hand is immobilized until union. If the lesion is large and further pathologic fractures are expected, then an intralesional curettage and grafting procedure may be warranted. In this patient, the lesion has not significantly altered the size, shape, or morphology of the involved metacarpal head and recurrent fracture is unlikely. Observation with follow-up radiographs is considered appropriate management. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 213-228.
Question 7
Which of the following mechanisms is considered the most common cause of failure of osteoarticular allografts used for articular reconstruction?

Explanation
Mechanical loosening and infection can occur as complications after surgery, but the most common cause of osteoarticular allograft failure is graft collapse during revascularization. Clinical rejection because of an immune response is an unusual means of failure. Meyers MH, Akeson W, Convery FR: Resurfacing of the knee with fresh osteochondral allograft. J Bone Joint Surg Am 1989;71:704-713.
Question 8
A 25-year-old left hand-dominant man has severe left shoulder pain after being involved in a high-speed motor vehicle accident. Examination reveals that he is unable to move the left shoulder. His neurovascular status is intact in the entire left upper extremity. A radiograph is shown in Figure 19. What is the most appropriate surgical management of this injury?

Explanation
In this young patient, every attempt must be made to retain the native proximal humerus; therefore, open reduction and internal fixation should be attempted of both the articular segment and tuberosities to the humeral shaft. This is best accomplished through an open approach. Shoulder arthroplasty should be reserved for the elderly and for failed internal fixation. Ko JY, Yamamoto R: Surgical treatment of complex fractures of the proximal humerus. Clin Orthop Relat Res 1996;327:225-237.
Question 9
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?

Explanation
Arthroscopic versus open distal clavicle excision has the advantage of allowing evaluation of the glenohumeral joint arthroscopically prior to moving into the subclavicular and subacromial space to perform the distal clavicle excision. This can be of value in both confirming the diagnosis as well as avoiding diagnostic errors. Berg and Ciullo showed that in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament. Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Question 10
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?

Explanation
Even though the patient has a grade 3 ankle ligament injury, studies have shown that 95% of patients with a grade 3 injury that may include a complete tear of the ligaments will heal successfully with conservative functional management. Extensive diagnostic evaluation with stress radiographs, CT, and MRI is not indicated. Surgical reconstruction is not indicated because of the overwhelming success of conservative management; however, in the few patients where late instability develops, surgical reconstruction offers an excellent outcome. Carne P: Nonsurgical treatment of ankle sprains using the modified Sarmiento brace. Am J Sports Med 1989;17:253-257.
Question 11
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?

Explanation
Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH. Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
Question 12
A 9-year-old child sustains a proximal tibial physeal fracture with a hyperextension mechanism. What structure is at most risk for serious injury?

Explanation
The most serious injury associated with proximal tibial physeal fracture is vascular trauma. The popliteal artery is tethered by its major branches near the posterior surface of the proximal tibial epiphysis. During tibial physeal displacement, the popliteal artery is susceptible to injury. Injuries to the other structures are less common.
Question 13
Figure 42 is a transverse MRI scan of the left shoulder. The arrow points to which of the following structures?

Explanation
The figure shows an axial image of the shoulder immediately inferior to the coracoid process. The subscapularis tendon, which can be traced from the myotendinous junction, is torn and detached from its lesser tuberosity attachment on the humerus. Lateral to the lesser tuberosity, the bicipital groove is empty. The arrow points to the subluxated biceps tendon. Superficial fibers of the subscapularis tendon are contiguous with the biceps retinaculum, which covers the bicipital groove and hold the biceps tendon in place. The vast majority of subscapularis tendon tears result in disruption of the biceps retinaculum with resultant subluxation of the tendon. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Scientific References
-
:
Question 14
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?

Explanation
The lesion is typical of a subungual exostosis, which is most often found on the medial aspect of the great toe in children and young adults. The diagnosis is confirmed on radiographs and usually requires excision for relief. Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79. Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Question 15
High Yield
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?

Explanation
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high energy humeral shaft fractures. J Hand Surg 2004;29:144-147. Foster RJ, Swiontkowski MR, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 16
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?

Explanation
The radiograph shows multiple wide physes, consistent with a diagnosis of rickets. A low serum phosphorous level and an elevated alkaline phosphatase level are the hallmarks in diagnosing familial hypophosphatemic Vitamin D-resistant rickets. Serum calcium is usually normal or low normal. This disease is inherited as an X-linked dominant trait and usually presents at age 18 to 24 months. The disease results from a poorly defined problem with renal phosphate transport in which normal dietary intake of vitamin D is insufficient to achieve normal bone mineralization. Renal tubular dysfunction is associated with urinary phosphate wasting. Treatment involves oral phosphate supplementation, which can cause hypocalcemia and secondary hyperparathyroidism. To prevent associated problems, high doses of Vitamin D are administered. While obtaining a scanogram may be clinically indicated in an associated limb-length discrepancy, and subsequent corrective surgery may be indicated, either of these choices would not be the first course of action. An orthosis may slow the progression of genu varum in this disorder but is less important than establishing the correct diagnosis to begin pharmacologic treatment. This amount of varum and tibial bowing far exceeds the normal limits of physiologic genu varum. Skeletal dysplasias usually are not associated with abnormal laboratory values. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743.
Question 17
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of


Explanation
The MRI scans show a mesoacromion with tendonopathy of the supraspinatus. The history and physical findings indicate that the patient has a symptomatic os acromiale. Simple excision of the unstable os acromiale has not yielded consistently good results. Meticulous internal fixation using tension banding with cannulated screws and autologous bone grafting has shown good results for this problem. Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Question 18
A 12-year-old girl who has a history of frequent tripping and falling also has bilateral symmetric hand weakness, high arched feet, absent patellar and Achilles tendon reflexes, and excessive wear on the lateral border of her shoes. She reports that she has multiple paternal family members with similar deformities. She most likely has a defect of what protein?
Explanation
The girl shows clinical features of hereditary motor sensory neuropathy type 1, Charcot-Marie-Tooth disease. The most common type of this autosomal-dominant disease is due to an underlying defect in the gene coding for peripheral myelin protein-22 on chromosome 17. Many other less common mutations have been identified in this family of neuropathies. Dystrophin is a protein that is abnormal in Duchenne's muscular dystrophy, which affects males and is diagnosed earlier. Type I collagen is defective in osteogenesis imperfecta. Alpha-L-iduronidase is defective in mucopolysaccharidosis type I, Hurler's syndrome. Defective cartilage oligomeric matrix protein is associated with some forms of multiple epiphyseal dysplasia. Patel PI, Roa BB, Welcher AA, et al: The gene for the peripheral myelin protein PMP-22 is a candidate for Charcot-Marie-Tooth disease type 1A. Nat Genet 1992;1:159-165.
Question 19
Figure 47 shows the radiograph of a 2-day-old girl who has been referred for swelling and limited use of the right upper extremity. The second of twins, the infant was breech and delivered with forceps at age 38 weeks, weighing 5.37 lb. Difficulty in moving the arm was noted shortly after birth. Examination shows no active motion of the shoulder, elbow, or wrist. Active finger flexion and extension are present. The elbow is mildly swollen, and passive motion shows lack of full extension of 20 degrees, lack of full flexion of 15 degrees, and no restriction of pronation or supination. What is the most likely diagnosis?

