Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The arrow in the axial T1-weighted MRI scan shown in Figure 18 is pointing to which of the following structures?

Explanation
The arrow is pointing to the ulnar nerve within Guyon's canal. Guyon's canal is approximately 4 cm long, beginning at the proximal extent of the transverse carpal ligament and ending at the aponeurotic arch of the hypothenar muscles. Many structures comprise the boundaries of Guyon's canal. The floor, for example, consists of the transverse carpal ligament, the pisohamate and pisometacarpal ligaments, and the opponens digiti minimi. Within Guyon's canal, the ulnar nerve bifurcates into the superficial and deep branches, with the deep branch of the ulnar nerve persisting distal to the canal. The ulnar artery is immediately adjacent and radial to the ulnar nerve. The median nerve is visualized within the carpal tunnel. The radial artery is on the radial side of the wrist. The hook of the hamate is clearly seen in the figure, orienting the observer to the ulnar side of the wrist. Goss MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 1985;196:238-247.
Question 2
Figure 49 shows the radiograph of a 3-year-old child with progressive bowlegs. Laboratory studies show a calcium level of 9.5 mg/dL (normal 9.0 to 11.0 mg/dL), a phosphorus level of 4.2 mg/dL (normal 3 to 5.7 mg/dL), and an alkaline phosphatase level of 305 IU/L (normal 104 to 345 IU/L). What is the most likely diagnosis?

Explanation
The patient has bowlegs associated with very wide physes, particularly noted at the hips. The widening of the growth plates is a classic sign of rickets; however, the normal levels of calcium, phosphorus, and alkaline phosphatase rule out both nutritional and hypophosphatemic rickets. Patients with nutritional rickets or hypophosphatemic rickets have hypophosphatemia and increased alkaline phosphatase levels. Jansen metaphyseal dysostosis has very severe radiographic findings that are not found in this patient; however, these radiographic findings are classic for Schmid metaphyseal dysostosis. This disorder is caused by a mutation in the gene for type X collagen, which is found only in the growth plates of growing children. Lachman RS, Rimoin DL, Spranger J: Metaphyseal chondrodysplasia - Schmid type: Clinical and radiographic delineation with a review of the literature. Pediatr Radiol 1988;18:93-102.
Question 3
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?

Explanation
Persistent pain following an ankle sprain can present a diagnostic dilemma. All of the injuries listed should be considered in the differential diagnosis. The superficial peroneal nerve courses in the lateral compartment and exits the crural fascia 12 to 15 cm above the level of the ankle. Muscle herniation through the fascial defect has been reported to be associated with entrapment of this nerve. The fascial hiatus also may serve as a potential tether in cases of inversion injuries causing injury to the superficial peroneal nerve. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 4
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4 degrees F (37.4 degrees C), and examination reveals that abduction of the left hip is limited to 30 degrees. Laboratory studies show a WBC of 11,000/mm3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of

Explanation
The most likely diagnosis is transient synovitis. Initial management should consist of bed rest and serial observation to rule out atypical septic arthritis of the hip. In an unreliable family situation, hospitalization for bed rest and observation may be indicated. Other disorders such as proximal femoral osteomyelitis, leukemia, juvenile rheumatoid arthritis, pelvic osteomyelitis, diskitis, and arthralgia secondary to other inflammatory disorders should be considered. However, these disorders are unlikely because of the paucity of abnormal clinical signs exhibited by the patient. On the other hand, transient synovitis of the hip in children is a diagnosis of exclusion; other possibilities should be explored if the patient's symptoms do not follow a typical course and resolve in 4 to 21 days.
Question 5
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
The majority of large collagen fibers within the menisci are oriented circumferentially. It is these fibers that develop the hoop stress with compressive loading of the menisci. Most meniscal tears are longitudinal and occur between these circumferential fibers. Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
Question 6
Figures 23a and 23b show the radiograph and clinical photograph of a patient who reports a reduced ability to flex the interphalangeal joint of her great toe after undergoing a Chevron-Akin bunionectomy. What is the most likely cause?


Explanation
The flexor hallucis longus tendon is at risk during a Chevron-Akin osteotomy because of its close relationship to the base of the proximal phalanx. The radiograph reveals a reduced ability to flex the interphalangeal joint secondary to the flexor hallucis longus laceration. The other complications are not supported by the radiograph. Tollison ME, Baxter DE: Combination chevron plus Akin osteotomy for hallux valgus: Should age be a limiting factor? Foot Ankle Int 1997;18:477-481.
Question 7
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
In the normal adult, the distance between the basion and the tip of the dens is 4 mm to 5 mm. Any distance greater than 5 mm is considered abnormal. This is one way to detect occipitocervical dissociation other than using the Power's ratio, which relies on an anterior dislocation. Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Question 8
Which of the following statements is most accurate regarding undetected intraoperative surgical glove perforation?
Explanation
The incidence of undetected intraoperative surgical glove perforation has been demonstrated at approximately 8.5%, occurring most frequently on the index finger or left hand of the assistant surgeon. The frequency of glove perforation is higher in surgeries lasting longer than 3 hours. Al-Habdan I, Sadat-Ali M: Glove perforation in pediatric orthopaedic practice. J Pediatr Orthop 2003;23:791-793.
Question 9
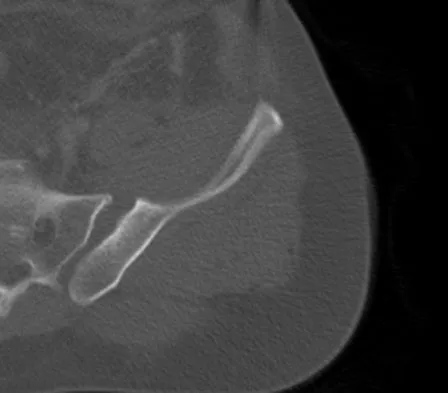
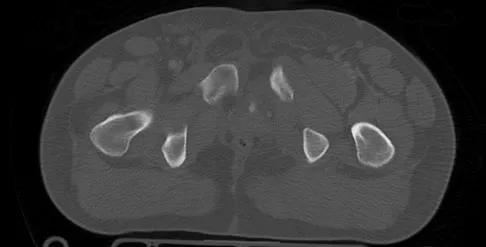
An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?



Explanation
The sagittal and axial CT scans show a bilateral spondylolysis at L5. The defect is in the pars interarticularis on the right side but at the base of the pedicle on the left. Having failed a trial of physical therapy with only a 3-month history of pain, the next most appropriate step in management should consist of activity modification and bracing in an antilordotic lumbosacral orthosis. Surgical intervention is reserved for patients who have failed to respond to a trial of bracing and activity restriction. Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.
Question 10
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?