Explanation
Fractures involving the entire distal humeral physis may be a complication of a difficult delivery. Basing the diagnosis on radiographs can be difficult at this age because the secondary ossification center of the lateral condyle has not developed. The key to the diagnosis is the constant relationship of the radius and ulna, with medial and posterior displacement of the forearm relative to the humerus. An ultrasound can be obtained to confirm the diagnosis in newborns. Because the fracture is through cartilage, examination may reveal only mild swelling, and crepitation may be muffled or not apparent. The lack of apparent active motion of the shoulder, elbow, and wrist is secondary to pseudoparalysis. Child abuse is a common mechanism of this injury in a child who is age 1 month to age 3 years. Beaty JH, Wilkins KE: Fractures involving the entire distal humeral physis, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, vol 3, pp 790-801. Dias JJ, Lamont AC, Jones JM: Ultrasonic diagnosis of neonatal separation of the distal humeral epiphysis. J Bone Joint Surg Br 1988;70:825-828.
Question 20
An 83-year-old woman reports pain in her left middle finger after a minor injury. Laboratory studies show a WBC count of 7,000/mm3, an erythrocyte sedimentation rate of 3 mm/h, a uric acid of 10.4 mg/dL, and a normal serum protein electrophoresis. Radiographs are shown in Figures 49a and 49b. A core biopsy specimen is shown is Figure 49c. In addition to treatment of the finger fracture, treatment should include



Explanation
This clinical picture is most consistent with periarticular erosions from gout. The patient has multiple periarticular lytic lesions in the hand. The laboratory studies show an elevated serum uric acid level, and the biopsy specimen demonstrates acute and chronic inflammation with prominent clefts. Therefore, the preferred treatment is systemic control of her gout. Radiation therapy, chemotherapy, and/or amputation should be considered for a malignancy; however, the pathology does not demonstrate any evidence of pleomorphism, high nuclear-to-cytoplasmic ratio, nuclear atypia, or mitotic activity. Antibiotics for an infectious process is a consideration, but the minimal elevation in the WBC count and erythrocyte sedimentation rate does not support an infectious process. Wise CM: Crystal-associated arthritis in the elderly. Clin Geriatr Med 2005;21:491-511.
Question 21
A 37-year-old man has left shoulder pain and weakness. Coronal T1- and axial T2-weighted MRI scans are shown in Figures 17a and 17b. The biopsy specimen is shown in Figure 17c. What is the most likely diagnosis?



Explanation
A ganglion cyst arising from the posterior labrum of the shoulder is a known cause of suprascapular nerve impingement. The MRI characteristics of low-signal intensity on T1 and high-signal intensity on T2 are seen in lesions with a high fluid content. The histology shows a cavity with a thin fibrous lining. Ferrick MR, Marzo JM: Suprascapular entrapment neuropathy and ganglion cysts about the shoulder. Orthopedics 1999;22:430-434.
Question 22
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?

Explanation
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended. Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 23
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?


Explanation
A headfirst slide with the arm extended can injure the posterior shoulder. Winging of the scapula is dynamic and is considered a compensatory effort to prevent subluxation; it is not related to nerve injury. Posterior glenohumeral subluxation can be present during the initiation of a bat swing. Rotator cuff function, interval tears, and superior labrum tears can be painful but do not produce winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 24
A 15-year-old girl who competes in gymnastics has immediate pain and giving way of the left elbow after falling from the uneven parallel bars and landing on her outstretched arms. Examination reveals swelling and tenderness about the elbow, especially over the medial side. Measurement of elbow motion shows 0 degrees to 125 degrees of flexion, and valgus stress at the elbow is painful. AP, lateral, and stress radiographs are shown in Figures 9a through 9c. Management should consist of



Explanation
While many low-demand patients with injuries to the ulnar collateral ligament can be treated nonsurgically, Jobe and associates described two situations in which ulnar collateral ligament reconstruction is indicated: (1) an acute complete rupture in a competitive athlete who uses the upper extremities extensively and who wishes to remain active; and (2) chronic pain or instability that does not improve after at least 3 months of nonsurgical management. Rarely is direct surgical repair of the ligament possible or able to withstand the valgus stresses applied to the elbow. Most authors recommend surgical reconstruction of the ulnar collateral ligament using a palmaris longus, plantaris, or fourth toe extensor tendon from the fourth autograft. Andrews JR, Jelsma RD, Joyce ME, et al: Open surgical procedures for injuries to the elbow in throwers. Oper Tech Sports Med 1994;4:109-133. Jobe FW, Kvitne RS: Elbow instability in the athlete. Instr Course Lect 1991;40:17-23.
Question 25
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?

Explanation
The MRI scan shows significant dural ectasia, which is seen in more than 60% of patients with Marfan syndrome. It is also relatively common in patients with neurofibromatosis, but this patient has no skin lesions. It has also been described in Ehlers-Danlos syndrome but is less common. Ahn NU, Sponseller PD, Ahn UM, Nallamshetty L, Kuszyk BS, Zinreich SJ: Dural ectasia is associated with back pain in Marfan' syndrome. Spine 2000;25:1562-1568.
Question 26
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?

Explanation
Focal calcifications causing small radiopacities are found in 15% to 20% of synovial sarcomas. Their irregular contours differentiate them from the phleboliths found in a benign hemangioma. Ewing's sarcoma, clear cell sarcoma, and malignant fibrous histiocytoma do not commonly have calcifications within the lesions. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 761.
Question 27
Initial repair of the large U-shaped rotator cuff tear shown in Figure 12 consists of closing the tear side-to-side to take advantage of margin convergence. The most significant biomechanical consequence of this repair step results in

Explanation
Margin convergence refers to the phenomenon that occurs with side-to-side closure of large U- or L-shaped rotator cuff tears in which the free margin of the tear converges toward the greater tuberosity as the side-to-side tear progresses. The creation of the converged cuff margin creates decreased strain in the free margin of the repaired cuff, resulting in a decreased strain in the repair sutures. While the size of the humeral head defect is made smaller with side-to-side closure, biomechanically, this is less significant. The mild increase in thickness of the repair at the side-to-side margin is less important than a reduction in stress in the repaired tissue. Stress in the crescent cable region of the cuff actually increases and becomes more physiologic in transmitting force from the cuff to the greater tuberosity. Burkhart SS: A stepwise approach to arthroscopic rotator cuff repair based on biomechanical principles. Arthroscopy 2000;16:82-90.
Question 28
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?

Explanation
The standard approach to the volar aspect of the distal radius is the Henry approach. Following incision of the skin and subcutaneous tissues, the forearm fascia is incised. The radial artery and venae comitantes lie in the interval between the tendons of the flexor carpi radialis muscle and the brachioradialis muscle. This interval is developed, and the radial artery and veins are retracted in a radial direction. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 29
A patient with an acromioclavicular dislocation has a very prominent distal clavicle. Examination reveals that the deformity increases rather than reduces with an isometric shoulder shrug. Which of the following structures is most likely intact?

Explanation
Severely displaced acromioclavicular injuries disrupt the deltotrapezial fascia and muscular origin in addition to the ligaments (acromioclavicular and coracoclavicular or trapezoid and conoid). When the deltoid is still attached to the clavicle, an isometric shoulder shrug will tend to reduce the displacement. When the deltoid is detached but the trapezius is attached, this manuever will increase the deformity and surgery may be indicated.
Question 30
High Yield
A 36-year-old woman is placed in a short arm cast for a nondisplaced extra-articular distal radius fracture. Seven weeks later she notes the sudden inability to extend her thumb. What is the most likely cause of her condition?