Explanation
Several studies have shown that sitting ability by age 2 years is highly prognostic of walking. Molnar and Gordon reported that children not sitting independently by age 2 years had a poor prognosis for walking. Wu and associates reported that children sitting without support by age 2 years had an odds ratio of 26:1 of walking compared with those unable to sit. This was far higher than the odds ratios for cerebral palsy location, motor dysfunction, crawling, creeping, scooting, or rolling. Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Question 11
A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient's ability to heal the wound postoperatively?
Explanation
Absolute toe pressures greater than 40 to 50 mm Hg are a good sign of healing potential. An ABI of greater than 0.45 favors healing, but indices greater than 1 are falsely positive due to calcifications in the vessels. Normal albumin is an overall indication of nutritional status. A transcutaneous oxygen level should be greater than 40 mm Hg for healing. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.
Question 12
The lateral arm flap is based on what arterial supply?
Explanation
The lateral arm flap is based on the posterior radial collateral artery, a branch of the profunda brachial artery. Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
Question 13
Which of the following best describes athletic pubalgia?
Explanation
Athletic pubalgia refers to a distinct syndrome of lower abdominal and adductor pain that is mostly commonly seen in high performance male athletes. This condition must be distinguished from others such as painful inflammation of the symphysis pubis, referred to as osteitis pubis. Symptoms attributable to the iliopsoas tendon are most commonly associated with snapping of the tendon. Stress fracture of the pubic ramus may cause symptoms in this area, but it is usually confirmed by imaging studies. Neurapraxia of the pudendal nerve is associated with pressure from the seat in cycling sports and also as a complication associated with traction during surgical procedures. Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Question 14
An 11-year-old boy sustained an injury to his arm in gym class. He denies prior pain in the arm. Radiographs are shown in Figures 48a and 48b. What is the next most appropriate step in the management of this lesion?


Explanation
This radiolucent lesion with a "fallen leaf sign" is typical for a unicameral bone cyst(UBC). The most appropriate treatment is to allow the fracture to heal with clinical and radiographic observation. Curettage and bone grafting is not the best initial management for UBC. Wide resection is not indicated for UBC. The proximal humerus is the most common site for UBC. While staging studies consisting of MRI, bone scan, and CT of the chest are appropriate for lesions suspected of being malignant, the classical appearance of this UBC is such that this work-up is not necessary initially. Following fracture healing, aspiration and injection of the cyst may be indicated. Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Question 15
A 10-month-old girl has the spinal deformity shown in Figures 55a and 55b with no apparent neurologic finding. The next step in evaluation should be to obtain


Explanation
Approximately 60% of patients with a congenital spine abnormality have associated malformations outside the spinal column. Genitourinary abnormalities are probably the most common, occurring in up to 37% of patients. These are usually anatomic anomalies, such as renal agenesis, duplication, fusion, and ectopia. A genitourinary ultrasound is the least invasive screening tool. Other associated anomalies include cervical vertebral abnormalities, VATER syndrome, and intraspinal abnormalities such as diastematomyelia. An MRI scan is not recommended as part of the screening examination; however, if the patient had neurologic signs or symptoms, an MRI scan would be indicated. Beals RK, Robbins JR, Rolfe B: Anomalies associated with vertebral malformations. Spine 1993;18:1329-1332.
Question 16
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?


Explanation
Microfracture is a marrow stimulation technique where stem cells from the underlying subchondral bone marrow can form at the base of the lesion. The rationale for this technique is based on these cells differentiating into cells that will produce an articular cartilage repair. Biopsy findings in animals and humans have demonstrated primarily a fibrocartilagenous repair tissue and not articular cartilage. The collagen type found in hyaline or articular cartilage is of the type II variety. Fibrocartilage possesses mostly type I and III cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
Question 17
What is the most prevalent adverse event associated with allogeneic blood transfusion?

Explanation
Clerical error leading to acute hemolysis and even death occurs in 1:12,000 to 1:50,000 transfusions. Bacterial contamination leading to sepsis/shock occurs in 1:1 million transfusions. HIV transmission is approximately 1:500,000 transfusions and hepatitis C is 1:103,000 transfusions. Anaphylactic reactions occur in 1:150,000 transfusions. Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Question 18
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of

Explanation
Serratus anterior palsy or long thoracic nerve palsy is usually caused by traction injury to the nerve, blunt injury, or iatrogenic injury. The palsy results in winging of the scapula and medial rotation of the inferior pole of the scapula. A patient with this injury will usually recover in 12 to 18 months. Initial treatment should include observation and shoulder strengthening exercises. Nerve exploration with repair has not proven beneficial in changing the outcome. Many orthopaedic surgeons favor using a split pectoralis major transfer for symptomatic patients. Electrodiagnostic studies are helpful in confirming the diagnosis. Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
Question 19
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
Injury to the sciatic nerve is a relatively rare but serious complication of THA. Dissection of the sciatic nerve is not typically done during primary THA, although the nerve can be identified during the surgical approach. An anterolateral approach to THA would not necessarily be associated with any greater incidence of sciatic nerve injury than other approaches. Screw fixation for the acetabular component is often a matter of surgeon preference. Provided that the anatomic safe zones for screw fixation (posterior inferior and posterior superior) are recognized, injury to the sciatic nerve from acetabular screws can be minimized. Restoration of anatomic length is important in primary THA. Overlengthening can result in sciatic nerve palsy. Developmental dysplasia of the hip can lead to a congenitally shortened extremity with concomitant congenital shortening of the associated neurovascular structures. Overlengthening of the extremity during THA for developmental dysplasia of the hip can lead to sciatic palsy. Osteonecrosis is not an associated risk factor for sciatic nerve palsy. DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
Question 20
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of

Explanation
The clinical photographs show a patient with a type I hereditary sensory motor neuropathy who has cavus feet with a flexible hindfoot. The Coleman block test shows that the hindfoot corrects into valgus. To prevent progressive cavus, patients with this condition may benefit from soft-tissue releases at a younger age while the foot is flexible. Once there is fixed deformity, combined soft-tissue and bone procedures usually are necessary. Metatarsal osteotomies will correct the cavus, but will do nothing for the drop foot. Transfer of the extensor hallucis longus to the neck of the first metatarsal and modified transfer of the extensor digitorum longus to the dorsum of the foot will prevent further claw toes and improve foot dorsiflexion. Anterior transfer of the posterior tibialis tendon will also aid in dorsiflexion. Calcaneal osteotomy should be reserved for fixed hindfoot varus that does not correct with block testing, and triple arthrodesis should be avoided as long as possible because the long-term outcome is poor. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245. Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Question 21
A 67-year-old patient seen in the emergency department reports the acute onset of pain and is unable to ambulate. History reveals that the patient underwent surgical treatment for a periprosthetic femoral fracture 6 months ago. A radiograph is shown in Figure 41. What is the best treatment option at this time?