Detailed Explanation
A recent review of 200 consecutive distal radius fractures noted that the overall incidence of extensor pollicis longus rupture was 3%. The causes are believed to be mechanical irritation, attrition, and vascular impairment. The fracture is usually nondisplaced and the patient notes weeks to months after injury the sudden, painless inability to extend the thumb. Treatment involves extensor indicis proprius tendon transfer or free palmaris longus tendon grafting. Skoff HD: Postfracture extensor pollicis longus tenosynovitis and tendon rupture: A scientific study and personal series. Am J Orthop 2003;32:245-247. Bonatz E, Kramer TD, Masear VR: Rupture of the extensor pollicis longus tendon. Am J Orthop 1996;25:118-122.
Question 31
A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
Explanation
Nickel allergy is not an infrequent preoperative finding. The ramifications of such allergies in arthroplasty patients are poorly understood at this time. Stainless steel and cobalt-chromium alloys contain relatively high concentrations of nickel. Titanium, oxidized zirconium, and polyethylene do not contain significant amounts of nickel. Titanium is not a good surface for the articulating portion of the femoral component because of its propensity for metallosis. Oxidized zirconium is the only suitable femoral component for patients allergic to nickel. A modular titanium tibial component or an all-polyethylene tibial component would be satisfactory for these patients. Laskin RS: An oxidized Zr ceramic surfaced femoral component for total knee arthroplasty. Clin Orthop 2003;416:191-196.
Question 32
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
The suprascapular nerve passes through the suprascapular notch and the spinoglenoid notch before innervating the infraspinatus muscle. At both locations, the suprascapular nerve is prone to nerve compression, which often results from a ganglion cyst. The other anatomic locations are not associated with suprascapular nerve impingement. Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Question 33
An 81-year-old man with severe low back pain reports right extensor hallucis longus and anterior tibialis weakness and difficulty urinating over the past 24 hours. He has a temperature of 101 degrees F (38.3 degrees C). MRI scans are shown in Figures 31a and 31b. Management should consist of


Explanation
An epidural abscess with neurologic deficit represents a medical and surgical emergency. The prognosis is related to the timeliness of diagnosis and treatment. Once identified, the primary treatment is surgical decompression of the abscess, followed by organism-specific antibiotics. In the absence of a significant anterior process such as diskitis or vertebral osteomyelitis, lumbar epidural abscesses generally can be drained through a posterior approach. Delayed stabilization usually is not required unless, in the course of decompression, removal of too much of the facets creates an instability; this is an uncommon occurrence. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Question 34
A 40-year-old man fell 10 feet from a tree and sustained the closed isolated injury shown in Figures 35a and 35b. Management consists of splinting. At his 2-week follow-up visit, he clinically passes the wrinkle test. He agrees to open reduction and internal fixation. What is the best surgical approach to obtain anatomic reduction and limit wound dehiscence?


Explanation
The approach to the calcaneus has evolved from several different patterns, driven by a high wound complication rate of 10%. The current extensile lateral approach was described by Zwipp and associates in 1988. The surgical exposure uses an L-shaped incision, with the vertical component positioned one half a finger's breath anterior to the Achilles tendon and extending distally to the junction of the lateral skin and the plantar skin. Borrelli and Lashgari mapped the angiosome of the lateral calcaneal flap and found that the major arterial blood supply to this flap consisted of three arteries: the lateral calcaneal artery, the lateral malleolar artery, and the lateral tarsal artery. The lateral calcaneal artery appeared to be responsible for most of the blood supply to the corner of the flap. This was found 1.5 cm anterior to the Achilles tendon. Division of this artery with inaccurate placement of the vertical limb of the incision can cause ischemia of the lateral skin flap. Borrelli J Jr, Lashgari C: Vascularity of the lateral calcaneal flap: A cadaveric injection study. J Orthop Trauma 1999;13:73-77. Freeman BJC, Duff S, Allen PE, et al: The extended lateral approach to the hindfoot: An anatomical basis and surgical implications. J Bone Joint Surg Br 1998;80:139-142.
Question 35
A 42-year-old man reports the recent onset of right hip pain. A radiograph and MRI scan are shown in Figures 38a and 38b. A WBC count, erythrocyte sedimentation rate, and hip aspiration are within normal limits. Management should now consist of


Explanation
Transient osteoporosis of the hip is an uncommon problem, usually affecting women in the last trimester of pregnancy and middle-aged men. Symptoms include pain in the involved hip with temporary osteopenia; however, there is no joint space involvement. In this patient, the imaging findings are consistent with transient osteoporosis. Short TR/TE (repetition time/echo time) images reveal diffusely decreased signal intensity in the femoral head and intracapsular region of the femoral neck. Increased signal intensity is seen with increased T2-weighting. Within a few months, the pain, as well as the imaging findings, will completely resolve without intervention. Distinguishing the diffuse features of transient osteoporosis of the hip from the segmental findings of osteonecrosis is essential. Unlike transient osteoporosis of the hip, osteonecrosis will have a double-density signal on MRI and may progress radiographically. Surgical intervention and oral corticosteriods are not indicated for treatment. Protected weight bearing until the pain resolves may decrease symptoms while the transient osteoporosis resolves. Potter H, Moran M, Scheider R, et al: Magnetic resonance imaging in diagnosis of transient osteoporosis of the hip. Clin Orthop 1992;280:223-229. Bijl M, van Leeuwen MA, van Rijswijk MH: Transient osteoporosis of the hip: Presentation of typical cases for review of the literature. Clin Exp Rheumatol 1999;17:601-604.
Question 36
Metal-on-metal articulation has been reintroduced because of concern about polyethylene wear. This type of articulation is considered favorable because
Explanation
The improvements in metal-on-metal bearing surfaces come from the nonlinear wear rate and smaller particle size of the high carbon wrought material. Extremely low rates of wear have been demonstrated with high carbon metal-on-metal implants. There is no significant electrochemical effect of mating two like materials in vivo.
Question 37
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?

Explanation
Radiation therapy is commonly used as an adjuvant in the treatment of soft-tissue sarcomas, but a controversy exists whether it should be preoperative or postoperative. Radiation therapy can be given prior to or following resection of the tumor. Postoperative radiation is usually given in a higher dose to a larger treatment field. This commonly results in a higher incidence of fibrosis and lymphedema. There is no statistical difference in local recurrence rate between the two radiation treatment plans. Neuropathy is more commonly a complication of chemotherapy. Preoperative radiation therapy has been shown to have a higher wound complication rate than postoperative radiation. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Question 38
Factors contributing to an increased risk of hip fracture include reduced bone mineral density of the femoral neck, cognitive status of the individual, and
Explanation
The etiology of hip fractures in the elderly is multifactorial, and intervention and prevention can occur at multiple points. Events leading to hip fracture from a fall include fall initiation (during which the individual's neuromuscular status, cognitive status, and vision come into play along with environmental hazards); fall descent (fall direction toward the side being the most influential, energy content of the fall, and fall height, along with muscle activity of the muscles of the thigh); impact (impact location, soft-tissue attenuation such as from trochanteric padding or from overlying fat, impact surface, and muscle activity); and the structural capacity of the femur (bone mineral density, bone geometry, and bone architecture). Hayes and Myers noted that striking the ground in a stiff state with the trunk muscles contracted actually increased the peak impact force, whereas falling in a relaxed state actually reduced peak impact force. Flexion of the trunk at impact had no bearing on the impact force. Direction of the fall was important; falls to the side, not forward, were associated with an increased risk of hip fracture. Increased muscle activity about the hip is thought to be associated with spontaneous fractures of the hip and may actually account for up to 25% of hip fractures; however, it is not related to fractures resulting from a fall.
Question 39
During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?