Explanation
The radiograph reveals a periprosthetic fracture at the tip of the stem with a stable cemented implant. This is classified as a Vancouver type B1 periprosthetic fracture. An attempt at internal fixation has already failed; therefore, the most predictable results would be achieved with distal fixation. After removal of the well-fixed cemented implant, the proximal bone may not be suitable for proximal fixation. Adequate bone stock is available such that an allograft prosthetic composite or a tumor prosthesis is not necessary. The best option is a long stem implant with distal fixation, which serves as an intramedullary device to restore alignment and increase the likelihood of union. Cortical onlay strut grafts are used as an adjunct to definitive fixation. Younger AS, Dunwoody I, Duncan CP: Periprosthetic hip and knee fractures: The scope of the problem. Inst Course Lect 1998;47:251-256.
Question 22
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
Breech positioning has been noted as the risk factor that most increases the relative risk of developmental dysplasia of the hip in multiple series and meta-analysis. All the other factors also increase the risk but to a lesser magnitude. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 23
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?


Explanation
The radiographs show early ectopic bone formation originating between the ulna and the radius. The development of ectopic bone in this area following a two-incision approach for anatomic repair of the distal biceps tendon is thought to be related to exposure of the periosteum of the lateral ulna during surgery. This can be avoided by the use of a muscle-splitting incision between the extensor carpi ulnaris and common extensor muscles. Full pronation of the forearm allows for the necessary exposure of the radial tuberosity during the procedure and for fixation of the tendon at its maximal length. Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Question 24
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed

Explanation
Very large corrections of tibial deformity can be achieved at or just below the tibial tubercle. This level of osteotomy maintains the relationship between the tubercle and the rest of the joint, does not alter patellofemoral mechanics, and avoids complicating possible future conversion to total knee arthroplasty. High tibial osteotomy is contraindicated for large corrections because of excessive elevation of the tibial tubercle and overhang of the lateral plateau. Correction in the tibial diaphysis creates a zig zag pattern in the tibia by correcting below the deformity and risks nonunion in cortical bone. There is no evidence that the femur is deformed; therefore, femoral osteotomy is not indicated.
Question 25
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?




Explanation
Giant cell tumors typically occur in a juxta-articular location involving the epiphysis and metaphysis of long bones, usually eccentric in the bone. The radiographs show a destructive process within the distal tibia and an associated soft-tissue mass. The histology shows multinucleated giant cells in a bland matrix with a few scattered mitoses. Osteosarcoma can have a similar destructive appearance but a very different histologic pattern with osteoid production. Ewing's sarcoma also can have a diffuse destructive process in the bone. The histologic pattern of Ewing's sarcoma is diffuse round blue cells. Aneurysmal bone cysts typically are seen as a fluid-filled lesion on imaging studies and have only a scant amount of giant cells histologically. Metastatic adenocarcinoma does not demonstrate the pattern shown in the patient's histology specimen. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
Question 26
Figures 1a and 1b show the sagittal T2- and T1-weighted MRI scans of a 25-year-old intravenous drug abuser who has low back pain that is increasing in intensity. Laboratory studies show a WBC count of 10,000/mm3 and an erythrocyte sedimentation rate of 80 mm/h. Blood culture is negative. Initial management consist of


Explanation
The MRI scans show vertebral diskitis/osteomyelitis. The treatment of spinal infection in adults should be organism specific; therefore, initial management should consist of CT-guided closed biopsy prior to administration of antibiotic coverage. An open biopsy is indicated for a failed closed biopsy or failure of nonsurgical management. Although Staphylococcus aureus is the most common bacteria, a history of intravenous drug abuse raises suspicion for other organisms, including Pseudomonas. Tay BK, Deckey J, Hu SS: Spinal Infections. J Am Acad Orthop Surg 2002;10:188-197.
Question 27
Which of the following is a recognized consequence of hip fusion?

Explanation
Low back pain is an expected long-term complication of fusion; ipsilateral knee laxity is frequently encountered, as is degeneration of the contralateral hip. Hip fusion is equally valuable for both men and women, with both genders reporting satisfactory sexual function. Female patients often deliver by elective Cesarean section, although vaginal deliveries are reported. Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Question 28
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the

Explanation
The sciatic nerve is formed by the roots of the lumbosacral plexus. It exits the pelvis through the greater sciatic notch and appears in the buttock anterior to the piriformus. From that point, the sciatic nerve passes posteriorly over the superior gemellus, obturator internus, inferior gemellus, and quadratus femoris before it passes deep to the biceps femoris. The tendon of the obturator internus passes through the lesser sciatic notch. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347. Anderson JE: Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
Question 29
A 37-year-old man has left shoulder pain and weakness. Coronal T1- and axial T2-weighted MRI scans are shown in Figures 17a and 17b. The biopsy specimen is shown in Figure 17c. What is the most likely diagnosis?



Explanation
A ganglion cyst arising from the posterior labrum of the shoulder is a known cause of suprascapular nerve impingement. The MRI characteristics of low-signal intensity on T1 and high-signal intensity on T2 are seen in lesions with a high fluid content. The histology shows a cavity with a thin fibrous lining. Ferrick MR, Marzo JM: Suprascapular entrapment neuropathy and ganglion cysts about the shoulder. Orthopedics 1999;22:430-434.
Question 30
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?


Explanation
The MRI scans reveal a meso os acromiale with edema at the site in a skeletally mature patient. Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.
Question 31
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?



Explanation
Because the MRI scans show marked dilation and proliferation of lymphatic channels that completely involve all the leg muscles and the clinical photograph shows the severe swelling associated with this disease, the most likely diagnosis is lymphangiomatosis. Poliomyelitis affects the anterior horn cells and manifests as muscle atrophy. Neurofibromatosis can have a similar clinical appearance but usually is associated with other systemic and cutaneous findings. Congenital band syndrome results in amputated or shortened extremities. Chronic venous stasis disease usually is not associated with joint contractures, and typically it affects older individuals. Surgical excision is the only known treatment; this patient underwent an above-knee amputation. Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Question 32
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Explanation
Flap necrosis and infection rates are lowest if free flap coverage is performed within 72 hours of injury. Delays beyond 72 hours are associated with a higher rate of complications. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
Question 33
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include


Explanation
The radiographs show massive subsidence of the lateral side of the tibia with severe tibial bone loss and a fractured proximal fibula. Reconstruction should consist of a large metal or bony lateral tibial augmentation, and a stem long enough to bypass the defect is required. The femoral and tibial components are articulating without any remaining polyethylene medially; therefore, the femoral component is damaged and needs revision. The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250. Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Question 34
A 20-year-old man has a symptomatic lesion of fibrous dysplasia in the femoral neck. Management should consist of
Explanation
Fibrous dysplasia in the femoral neck frequently warrants treatment because of the risk of pathologic fracture. Cortical strut grafts reduce the risk of local recurrence compared with cancellous bone grafting. Because of the consequences associated with fracture in this location, prophylactic fixation is recommended. Radiation therapy and chemotherapy are not used for this benign condition. Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 197.
Question 35
Because the patient shown in Figure 27 can no longer fit in shoes, treatment of the deformity should consist of

Explanation
In local gigantism, a ray resection allows proper fitting of shoes. The ray resection narrows the foot and shortens the length. The foot may require further surgery with growth. Debulking, physeal arrest, and distal phalanx amputation are unlikely to be effective. Turra S, Santini S, Cagnoni G, Jacopetti T: Gigantism of the foot: Our experience in seven cases. J Pediatr Orthop 1998;18:337-345.
Question 36
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 37
A 58-year-old man has anterior knee pain after undergoing total knee arthroplasty for osteoarthritis 2 years ago. He denies any history of trauma. A Merchant view is shown in Figure 20. What is the most likely cause of his pain?