Explanation
Positioning of the femoral and tibial components is a common cause of early failure of total knee arthroplasty. Two modes of possible position are raising or lowering the joint line from its anatomic level. Raising or lowering the joint line beyond an established threshold can cause limited range of motion, poor patellar function, and possible instability. It has been determined that a threshold of approximately 8 mm provides consistently good results after knee arthroplasty.
Question 40
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?

Explanation
The avulsed fragment represents the origin of the rectus femoris from the anterior inferior iliac spine and the brim of the acetabulum. Avulsion of the anterior inferior iliac spine is much less common than avulsion of the anterior superior iliac spine with its origin of the sartorius. The origin of the gluteus minimus is from the outer cortex of the iliac wing and has not been reported as a source of bony avulsion. The hip capsule is composed of the ischiofemoral and pubofemoral ligaments, in addition to the iliofemoral ligament. The pelvic attachment of the ischiofemoral ligament is from the ischial part of the acetabulum posteriorly, while the pubofemoral ligament attaches to the pubic portion inferiorly. Technically, ligaments do not have origins and insertions as muscle tendon groups do, but have attachment sites. Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 41
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?

Explanation
Laminoplasty or any posterior decompressive procedure is contraindicated in patients with cervical spondylotic myelopathy and cervical kyphosis. The residual kyphotic posture of the cervical spine results in persistent spinal cord compression. The other choices are not contraindications for laminoplasty. Concomitant cervical radiculopathy can be addressed at the time of laminoplasty with a keyhole foraminotomy. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 42
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?

Explanation
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region. Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 43
A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
Explanation
Following any closed fracture, the most important determinant for the timing of surgery is the condition of the soft tissues and especially the skin. The best determinant of appropriate soft-tissue condition is the presence of wrinkling of the skin (wrinkle sign) at the site of the incision. A wrinkle sign is present when all the interstitial edema has left the skin; this may take up to 14 to 21 days of elevation. Any abrasion must be epithelialized so that there are no bacteria left at the site. To date, no other method of soft-tissue viability measurement has been shown to be of any clinical benefit. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Question 44
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
A widened medial clear space indicates instability caused by an associated tear of the deltoid ligament; therefore, nonsurgical management is not warranted. Weber type B distal fibular fractures without a deltoid tear have a medial clear space of < 4 mm, even under stress, and may be successfully treated nonsurgically. The presence of medial hindfoot ecchymosis and medial ankle tenderness is not fully indicative of medial soft-tissue instability; however, these findings may indicate a deltoid injury and should raise suspicion of an unstable fracture injury pattern. Stress testing is necessary to demonstrate the presence or absence of instability. A small amount of comminution is also cause for increased suspicion of an unstable pattern; however, it is not a direct contraindication when considering nonsurgical management. Two millimeters of fibular displacement without lateral shift of the talus is an acceptable position when considering nonsurgical management of Weber type B distal fibular fractures. Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Question 45
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?

Explanation
Progressive weakness is a common sign with a large differential diagnosis. Nerve, muscle, and joint problems should be excluded when a patient has diffuse weakness and atrophy. Fascioscapulohumeral dystrophy is a rare disease characterized by facial muscle weakness and proximal shoulder muscle weakness. The weakness is usually bilateral, and scapular winging is common. If the scapular winging becomes pronounced, elevation of the shoulder can be affected. In severe cases, scapulothoracic fusion or pectoralis muscle transfer to the scapula may be indicated. Duchenne muscular dystrophy is typically severe and progressive. The other diagnoses are not compatible with the history or the physical findings. Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Question 46
Which of the following findings is considered the strongest indication for surgical treatment of a mallet fracture of the distal phalanx?
Explanation
The majority of mallet fractures can be treated nonsurgically with a distal interphalangeal joint extension splint. Excellent results can be obtained in most patients with splinting alone. The fragment size, amount of displacement, and degree of articular incongruity usually do not affect final outcome, as long as the joint is reduced. Surgical fixation takes on several forms but is fraught with complications including skin/wound problems, loss of fixation, nonunion, and stiffness of the distal interphalangeal joint. Volar subluxation of the distal phalanx remains the primary indication for surgical treatment. Green DP, Butler TE Jr: Fractures and dislocations in the hand, in Rockwood CA, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 621-623.
Question 47
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?

Explanation
The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 48
A 37-year-old patient with type I diabetes mellitus has a flexor tenosynovitis of the thumb flexor tendon sheath following a kitchen knife puncture wound to the volar aspect of the thumb. Left unattended, this infection will likely first spread proximally creating an abscess in which of the following spaces of the palm?

Explanation
Flexor tenosynovitis of the thumb flexor tendon sheath can spread proximally and form an abscess within the thenar space of the palm. The flexor pollicis longus tendon does not pass through the central space of the palm or the hypothenar space of the palm. The flexor pollicis longus tendon does pass through the carpal tunnel, but this is not a palmar space. The three palmar spaces include the hypothenar space, the thenar space, and the central space. The posterior adductor space would likely only be involved secondarily after spread from a thenar space infection. Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 478-479.
Question 49
When posterior fusion with instrumentation to the sacrum is used to treat adult scoliosis, what instrumentation technique best increases the chance of a successful lumbosacral fusion?
Explanation
As the chance of success of lumbosacral fusion increases with the stiffness and rigidity of the construct, fixation and stiffness improve with fixation into both the upper sacrum and the ilium. In a review of individuals treated with long constructs to the pelvis for adult scoliosis, Islam and associates reported that the rate of pseudarthrosis was significantly lower with sacral and iliac fixation compared with sacral fixation alone or iliac fixation alone. Iliac screws provide significant fixation anterior to the instantaneous axis of rotation for flexion and extension, as well as provides resistance to lateral bending and rotational forces. Numerous biomechanical studies support the concept of increasing biomechanical stabilization with increased fixation from the sacrum to the ilium. Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173. O'Brien N, et al: Sacral pelvic fixation and spinal deformity, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 601-614.
Question 50
A patient who sustained a knife wound to the axilla 4 months ago now has profound interosseous wasting and generalized hand weakness. A brachial plexus injury is likely at which of the following locations in Figure 29?

Explanation
Penetrating sharp wounds in proximity to major nerve or vascular structures should always be acutely explored. Because this patient did not seek treatment for a potentially treatable injury, interosseous wasting implies injury to the C8 and T1 nerve roots that contribute to ulnar nerve function. The most likely location for the brachial plexus injury is the location marked L or the inferior trunk. A wrist drop that is the result of radial nerve dysfunction would be expected with an injury at K or O. An upper brachial plexus palsy with loss of elbow flexion and shoulder abduction would be expected with an injury at B. A loss of elbow flexion alone would be expected following an injury at C. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29. Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1255-1272.
Question 51
The carpal tunnel canal is narrowest (smallest cross-sectional area) at what level?
Explanation
The carpal tunnel canal has an hourglass shape in the coronal plane and is narrowest at the level of the hook of the hamate. Cobb TK, Dalley BK, Posteraro RH, et al: Anatomy of the flexor retinaculum. J Hand Surg Am 1993;18:91-99.
Question 52
Which of the following is a true statement regarding thoracic disk herniations?
Explanation
Symptomatic herniations of the thoracic spine are much less common than those of the cervical or lumbar region. They tend to occur most commonly during the third to fifth decades of life and although they can be found at all levels, they are most common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals. Shah RP, Grauer JN: Thoracoscopic excision of thoracic herniated disc, in Vaccaro AR, Bono CM (eds): Minimally Invasive Spine Surgery. New York, NY, Informa Healthcare, 2007, pp 73-80.
Question 53
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of

Explanation
Excision of the affected mucoid degenerative area is considered appropriate management in the Blazina classification system. A finding of phase III indicates persistent pain with or without activities, as well as deterioration of performance. With the appearance of the mucoid degeneration and the vigorous activity level of the intercollegiate basketball player, it is unlikely that nonsurgical management will provide adequate relief. When excising the affected degenerative area, care must be taken to retain normal tendon fibers. The defect in the patellar tendon is closed with absorbable sutures, as is the paratenon. Postoperative rehabilitation involves initial mobilization extension, with progressive range-of-motion and mobilization exercises as tolerated and weight bearing as tolerated. Open chain and isokinetic exercises are delayed until full range of motion and mobility is obtained, generally within 4 weeks. A return to activities is achieved by 80% to 90% of athletes, although there may be occasional activity-related aching for 4 to 6 months after surgery. Blazina ME, et al: Jumper's knee. Orthop Clin North Am 1973;4:665. Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper's knee. Am J Sports Med 1984;12:375-380. Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Question 54
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of

Explanation
In a subgroup of patients with monoarticular JRA and a limb-length discrepancy that developed before the age of 9 years, Simon and associates showed that a subsequent growth deceleration on the affected side may correct a large part of the difference in length. This possibility would make surgery unnecessary and should prompt further observation. Simon S, Whiffen J, Shapiro F: Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Joint Surg Am 1981;63:209-215.
Question 55
The primary purpose of obtaining the radiograph shown in Figure 9 is to assess

Explanation
The radiograph shows a faux profil view of the hip. The primary purpose of this view is to evaluate anterior coverage of the femoral head. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 56
Etanercept is a recombinant genetically engineered fusion protein used to treat rheumatoid arthritis. What is its mode of action?
Explanation
Etanercept is a molecule consisting of the Fc portion of IgG fused to the extracellular domain of the p76 human THF-a receptor. It is soluble and binds TNF-a. Infliximab is the monoclonal antibody that binds TNF-a. IL-1 receptor antagonists are still in development. Leflunomide is a drug that inhibits pyrimidine synthesis and is similar to methotrexate as an antimetabolite.
Question 57
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
Although thoracic disk herniations have been reported at all levels of the thoracic spine, more than two thirds are found at T9-T12, which is the more mobile lower third of the thoracic region. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Question 58
Figures 43a and 43b show the clinical photographs of a 4-month-old child with bilateral popliteal pterygium. The fixed knee contractures measure 100 degrees bilaterally. What future treatment is most likely to successfully correct this deformity?


Explanation
Congenital popliteal webbing with contractures of 60 degrees is a difficult deformity to correct. The anatomy of the web is of considerable importance. MRI can delineate the extent of the posterior fibrous band that often stretches from the ischium to the calcaneus. The sciatic nerve, usually shortened, most often runs just anterior to this fibrous band. For mild contractures of less than 20 degrees, nonsurgical management is usually adequate. Hamstring lengthening and postoperative splinting are usually sufficient for contractures of 20 degrees to 40 degrees. Moderate contractures of up to 60 degrees usually require Z-plasties in the popliteal fossa and postoperative serial casting to avoid undue tension on neurovascular structures. Contractures of more than 60 degrees require a femoral shortening osteotomy or gradual correction with an external fixator. However, rapid recurrence following fixator removal is common if formal soft-tissue procedures and postoperative splinting are not performed. Parikh SN, Crawford AH, Do TT, et al: Popliteal pterygium syndrome: Implications for orthopaedic management. J Pediatr Orthop B 2004;13:197-201.
Question 59
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management?


Explanation
Congenital scoliosis in an infant warrants evaluation of the renal, cardiac, and neurologic systems because frequently there is concurrent pathology. Progression in this instance is possible but not certain; therefore, progression must be documented prior to any surgical intervention. Close observation with serial radiographs every 4 to 6 months is appropriate. All of the surgical options listed may be reasonable choices in the future, but cardiac evaluation is the most important issue at this time. Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity: A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
Question 60
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Explanation
In adolescents, a lumbar herniated disk is characterized by a paucity of clinical findings; a positive straight leg raising test may be the only consistent positive finding. This may result in a long period of nonsurgical management that fails to provide relief. Activities that place a significant shear load on the lumbar spine, such as the dead lift, are associated with an increased risk of central disk herniation. When an adolescent who lifts weights has a history of low back pain that fails to respond to a short period of active rest, an MRI scan is the study of choice to evaluate for a lumbar herniated disk. Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Question 61
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
A muscle that lengthens as it is activated is an eccentric contraction. Isometric contraction involves no change in length. Concentric contraction occurs while the muscle is shortening. In isotonic contraction, the force remains constant through the contraction range. Isokinetic muscle contraction occurs at a constant rate of angular change of the involved joint. Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 12-13.
Question 62
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
The patient has an acute peroneal tendon dislocation. The evaluation for syndesmotic injury and lateral ankle instability is negative. The cortical avulsion off the distal tip of the lateral malleolus, a rim fracture, is characteristic of peroneal tendon dislocations. The sensation of apprehension or frank subluxation of the peroneal tendons with active dorsiflexion of the foot while the foot is held in plantar flexion confirms the diagnosis. Based on these findings, initial management should consist of cast immobilization and protected weight bearing. If a recurrent or chronic condition develops, surgery is the most reliable treatment option. Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Question 63
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
The medial collateral ligament complex of the elbow consists of three portions: the anterior bundle, the posterior bundle, and a transverse component that has little biomechanic significance. The origin of the ligament is from the central two thirds of the anteroinferior undersurface of the medial epicondyle.
Question 64
A 31-year-old man sustained a closed injury to his arm in a motor vehicle accident 16 months ago. Treatment of the fracture consisted of intramedullary nailing of the humerus. He now reports pain with minimal activities. Clinical examination and laboratory studies suggest no signs of infection. Radiographs are seen in Figures 12a through 12c. Treatment should now consist of



Explanation
The use of locked nailing for the treatment of established nonunion of the humerus has produced poor results. Since humeral nailing has already failed, exchange humeral nailing without bone grafting has an even less change of success. To increase the likelihood of achieving bony union, the treatment of choice is removal of the humeral nail, dynamic compression plating, and bone grafting. Zuckerman J, Giordanno C, Rosen H: Treatment of humeral shaft non-unions, in Bigliani L (ed): Complications of shoulder surgery. Baltimore, MD, William & Wilkins, 1993, pp 173-190.
Question 65
Medial dislocation of the long head of the biceps tendon in the shoulder is most commonly caused by a
Explanation
Medial dislocation of the biceps tendon in the shoulder is commonly associated with subscapularis tendon tears. Although type II SLAP tears can result in bicipital instability, type I SLAP lesions do not. Congenitally shallow grooves and tears of the transverse ligaments usually do not lead to dislocation of the biceps tendon. Supraspinatus tendon tears are associated with long head of the biceps tendon ruptures but do not cause biceps tendon dislocations. Werner A, Mueller T, Boehm D, et al: The stabilizing sling for the long head of the biceps tendon in the rotator cuff interval: A histoanatomic study. Am J Sports Med 2000;28:28-31.
Question 66
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical managment has failed to provide relief. What is the treatment of choice?