Explanation
The patient has a patellar stress fracture after resurfacing in a total knee arthroplasty. Several studies have shown that over-resection of the patella to less than 12 to 15 mm increases anterior patellar surface strains to a point where the risk of fracture is increased. Increasing the patellar thickness, positioning of the femoral component, lateral releases, and component types have not been clearly associated with increased fracture risk. Reuben JD, McDonald CL, Woodard PL, Hennington LJ: Effect of patella thickness on patella strain following total knee arthroplasty. J Arthroplasty 1991;6:251-258. Hsu HC, Luo ZP, Rand JA, An KN: Influence of patellar thickness on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty 1996;11:69-80.
Question 38
A 12-year-old boy with hemophilia A and no known inhibitors sustains a tibia fracture and has pain with passive motion of the deep toe flexors. Appropriate management should consist of
Explanation
In a patient with hemophilia, factor replacement followed by assessment of compartment pressures is essential. If the patient has inhibitors, the problem is more difficult. Porcine factor has been helpful in patients with inhibitory antibodies. Recent evidence points to using activated factor VII and bypassing the intrinsic pathway. Desmopressin is an adjunct to therapy but is not as effective as factor VII. Dumontier C, Sautet A, Man M, Bennani M, Apoil A: Entrapment and compartment syndromes of the upper limb in haemophilia. J Hand Surg Br 1994;19:427-429. Carr ME Jr, Loughran TP, Cardea JA, Smith WK, Kuhn JG, Dottore MV: Successful use of recombinant factor VIIa for hemostasis during total knee replacement in a severe hemophiliac with high-titer factor VIII inhibitor. Int J Hematol 2002;75:95-99.
Question 39
In the spine, osteoblastomas usually originate in the

Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 40
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern?
Explanation
Although symptomatic thoracic disk herniations can affect more caudal structures, even to the point of paralysis, the pattern of radiating pain has been described as either following the dermatomal band around the chest or feeling to the patient as if the pain passes straight anteriorly to the chest wall.
Question 41
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?

Explanation
The lesion has the typical "blown out" lytic radiographic appearance that is most commonly found in thyroid or renal cell metastases. Given the history of hematuria and histology findings, the most likely diagnosis is metastatic renal cell carcinoma. This tumor is relatively resistant to chemotherapy. Radiation therapy is used as a postoperative adjuvant treatment with varying response rates. Surgery should be performed after preoperative embolization to decrease the risk of intraoperative bleeding, as no tourniquet can be used in this location. Patients with metastatic renal cell carcinomas may survive for years, resulting in a higher likelihood of local tumor progression with ineffective adjuvant therapy. Intramedullary fixation combined with curettage and cementation will provide the best chance of local control while maintaining the patient's native shoulder and elbow joints. A total humeral resection is an extensive surgery with considerable morbidity and is not indicated for this patient because less extensive surgery is likely to be effective. Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054. Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 42
Which of the following is considered the most common long-term effect on the spine of a professional race horse jockey?
Explanation
Horseback riding is a sport that directly affects the jockey's spine. Tsirikos and associates reported the results of a study of 32 jockeys. They found that equestrian sports, especially professional horseback riding, apart from the increased risk of direct spinal injury caused by a fall from the horse, can lead to progressive spinal degeneration as a result of repetitive trauma and increased physical stress on the spine. It is associated with spondylosis of the cervical spine and lumbar spine. Tsirikos A, Papagelopoulos PJ, Giannakopoulos PN, et al: Degenerative spondyloarthropathy of the cervical and lumbar spine in jockeys. Orthop 2001;24:561-564.
Question 43
A 46-year-old woman who was involved in a motor vehicle accident reports a 4-month history of right-sided lower back pain and pain radiating into the right thigh. The patient underwent an extensive 3-month course of physical therapy and now is dependent on narcotic medication for pain control. Epidural injection therapy has failed to improve her symptoms. Examination is significant for weakness of hip flexion in the seated position and for decreased sensation to light touch in the medial anterior thigh region. Straight leg raise is negative, but the femoral stretch test reproduces anterior thigh pain. A CT myelogram image, at L3-L4, is shown in Figure 3. What is the most appropriate management at this time?

Explanation
The CT scan reveals a right-sided lateral disk protrusion at L3-4 that has been symptomatic for more than 4 months despite appropriate nonsurgical management. Relative surgical indications include persistent radiculopathy despite an adequate trial of nonsurgical management, recurrent episodes of sciatica, persistent motor deficit with tension signs and pain, and pseudoclaudication caused by underlying stenosis. Whereas studies have shown improvement in patients with sciatica from a lumbar disk herniation treated either nonsurgically or surgically, those undergoing surgical treatment had an overall greater improvement of symptoms. Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Question 44
Based on the appearance of the imaging studies shown in Figures 11a through 11c, what structure has most likely been injured?



Explanation
The radiographs reveal marked lateral subluxation of the patella in a patient who has recurrent patellar instability. The medial patellofemoral ligament is the main restraint to lateral subluxation of the patella. Boden BP, Pearsall AW: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
Question 45
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown in Figure 18. What is the most likely diagnosis?