Explanation
The radiograph reveals the classic "bump" that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement. Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Question 67
Collagen orientation is parallel to the joint surface in what articular cartilage zone?
Explanation
The collagen orientation changes from parallel in the superficial zone to a more random pattern in the middle zone and finally to perpendicular in the calcified zone. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 498-499.
Question 68
The fracture shown in Figure 50 is most reliably treated with what form of fixation?

Explanation
The radiograph shows a comminuted proximal ulnar fracture. The most reliable fixation is a posterior plate, acting as a tension band plate. The fracture involves the proximal shaft of the ulna; therefore, a 3.5-mm compression plate or one of similar size should be used to provide adequate stability. Kirschner wires and tension band wires do not provide axial stability of the comminution of the ulna. Compression screws alone will most likely fail and will not provide axial rotational stability to the construct. A medial plate will not resist the distraction forces across this fracture. McKee MD, Seiler JG, Jupiter JB: The application of the limited contact dynamic compression plate in the upper extremity: An analysis of 114 consecutive cases. Injury 1995;26:661-666.
Question 69
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals

Explanation
The MRI scan reveals a full-thickness rotator cuff tear with retraction and increased signal in the subacromial space indicating joint fluid. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Question 70
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively?

Explanation
The effects of cigarette smoking and smoking cessation on spinal fusion have been studied extensively. Although permanent smoking cessation is ideal, significant improvements in fusion rates are seen in patients who avoid smoking for greater than 6 months postoperatively.
Question 71
A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of


Explanation
The patient has an isolated closed injury involving the humeral diaphysis. The lack of wrist and finger extension indicates injury to the radial nerve. Based on these findings, ongoing observation of the nerve is warranted with delayed exploration after 3 to 4 months if there are no signs of progressive return of nerve function. Treatment of the fracture should include external immobilization and fracture bracing. An indication for nerve exploration and surgical stabilization would be an open fracture. Zuckerman JD, Kovil KJ: Fractures of the shaft of the humerus, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1025-1053.
Question 72
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of




Explanation
Tarsal coalitions commonly present in the preadolescent age group as a rigid, planovalgus foot. Small coalitions of the calcaneonavicular joint or the middle facet of the talocalcaneal joint can be excised with interposition of fat or muscle tissue. Isolated calcaneocuboid joint coalitions are very rare. This patient has an associated large talocalcaneal coalition; therefore, resection is contraindicated. Surgery is warranted after failure of nonsurgical management, and because of the involvement of two joints, the only viable option for the severely symptomatic foot is triple arthrodesis. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 73
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?



Explanation
The MRI scans clearly show an extruded L4-5 disk that is affecting the L5 nerve root on the left side. In addition, the L5 nerve root has a cutaneous distribution in the first dorsal web space. S1 affects the lateral foot. L4 affects the medial calf.
Question 74
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
Explanation
The history and presentation are consistent with type I Charcot-Marie-Tooth (CMT), the most common form of hereditary peripheral motor sensory neuropathy. Type I CMT is the most common, occurring in 50% of patients with CMT, and is characterized by marked slowing of motor neuron velocities, and inconsistent slowing of sensory neuron velocities. Peroneus longus to brevis transfer is indicated to release the overpull of the peroneus longus, and restore the eversion and dorsiflexion function of the peroneus brevis. A lateralizing calcaneal osteotomy with proximal translation is indicated to correct heel varus given that the Coleman block only allows for partial correction of heel varus. Proximal translation of the posterior tuber corrects for the increased calcaneal dorsiflexion, improving the lever arm for the triceps surae. A medial column closing wedge osteotomy is often required to correct a rigid, or semirigid plantar flexed first ray to allow for a balanced, plantigrade foot. Triple arthrodesis is indicated for rigid, arthritic hindfoot deformities. Transfer of the posterior tibial tendon to the tibialis anterior is not indicated since it is an out-of-phase transfer. Transfer of the posterior tibial tendon, when performed, should be to the lateral aspect of the foot. A medializing calcaneal osteotomy would accentuate the heel varus. There is no indication for Botox in CMT; Botox injection of the calf would further weaken push-off during gait. Bracing of a progressive semirigid or rigid deformity is not recommended. Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315. Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.
Question 75
A 15-year-old female field hockey player sustains a blow to the mouth from a hockey stick. Three front teeth are knocked out and shown in Figure 4. In addition to calling a dentist immediately, what is the next best step in management?

Explanation
Tooth avulsions can occur in contact or collision sports. An avulsed tooth is a medical emergency. The likelihood of survival of the tooth depends on the length of time that the tooth is out of the socket and the degree to which the periodontal ligament is damaged. The tooth should be handled only by the crown end and not the root end. It can be rinsed of debris with water or normal saline solution. The tooth should not be brushed or cleaned otherwise. During transport, the tooth must be kept moist. An avulsed tooth can be transported in whole milk, saliva, sterile saline solution, or commercially available kits with physiologic buffer solutions. The tooth and the athlete should be transported to the dentist for reinsertion as soon as possible and preferably within an hour. Krasner P: Management of sports-related tooth displacements and avulsions. Dent Clin North Am 2000;44:111-135. Sullivan JA, Anderson SJ (eds): Care of the Young Athlete. Rosemont IL, American Academy of Orthopaedic Surgeons, Elk Grove Village, IL, American Academy of Pediatrics, 2000, p 190.
Question 76
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 77
Figures 13a and 13b show the preoperative radiographs of a 60-year-old woman who is scheduled to undergo total knee arthroplasty under epidural anesthesia. Postoperatively she reports a burning sensation on the dorsum of her foot despite the administration of IV analgesics through a patient-controlled analgesia (PCA) pump. Management should now include


Explanation
The patient has a significant flexion contracture and valgus deformity; therefore, the risk of peroneal nerve injury is increased. Idusuyi and Morrey noted that epidural anesthesia also increases the risk of peroneal nerve injury. The initial symptom can be a burning sensation on the foot, followed by pain and then motor weakness. Initial management should consist of release of the dressings and knee flexion. Idusuyi OB, Morrey BF: Peroneal nerve palsy after total knee arthroplasty: Assessment of predisposing and prognostic factors. J Bone Joint Surg Am 1996;78:177-184.
Question 78
An 11-year-old boy has had a fever and pain and swelling over the lateral aspect of his right ankle for the past 3 days. Examination reveals warmth, swelling, and tenderness over the lateral malleolus, and he has a temperature of 103.2 degrees F (39.5 degrees C). Laboratory studies show a WBC count of 13,200/mm3 with 61% neutrophils, an erythocyte sedimentation rate of 112 mm/h, and a C-reactive protein of 15.7. Radiographs and a T2-weighted MRI scan are shown in Figures 13a through 13c. Aspiration yields 1 mL of purulent fluid. Management should now consist of



Explanation
The initial signs and symptoms of acute hematogenous osteomyelitis vary widely but usually include fever, bone pain, and impaired use of the involved extremity. In lower extremity infections, the child may limp or refuse to walk. Examination often reveals bone tenderness. In more advanced cases, erythema, warmth, and swelling may be present. The WBC and neutrophil counts are not always elevated, but the erythocyte sedimentation rate will be abnormal in more than 90% of patients. When the infection is diagnosed early, before a subperiosteal abscess has formed, antibiotics alone may be adequate to treat the infection. This patient has a more advanced infection, however, with the MRI scan revealing a subperiosteal abscess that was confirmed by aspiration. When an abscess is present, surgical drainage is generally indicated to remove devitalized tissue and to enhance the efficacy of the antibiotics. Further studies, such as bone or indium scans, are not necessary and will delay definitive treatment. Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: A review of 116 cases. J Pediatr Orthop 1990;10:649-652.
Question 79
A superior labrum anterior and posterior (SLAP) lesion doubles the strain in which of the following stabilizing structures?
Explanation
A superior labrum, when intact, stabilizes the shoulder by increasing its ability to withstand excessive external rotational forces by an additional 32%. The presence of a SLAP lesion decreases this restraint and increases the strain in the superior band of the inferior glenohumeral ligament by over 100%. Rodosky MW, Harner CD, Fu FH: The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med 1994;22:121-130.
Question 80
A 25-year-old competitive skier sustains a twisting injury to the right ankle while skiing. She is unable to continue the activity secondary to severe lateral ankle pain. Examination reveals ecchymosis and fullness over the lateral malleolus with pain and weakness on active ankle dorsiflexion and external rotation. There is no medial-sided pain. Neurovascular examination is normal. An AP radiograph and MRI scan are shown in Figures 17a and 17b, respectively. Management should consist of


Explanation
The MRI scan shows a dislocated peroneus brevis tendon with disruption of the peroneal retinaculum. This injury is commonly seen in skiers and is the result of peroneal contraction with the ankle everted and dorsiflexed. Nonsurgical management is rarely successful; therefore, repair of the peroneal retinaculum is the treatment of choice. Eckert WR, Davis EA Jr: Acute rupture of the peroneal retinaculum. J Bone Joint Surg Am 1976;58:670-672. Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Question 81
Figures 4a and 4b show the radiographs of a 32-year-old man who has right groin pain with activity or prolonged standing. Which of the following factors would not prohibit consideration of acetabular liner exchange and grafting of the defects?


Explanation
Polyethylene particles generated as mechanical wear debris can be phagocytized by macrophages and enter a metabolically active state that releases cytokines, causing periprosthetic bone resorption. Significant osteolysis can occur in the pelvis with a porous-coated cementless socket without loosening of the component. If the acetabular component is modular, well positioned, well-designed with a good survivorship record, and remains undamaged after liner removal, the polyethylene liner can be exchanged and the lytic defects can be debrided and bone grafted. This implant is well positioned, has a good survivorship record, a good locking mechanism, and is modular. The hip arthroplasty needs to be aseptic for consideration of liner exchange. Maloney WJ, Herzwurm P, Paprosky W, Rubash HE, Engh CA: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Question 82
A 64-year-old man with a history of metastatic lung cancer reports increasing right hip pain over the period of several months. Radiographs are shown in Figures 3a and 3b. Initial management should consist of


Explanation
The patient has lung cancer metastatic to the right proximal femur. The lesion is large, has destroyed a portion of the cortex, and involves the peritrochanteric region. All of these findings put the patient at high risk for pathologic fracture. The lesion is amenable to intramedullary fixation in the form of some type of reconstruction nail. Chemotherapy alone will not restore the bone stock. Given the extent of the lesion, radiation therapy, chemotherapy, or embolization will not prevent fracture. A proximal femoral replacement would be indicated in patients with bone destruction extending into the femoral head and neck. Bisphosphonates may diminish the risk of subsequent lesions but are not sufficient to treat this high-risk lesion. Radiation therapy should be given postoperatively to prevent further bone destruction.
Question 83
Which of the following is considered the best method to measure limb-length discrepancy in a patient with a knee flexion contracture?

Explanation
The most effective way to measure a limb-length discrepancy in a patient with a knee flexion contracture is a lateral CT scanogram. All the other methods listed provide inaccurate results with a knee flexion contracture because the measurements are made in the coronal plane. Aaron A, Weinstein D, Thickman D, et al: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Question 84
A 26-year-old man sustained an isolated injury to his left hip joint in a motor vehicle accident. Closed reduction was performed, and the postreduction radiograph is shown in Figure 29. Management should now consist of

Explanation
The patient has a posterior fracture-dislocation of the hip and following reduction, an incarcerated fragment of bone resulted in an incongruent reduction. Whereas expedient removal of the fragment is required to limit articular cartilage damage, this situation is not an emergency and the procedure may be performed when the appropriate surgical team is available and the patient is stabilized. Skeletal traction through either the femur or tibia may relieve some pressure on the joint and prevent articular damage. Nonsurgical care for incarcerated fragments is contraindicated. Tile M, Olson SA: Decision making: Non operative and operative indications for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 496-532.
Question 85
Plots of stress versus strain for four orthopaedic biomaterials are shown in Figure 3. Referring to the figure, what is the correct identification of the curves?

Explanation
Stress-strain plots allow easy comparison of a number of important mechanical properties, including elastic modulus (the slope of the initial straight line portion of the curve) and yield stress (the stress at the break in the curves for bone, steel, and titanium alloy). Important considerations here are much lower modulus and ultimate stress of bone and cement compared to the two metallic alloys, the fact that titanium is lower modulus but higher strength than stainless steel, and the identification of cement as the only brittle material among the four. Burstein AH, Wright TM: Fundamentals of Orthopaedic Biomechanics. Baltimore, MD, Williams and Wilkins, 1994, pp 97-129.
Question 86
Which of the following methods of meniscal repair has the highest load to failure strength?
Explanation
Numerous experimental studies have shown that vertical suture techniques are superior to all of the other noted methods. In fact, vertical sutures have been shown to be twice as strong as several of these techniques. DeHaven KE: Meniscus repair. Am J Sports Med 1999;27:242-250. Dervin GF, Downing KJ, Keene GC, McBride DG: Failure strengths of suture versus biodegradable arrow for meniscal repair: An in vitro study. Arthroscopy 1997;13:296-300.
Question 87
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 88
A 15-year-old boy has had pain in the right shoulder for the past 3 months. He denies any history of trauma and has no constitutional symptoms. Examination reveals a large firm mass in the proximal arm. A radiograph and MRI scan are shown in Figures 27a and 27b. Biopsy specimens are shown in Figures 27c and 27d. Management should consist of




Explanation
The patient has an aneurysmal bone cyst. The fluid-fluid levels seen on the MRI scan are typical for aneurysmal bone cyst, and the histology is consistent with a cystic lining. Vascular lakes, multinucleated giant cells, reactive bone, fibrovascular tissue, and an absence of atypical cells or numerous mitoses are seen histologically. Aneurysmal bone cysts will typically continue to grow and cause further bone destruction; therefore, observation is not recommended. Steroid injections are not effective. A thorough curettage of the cyst lining and bone grafting are required. Wide resection and chemotherapy are reserved for more aggressive tumors. There is no evidence of infection radiographically or histologically. Telangiectatic osteosarcoma should also be considered in the differential diagnosis; therefore, biopsy is an important part of the work-up. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 232-233.
Question 89
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.
Question 90
A 35-year-old patient has right hip pain. Figures 34a and 34b show the coronal MRI scan and the biopsy specimen. What is the most likely diagnosis?