Explanation
Ganglia involving the cruciate ligaments have been recently reported as a cause of knee pain that interferes with knee flexion and extension. The symptoms are poorly localized in this patient and not along the medial joint line, making the diagnosis of a torn medial meniscus less likely. In addition, the MRI findings do not show a significant medial meniscal lesion. A Baker's cyst is usually posteromedial and extends posterior to the interval between the medial head of the gastrocnemius and semimembranosus. MRI scans show a fluid-filled lesion with an increased signal on T1- and T2-weighted images. A lipoma would be bright on the T1-weighted image only. Deutsch A, Veltri DM, Altchek DW, et al: Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 1994;10:219-223.
Question 46
A 37-year-old racquet player had dominant shoulder pain for 1 year, and cortisone injections provided only temporary relief. Because MRI findings did not reveal a rotator cuff tear, he underwent arthroscopic treatment including subacromial decompression and spur removal below the distal clavicle. Three years following surgery, he now reports that the pain has returned. What is the most likely cause of his pain?
Explanation
Co-planing the distal clavicle may lead to painful acromioclavicular joints in up to 35% of patients; this is felt to be related to destabilizing the distal clavicle. Intra-articular diagnosis of synovitis, degenerative joint disease, and superior labrum anterior and posterior lesions would have been identified at initial arthroscopy (not necessarily seen in open surgery). Ganglions are seen on MRI. Fischer BW, Gross RM, McCarthy JA: Incidence of acromioclavicular joint complications after arthroscopic subacromial decompression. Arthroscopy 1999;15:241-248. Hazel RM, Tasto JP, Klassen J: Arthroscopic subacromial decompression: A 9-year follow-up. Arthroscopy 1998;14:419.
Question 47
Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?

Explanation
The initial stages of posterior tibial tendon insufficiency, where the deformity remains supple, may be treated with bracing or an orthotic for pain relief. The Arizona brace was introduced in 1988, and assists in pain relief and deformity correction by minimizing hindfoot valgus alignment, lateral calcaneal displacement, and medial ankle collapse. It is particularly helpful in those patients with advanced disease that cannot tolerate an ankle-foot orthosis. All other choices are incorrect because of the addition of lateral posting, which is not advantageous in valgus deformities. The addition of medial posting to any of the above choices would render them correct alternatives. A heel lift is applicable in Achilles tendon disorders, not posterior tibial tendon disorders. Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Question 48
Figures 42a through 42c show the clinical photographs and radiograph of a patient with diabetes mellitus who lives independently. The patient was admitted to the hospital late yesterday afternoon with clinical signs of sepsis. Parenteral antibiotic therapy resolved the sepsis, and blood glucose levels are now well controlled. The patient has no palpable pulses. The ankle-brachial index is 0.70. Laboratory studies show a WBC count of 8,500/mm3, a serum albumin of 1.9 g/dL, and a total lymphocyte count of 1,500/mm3. What treatment has the best potential to optimize his survival and independence?



Explanation
The patient was admitted to the hospital with sepsis. The sepsis has resolved, leaving the patient with a negative nitrogen balance. Now that the patient is stable, metabolic support should be used to optimize his nutrition. If the serum albumin can be increased to 2.5 g/dL, he has an excellent potential to heal an amputation at the Syme ankle disarticulation level; a level that will optimize his functional independence. Pinzur MS, Stuck RR, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Question 49
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?

Explanation
The MRI arthrogram reveals dye extravasation into the labrum, consistent with a labral tear. The MRI findings are not typical of osteonecrosis, stress fracture, or transient osteoporosis. There is no increase in bone marrow edema in the neck or femoral head. Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
Question 50
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Explanation
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
Question 51
A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm3. The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?

Explanation
Synovial fluid analysis is a very sensitive tool for detecting infection in total knee arthroplasties. Several studies have demonstrated that an absolute leukocyte count in the synovial fluid of less than 1,700 to 2,500/mm3 is an accurate predictor of absence of infection. Similarly, a differential cell count of the WBCs demonstrating less than 50% to 60% neutrophils is an accurate predictor of absence of infection. If both parameters are normal, it is unlikely that the patient has an infection. The three surgical options are contraindicated based on the normal examination findings and laboratory parameters. Similarly, antibiotics should be avoided. The work-up should include tests to evaluate noninfectious sources of knee pain and sources of referred knee pain. Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562. Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.
Question 52
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?

Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 53
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?

Explanation
The radiograph reveals an increased first-second intermetatarsal angle and a congruent metatarsophalangeal joint with an abnormal distal metatarsal articular angle. Correction of both of these abnormalities requires a proximal and distal first metatarsal osteotomy. Coughlin M: Juvenile bunions, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 297-339.
Question 54
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?

Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve. Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Question 55
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?



Explanation
The osseous sites most frequently involved by giant cell tumor of bone are the distal femur, proximal tibia, and distal radius with approximately 10% of giant cell tumors involving the distal radius. The goals of treatment are to remove the tumor completely and to preserve maximum function of the extremity.
Question 56
Examination of a supine patient in which the hip is abducted, externally rotated, and flexed is referred to as

Explanation
During Patrick's test, also known as the FABER test, the flexed, abducted, and externally rotated hip is positioned to isolate sacroiliac pathology. Back pain with this test is not considered diagnostic. With Kernig's sign, the spinal cord is placed on stretch, eliciting root or meningeal irritation by forcibly flexing the patient's head and neck with his or her hands clasped behind the head. For Lasegue's sign, the patient performs a straight leg raise with the immobile hip already held in flexion. The femoral stretch test can be performed in the prone position or side lying, but the hip is held in extension while the knee is flexed, testing for femoral neuritis. Watkins RG: History, physical examination, and diagnostic tests for back and lower extremity problems, in Watkins RG (ed): The Spine in Sports. St Louis, MO, Mosby, 1996, Chapter 7.
Question 57
A 40-year-old man with an acetabular chondrosarcoma has a small soft-tissue mass. Treatment should consist of

Explanation
The treatment of choice for pelvic chondrosarcoma is wide resection via an internal hemipelvectomy. Chondrosarcoma requires surgical resection for control and does not respond to traditional chemotherapy or external beam radiation. Hip arthroplasty with acetabular reconstruction and curettage and cementation of the lesion are intralesional procedures that result in a higher incidence of local recurrence of tumor. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 58
A 6-year-old boy has leg pain. A radiograph, MRI, CT, and bone scans, and a biopsy specimen are shown in Figures 14a through 14e. What is the most likely diagnosis?





Explanation
From an imaging point of view, all of the diagnoses are possible. Biopsy results and cultures are necessary to make the diagnosis. The biopsy specimen shows inflammatory cells and necrotic bone, consistent with osteomyelitis. Fletcher BD, Hanna SL: Pediatric musculoskeletal lesions simulating neoplasms. Magn Reson Imaging Clin N Am 1996;4:721-747.
Question 59
A previously asymptomatic 14-year-old girl sustained a twisting injury to her ankle. Radiographs are shown in Figures 2a and 2b. Management should consist of


Explanation
The radiographs show a well-defined, irregular, eccentric lesion in the distal tibia metaphysis with a thin sclerotic margin. The radiographs are diagnostic of nonossifying fibroma, a common entity in this age group and in this location. No further work-up is indicated. The patient was asymptomatic prior to the injury and the lesion is small and thus not worrisome for an impending pathologic fracture; therefore, no treatment is indicated beyond observation. The natural history of these lesions is to gradually ossify as the patient reaches skeletal maturity. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 60
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?