Explanation
Alcohol abuse, steroids, Caisson disease, sickle cell disease, and radiation therapy are the leading causes of nontraumatic osteonecrosis of the femoral head. Arlet J: Nontraumatic avascular necrosis of the femoral head: Past, present, and future. Clin Orthop 1992;277:12-21.
Question 91
A 75-year-old woman undergoes hybrid total hip arthroplasty for osteoarthritis. A postoperative radiograph obtained in the recovery room is shown in Figure 18. Treatment should now consist of

Explanation
Intraoperative femoral fractures can often be avoided by careful preoperative planning to optimize implant design and size. Most fractures occur during implantation of a cementless implant; many can be avoided by careful femoral preparation and component implantation, with particular caution in osteopenic bone. Intraoperative femoral fractures are managed according to fracture severity. Minor cracks that do not affect stability or femoral integrity can often be managed intraoperatively with cerclage fixation, limited weight bearing, and observation. Femoral fractures that compromise implant stability or femoral integrity require fracture fixation with cerclage wires, strut grafts, or plates and may require conversion to a long stem implant. This patient's fracture is nondisplaced and the implant is well seated; therefore, limited weight bearing is considered appropriate management. Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118. Kelley SS: Periprosthetic femoral fractures. J Am Acad Orthop Surg 1994;2:164-172.
Question 92
When 6 weeks of noninvasive nonsurgical management fails to provide relief for a lumbar disk herniation, a trial of epidural steroid injections is likely to yield which of the following results?

Explanation
Lumbar epidural steroid injections appear to play a role in management of a lumbar disk herniation that has failed to respond to at least 6 weeks of nonsurgical treatment. Approximately 42% to 56% of patients report significant pain relief compared with 92% to 98% of those patients treated with diskectomy. Patients with extruded or sequestered herniations report the greatest and most rapid relief. Similarly, those with well-hydrated disk fragments report rapid relief of symptoms. A smaller percentage of patients report symptom relief compared with those having surgery, but the degree of improvement is similar for both groups and the improvement lasts up to 3 years. Butterman GR: Treatment of lumbar disc herniation: Epidural steroid injection compares with discectomy: A prospective, randomized study. J Bone Joint Surg Am 2004;86:670-679.
Question 93
Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?

Explanation
The incidence of femoral fracture in primary cementless total hip arthroplasty ranges from 1.5% to 27.8%. It is imperative that the implant and fracture are stable both intraoperatively and postoperatively. Cerclage wiring or cerclage cabling is the current recommended treatment for nondisplaced calcar fractures and minimally displaced proximal fractures. Berend and associates reviewed the results of 58 total hips in 55 patients with intraoperative calcar fracture managed with single or multiple cerclage wires or cables and immediate full weight bearing. Follow-up averaged 7.5 years, and there were no revisions of the femoral component. No patients had severe thigh pain. Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21. Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.
Question 94
A 65-year-old man has a painful right hip mass that has been growing for several years. A radiograph, CT scan, and photomicrograph are shown in Figures 56a through 56c. What is the most appropriate treatment?



Explanation
This is a conventional chondrosarcoma. The radiograph and the CT scan show a lesion arising from the inferior pubic ramus with a large soft-tissue mass. Abundant punctate, stippled, or "popcorn-like" calcification is present. The photomicrograph demonstrates hypercellular cartilage. Surgical resection is the only effective treatment. Whereas chemotherapy might play a role in the treatment of a dedifferentiated chondrosarcoma, it has no role in the treatment of a conventional chondrosarcoma. Chondrosarcomas are relatively radioresistant. Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Question 95
A 50-year-old woman has a painful hallux valgus and a painful callus beneath the second metatarsal head. A radiograph is shown in Figure 46. To correct these problems, treatment of the great toe deformity should consist of

Explanation
The patient has a significant hallux valgus and instability of the first ray, causing transfer metatarsalgia to the second metatarsal head. Therefore, the best procedure is fusion of the metatarsal cuneiform joint with soft-tissue realignment of the first metatarsophalangeal joint. This procedure provides the best chance of relieving symptoms under the second metatarsal head, as well as correcting the hallux valgus.
Question 96
Figure 53 shows the pedigree of a family with an unusual type of muscular dystrophy. This pedigree is most consistent with what type of inheritance pattern?

Explanation
The pedigree documents involvement of male offspring only, and it also shows transmission through an uninvolved female carrier. This inheritance pattern is most consistent with a x-linked recessive inheritance. It would be inconsistent with a dominant inheritance pattern unless there was incomplete penetrance. Autosomal-recessive inheritance would be possible only if the family member labeled II.F was also a carrier of the same gene; however, this is unlikely. Mitochondrial inheritance is possible, but as with autosomal patterns, mitochondrial inheritance normally affects both male and female offspring. It is transmitted only through the maternal line.
Question 97
High Yield
What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?
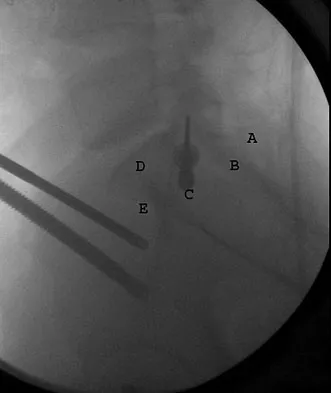
Explanation
Iliosacral screws cannot always be placed safely due to variations in pelvic anatomy. Transiliac bars are an alternative method for fixation but are placed using an open technique. A screw can be placed percutaneously through both iliac wings posterior to the posterior border of the sacrum. The starting point is visualized using a lateral C arm shot and is located on the posterior iliac crest at about the level of the S1 body where the crest has its largest area posterior to the sacrum. This area is labeled A in the figure, B represents the sacral canal, C is S1, D is the area cephalad to the iliocortical density, and E is the anterior border of the sacrum. The radiograph demonstrates a well-placed sacroiliac screw. Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: Cadaver feasibility study and preliminary clinical results. J Trauma 2007;62:357-364.
Question 98
Which of the following findings is seen in the chest radiograph shown in Figure 13?

Explanation
Orthopaedic surgeons are often responsible for interpreting radiographs of general examinations such as the chest radiograph shown. For accurate interpretation, it is important to systematically review all of the information available on the radiograph. Using this approach, the fracture of the left proximal humerus is readily recognized. Linear air soft-tissue density at the lung periphery would suggest a pneumothorax, but this finding is not shown on the radiograph. The upper thoracic spine is well aligned. The sternoclavicular and distal clavicles are normal.
Question 99
An 11-year-old child has Ewing's sarcoma of the femoral diaphysis with a small soft-tissue mass. Staging studies show no evidence of metastases. Treatment should consist of
Explanation
The use of chemotherapy has dramatically improved survival rates of patients with Ewing's sarcoma. Local disease is best handled with wide resection to decrease local recurrence and to avoid the complications of radiation therapy (ie, secondary sarcomas). Radiation therapy alone is reserved for unresectable lesions or poor surgical margins. Amputation generally is not necessary. Toni A, Neff JR, Sudanese A, et al: The role of surgical therapy in patients with non-metastatic Ewing's sarcoma of the limbs. Clin Orthop 1991;286:225. Picci P, Rougraff BT, Bacci G, et al: Prognostic significance of histopathologic response to chemotherapy in non-metastatic Ewing's sarcoma of the extremities. J Clin Oncol 1993;11:1763.
Question 100
Spontaneous entrapment of the posterior interosseous nerve most commonly occurs in which of the following locations?
Explanation
The extensor carpi radialis brevis, supinator muscle, arcade of Frohse, and leash of Henry are potential sites of compression for the posterior interosseous nerve. The most common location of spontaneous entrapment is the arcade of Frohse. The lateral intermuscular septum is a site of compression for the radial nerve.