Explanation
In this patient, examination reveals an inability to extend the fingers with the wrist extended, but full extension is possible with wrist flexion. These findings demonstrate isolated tenodesis of the flexor digitorum to the ring and little fingers. These findings are not consistent with compartment syndrome or nerve injury. Scarring or entrapment of tendons in forearm fractures can occur. Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128. Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184. Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
Question 61
What type of exercise is used early in the rehabilitation process to safely stimulate co-contraction of the scapular and rotator cuff muscles?

Explanation
Closed kinetic chain exercises are used early in the rehabilitation process. The distal segment is fixed, and an axial load is applied which provides glenohumeral compression and reduces the demand on the rotator cuff. These exercises stimulate co-contractions of the scapular and rotator cuff muscles, load scapular stabilizers, and facilitate active motion. Facilitated active motion exercises use proximal segment motion to stimulate and facilitate motion in the target tissue. These exercises are often performed in diagonal movements. Resistive active motion exercises are used later in the rehabilitation process. These are typically open kinetic chain exercises that involve active glenohumeral motion with extrinsic loads such as weights or exercise tubing. During the later stages of upper extremity rehabilitation, plyometrics are added. These exercises help to prepare the athlete for return to sport. When performed at slower speeds, these exercises emphasize stabilization and control. As the speeds increase, muscles begin to work in the stretch-shortening sequence associated with sports participation. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 129-136.
Question 62
An 8-year-old boy is diagnosed with acute onset cauda equina syndrome. A radiograph, MRI scans, and a biopsy specimen are shown in Figures 57a through 57d. What is the most appropriate treatment?




Explanation
The findings are consistent with an aneurysmal bone cyst. The MRI scan demonstrates a lesion involving the posterior elements of the vertebrae with fluid-fluid levels and neural compression. Fibrovascular tissue with multinucleated giant cells surrounding a vascular lake is seen on the histology. The most appropriate treatment is a marginal resection of the involved posterior elements. Although the recurrence rate can be as high as 25% to 30%, wide surgical resection could result in permanent neurologic injury and is not necessary. Aspiration and steroid injection have been advocated but would not relieve the nerve compression in this patient. Radiation therapy and chemotherapy are not indicated. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, et al: Aneurysmal bone cyst: A review of 150 patients. J Clin Oncol 2005;23:6756-6762.
Question 63
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced

Explanation
The literature supports similar clinical outcomes after surgical and nonsurgical methods. The chief difference lies in the complications between the groups. Surgical patients experience more wound problems but a significantly lower rerupture rate. Although suturing the tendon allows earlier mobility, the tendon healing time is unchanged. Nonsurgical methods are less expensive to provide. Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036. Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Question 64
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?

Explanation
Localized PVNS is a form of the disease in which synovial proliferation is restricted to one area of a joint and causes the formation of a small mass-like lesion. The true incidence of this is unknown but is probably less common than the diffuse form of the disease. PVNS presents as a usually painful discrete mass. The anterior compartment of the knee is the most common location. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
Question 65
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of


Explanation
The patient has aseptic loosening of the original semiconstrained prosthesis and significant proximal ulnar bone destruction; therefore, the treatment of choice is revision arthroplasty using a semiconstrained design. Although orthotic stabilization could be used, it will not provide long-term pain relief. Resection arthroplasty after removal of the components may lead to painful instability. Elbow arthrodesis would be difficult with the bone stock loss and is not considered the best option. Two main contraindications to the use of an unconstrained prosthesis are significant bone loss and previous use of a hinged or semiconstrained prosthesis. An ulnar allograft could be combined with the use of a semiconstrained long-stemmed ulnar prosthesis as a treatment modification. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 66
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 67
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Explanation
Flexor digitorum profundus rupture or "rugger jersey finger" often occurs in the ring finger after the player misses a tackle and catches the digit on the shirt of the opposing player. Surgical repair is required for zone I-type injuries. Moiemen NS, Elliot D: Primary flexor tendon repair in zone I. J Hand Surg Br 2000;25:78-84.
Question 68
What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?


Explanation
This intra-articular distal humerus fracture with displacement at the joint surface is best treated with surgical fixation. The most biomechanically sound construct is two plates applied to either column 180 degrees from one another. Elbow arthroplasty is most appropriate for low demand elderly patients. Schemitsch EH, Tencer AF, Henley MB: Biomechanical evaluation of methods of internal fixation of the distal humerus. J Orthop Trauma 1994;8:468-475. McCarty LP, Ring D, Jupiter JB: Management of distal humerus fractures. Am J Orthop 2005;34:430-438.
Question 69
A 25-year-old competitive skier sustains a twisting injury to the right ankle while skiing. She is unable to continue the activity secondary to severe lateral ankle pain. Examination reveals ecchymosis and fullness over the lateral malleolus with pain and weakness on active ankle dorsiflexion and external rotation. There is no medial-sided pain. Neurovascular examination is normal. An AP radiograph and MRI scan are shown in Figures 17a and 17b, respectively. Management should consist of


Explanation
The MRI scan shows a dislocated peroneus brevis tendon with disruption of the peroneal retinaculum. This injury is commonly seen in skiers and is the result of peroneal contraction with the ankle everted and dorsiflexed. Nonsurgical management is rarely successful; therefore, repair of the peroneal retinaculum is the treatment of choice. Eckert WR, Davis EA Jr: Acute rupture of the peroneal retinaculum. J Bone Joint Surg Am 1976;58:670-672. Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Question 70
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?

Explanation
The natural history of nontraumatic osteonecrosis varies greatly, so it is difficult to predict which patients will have severe arthrosis develop. Patients with sickle cell disease tend to have the most benign course. The most commonly reported cause of nontraumatic osteonecrosis is corticosteroid therapy. Fortunately, the incidence of osteonecrosis among patients treated with long-term systemic corticosteroids has fallen from more than 25% to less than 5% in recent years, owning to judicious steroid use and dosing. The interval between corticosteroid administration and the onset of shoulder symptoms is also variable, ranging from 6 to 18 months in one large series. This is comparable to the interval leading up to the onset of hip symptoms, which ranges from 6 months to 3 years or longer. The incidence of humeral head involvement has not been shown to vary with the underlying indication for steroid use. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298.
Question 71
An 8-year-old boy sustained an isolated distal radial fracture that was reduced and immobilized with 10 degrees of residual dorsal tilt. What is the next step in management?

Explanation
Distal radial fractures in children are common, and a large amount of displacement is acceptable. In general, 20 degrees of dorsal displacement and complete bayonet apposition in girls to age 12 years and in boys to age 14 years can be expected to remodel with an excellent outcome. The potential for increased fracture displacement and subsequent malunion may exist in up to one third of patients with displaced fractures with less than anatomic reduction. Therefore, early follow-up is recommended and remanipulation is indicated should loss in reduction occur. Consideration for percutaneous pinning of isolated distal radial fracture is reasonable in patients with little growth remaining. In these patients, higher rates of redisplacement exist with little chance for remodeling. Gibbons CL, Woods DA, Pailthorpe C, et al: The management of isolated distal radius fractures in children. J Pediatr Orthop 1994;14:207-210. McLauchlan GJ, Cowan B, Annan IH, et al: Management of completely displaced metaphyseal fractures of the distal radius in children. J Bone Joint Surg Br 2002;84:413-417. Proctor MT, Moore DJ, Patterson JH: Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br 1993;75:453-454.
Question 72
What is the primary concern for arthrodesis of a failed infected total knee arthroplasty using internal fixation?
Explanation
Arthrodesis of the failed infected total knee arthroplasty may be accomplished by external fixation, intramedullary rod fixation, and dual plates and screws. External fixation runs the risk of pin tract infection, although after its removal, there are no metal surfaces left in place. Intramedullary rods have been used successfully in the treatment of infected total knees, although they also leave metal within the region of the infection. The dual plate technique of knee fusion is useful in patients with rheumatoid arthritis who require fusion in the absence of infection because it provides good initial stability and avoids the use of external pins. However, in the face of infection, the large surface area of the screws and plates may serve as a site for bacteria to hide within a glycocalyx and make eradication of the infection almost impossible.
Question 73
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
The association of a nail puncture wound with a gram-negative infection (Pseudomonas aeruginosa) has been attributed to the local environmental factors in shoes. Osteomyelitis is rare, occurring only in about 1% of patients. Tetanus prophylaxis should be given if it is not up to date. While the remaining organisms listed are periodically involved, they are more common in patients who are immunocompromised or who have diabetes mellitus. Therefore, obtaining a culture of the infected wound is appropriate in such individuals because of the multifactorial nature of the infection. Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Question 74
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?



Explanation
Nodular fasciitis is a pseudosarcomatous, self-limiting reactive process composed of fibroblasts and myofibroblasts. Most patients give a history of a rapidly growing mass that has been present for only a few weeks. Many have pain associated with the mass and can recall a specific traumatic event predating the presence of the lesion. It can occur at any age but is most commonly seen in adults who are 20 to 40 years of age. Histologically, the lesion is composed of predominantly plump, immature-appearing fibroblasts that bear a close resemblance to the fibroblasts found in granulation tissue. Characteristically, the fibroblasts are arranged in short, irregular bundles and fascicles and are adjacent to collagen and reticulin. The lesions can appear to be more myxoid or more fibrotic in nature and this correlates to the duration of symptoms. The lesions with a short duration of symptoms have a more myxoid appearance in contrast to those of longer duration characterized by hyaline fibrosis. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 250-266.
Question 75
A 34-year-old man has had a 13-month history of an equinovarus deformity of the foot and ankle after a motorcycle accident. His foot and ankle are flexible, but bracing has become uncomfortable. Active dorsiflexion and eversion are absent. What is the most appropriate treatment?

Explanation
Arthrodesis of any of the ankle or hindfoot joints should be reserved for fixed deformities or end-stage degenerative arthritis. Achilles tendon lengthening is necessary to correct the equinus and to improve dorsiflexion-plantar flexion balance. Similarly, transfer of the posterior tibialis tendon reduces both plantar flexion and inversion torque. Hansen ST: Function Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 442-447.
Question 76
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?


Explanation
The MRI scans show a paralabral cyst, which is most commonly associated with labral tears. Compression of the suprascapular nerve results in weakness of the supraspinatus and/or infraspinatus depending on the level of compression. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 77
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
It is well known that suprascapular nerve entrapment can be secondary to many entities, and its association with ganglion cysts and SLAP lesions has been well documented. Because of a superior labral tear, synovial fluid will leak out of the joint underneath the labrum, causing the cyst and secondary compression of the nerve. Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734. Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Question 78
Which of the following anatomic structures is often difficult to visualize during elbow arthroscopy?

Explanation
The ulnar collateral ligament is often difficult to visualize during elbow arthroscopy. It can be seen clearly in only 10% to 30% of elbow arthroscopies. All of the other structures should be easily and thoroughly seen and palpated during elbow arthroscopy. Johnson LL: Arthroscopic Surgery: Principles and Practice. St Louis, MO, CV Mosby, 1988.
Question 79
High Yield
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?

Explanation
Symphyseal widening of greater than 2.5 cm and less than 5 cm denotes an AP II injury and a rotationally unstable pelvis. An AP II pelvic ring injury is best treated with anterior open reduction and internal fixation. Nonsurgical management is reserved for AP I injuries. Pelvic binders are used only acutely and should not be used for definitive management. Iliosacral screws usually are not necessary in the acute management of AP II injuries. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 80
A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45 degrees of valgus laxity at the metacarpophalangeal (MCP) joint. Examination of the right thumb shows 25 degrees of valgus laxity at the MCP joint. Radiographs are normal. Management should consist of
Explanation
The patient has a complete tear of the ulnar collateral ligament as defined by MCP joint laxity of greater than 30 degrees (or 15 degrees greater laxity compared with the opposite side). Primary repair is the treatment of choice because displacement of the ligament superficial to the adductor aponeurosis (Stener lesion) must be corrected. Any volar plate injury can be addressed during repair of the ulnar collateral ligament.
Question 81
A 43-year-old soccer player who had knee pain following a twisting injury underwent an arthroscopic meniscectomy 6 months ago. He continues to report posterior knee pain. Examination reveals soft-tissue fullness and tenderness just above the popliteal fossa, trace knee effusion, full range of knee motion, no instability, and negative meniscal signs. Radiographs show some mild medial joint space narrowing but no other bony changes. What is the next most appropriate step in management?
Explanation
The phenomenon of tumors misdiagnosed as athletic injuries has been termed "sports tumors." Lewis and Reilly presented a series of 36 patients who initially were thought to have a sports-related injury but ultimately were diagnosed with a primary bone tumor, soft-tissue tumor, or tumor-like condition. Muscolo and associates presented a series of 25 tumors that had been previously treated with an intra-articular procedure as a result of a misdiagnosis of an athletic injury. Initial diagnoses included 21 meniscal lesions, one traumatic synovial cyst, one patellofemoral subluxation, one anterior cruciate ligament tear, and one case of nonspecific synovitis. The final diagnoses were a malignant tumor in 14 patients and a benign tumor in 11 patients. The authors noted that oncologic surgical treatment was affected in 15 of the 25 patients. The most frequent causes of erroneous diagnosis were initial poor quality radiographs and an unquestioned original diagnosis despite persistent symptoms. Persistent symptoms warrant further diagnostic studies, not additional treatment such as physical therapy, corticosteroid injection, or an unloader brace. Although a bone scan may be helpful in this case and confirm arthrosis of the medial compartment, the suspicion of a soft-tissue mass makes MRI the imaging modality of choice. Muscolo DL, Ayerza MA, Makino A, et al: Tumors about the knee misdiagnosed as athletic injuries. J Bone Joint Surg Am 2003;85:1209-1214.
Question 82
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the

Explanation
The recurrent laryngeal nerve lies between the trachea and the esophagus and is subject to stretch injury if excessive retraction is applied. The vagus nerve lies in the carotid sheath. The sympathetic trunk lies anterior to the longus colli muscles. The hypoglossal nerve and superior laryngeal nerve are both at risk during the exposure but are not located between the trachea and esophagus. An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1998, chapter 2.
Question 83
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
Surgical decompression is unnecessary in a patient with no neurologic deficit and canal compromise of less than 50%. A compression deformity of less than 50% and kyphosis of less than 30 degrees may be successfully treated with a TLSO extension brace. Deformity in this range will reliably heal with minimal risk for late deformity or residual pain. Although some studies suggest 6 weeks of bed rest as treatment, early mobilization and bracing is preferred. Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures. Paraplegia 1995;33:73-76. Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 84
Figure 17 shows the radiograph of an 11-year-old boy with Duchenne muscular dystrophy who has been nonambulatory for the past 2 years. Management of the spinal deformity should consist of

Explanation
The presence of any curve greater than 20 degrees in a nonambulatory patient with Duchenne muscular dystrophy is an indication for posterior fusion with instrumentation. Because of progressive cardiomyopathy and pulmonary deficiency, waiting until the curve is larger can increase the risk of pulmonary or cardiac complications during or following surgery. There is some disagreement as to whether all such fusions must extend to the pelvis. Bracing or other nonsurgical management is ineffective and is not indicated in this situation. Sussman M: Duchenne muscular dystrophy. J Am Acad Orthop Surg 2002;10:138-151.
Question 85
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?

Explanation
An isolated tear of the subscapularis tendon has been noted as early as 1835 by Smith. In Gerber and associates' 1991 report of 16 men with an average age of 51 years, isolated subscapularis tendon rupture was often caused by a violent hyperextension injury. All patients reported pain anteriorly along with night pain. They also noted pain and weakness of the arm. The lift-off test is performed by having the patient lift the palm of the hand away from the small of the back. The patient must have sufficient internal rotation to allow this test to be performed. A subscapularis rupture is likely if the patient cannot perform the lift-off test. Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394. Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 86
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?

Explanation
Suprascapular nerve injuries are more commonly seen in athletes who participate in overhead activities. When a patient is evaluated for posterior shoulder pain and infraspinatus muscle weakness or atrophy, electrodiagnostic studies are an essential part of the evaluation. In addition, imaging studies are indicated to exclude other diagnoses that can mimic a suprascapular nerve injury. Initial management should consist of cessation of the aggravating activity along with an organized shoulder rehabilitation program. If nonsurgical management fails to provide relief within 6 months to 1 year, surgical exploration of the suprascapular nerve should be considered. Release of the spinoglenoid ligament with resultant suprascapular nerve decompression may result in pain relief and a return of normal shoulder function. In this patient, who has a chronic neuropathy and mild symptoms, surgery is indicated only if nonsurgical management fails to provide relief and he is unable to perform at his position. Cummins CA, Bowen M, Anderson K, et al: Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med 1999;27:810-812. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Question 87
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
The history is most consistent with a plantar fibroma. The nodules typically are located within the substance of the plantar aponeurosis. The clinical appearance is usually diagnostic without the need for advanced imaging studies. While the lesion may be prominent and painful to direct palpation, the anatomic location is usually off of the weight-bearing surface. Observation with or without an accommodative orthotic is the treatment of choice. Recurrence is common following attempted excision. Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 88
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?

Explanation
On T1-weighted images, the posterior cruciate ligament is a low-signal (black) structure that courses from the posterior aspect of the tibia to the medial femoral condyle. The posterior cruciate ligament can appear as arcuate, U-shaped, or kinked. The other structures have similar signal but different anatomic locations. Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Question 89
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of



Explanation
The plain radiograph and tomogram show an abnormality of the upper cervical spine, with erosion of the dens. The MRI scan shows evidence of cord impingement. The cervical spine is frequently involved in polyarticular JRA. Stiffness and autofusion are commonly seen, but C1-2 instability can also occur secondary to synovitis and bony erosion. Basilar invagination is rare in JRA. There is no consensus regarding fusion in the asymptomatic patient. In patients with symptoms and neurologic signs, C1-2 posterior fusion is indicated. Fried JA, Athreya B, Gregg JR, Das M, Doughty R: The cervical spine in juvenile rheumatoid arthritis. Clin Orthop 1983;179:102-106.
Question 90
Which of the following is considered the most common complication of the impaction grafting technique for femoral revision surgery?
Explanation
Impaction grafting technique for femoral revision surgery has become increasingly popular over the past decade. This technique is designed to address cavitary deficiencies of the femur. The femoral stem is inserted with cement fixation. Its clinical efficacy has not been shown to be superior to extensively porous-coated stems. Early subsidence of the stem has been reported in more than 50% of the patients. However, loss of fixation has occurred infrequently (5%) in reported series conducted by experienced surgeons. It has not been shown to have a higher infection rate. Gie GA, Linder L, Ling RS, Simon JP, Slooff TH, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Question 91
Lumbar disk replacement has been shown to offer which of the following results?
Explanation
There is no clear evidence that disk replacement results in pain relief that is superior to fusion. Pain relief appears to be equivalent with these two procedures. No study has clearly demonstrated that normal segmental motion has been consistently restored. Preexisting facet arthropathy is considered to be a contraindication to disk replacement. Comparative long-term data demonstrating a reduced incidence of adjacent segment disease compared to fusion are not yet available. Geisler FH, Blumenthal SL, Guyer RD, et al: Neurological complications of lumbar artificial disc replacement and comparison of clinical results with those related to lumbar arthrodesis in the literature. J Neurosurg Spine 2004;1:143-154.
Question 92
A 75-year-old woman reports foot pain and states that her foot has become progressively "flatter" in the past 3 years. Custom inserts and physical therapy have failed to provide relief. Examination reveals a flexible hindfoot and mild heel cord contracture. The patient is able to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 21a through 21d. What is the most appropriate surgical management?




Explanation
The patient has end-stage midfoot arthritis, with a secondary flatfoot deformity through the midfoot. The ability to perform a single limb heel rise indicates that the posterior tibial tendon is functioning, and the weight-bearing radiographs show normal calcaneal pitch and talar head coverage, thus confirming that the flatfoot deformity is isolated to the midfoot. Therefore, the most appropriate treatment is medial column arthrodesis and heel cord lengthening. The other listed procedures are not indicated because they are used in the management of adult flatfoot from posterior tibial tendon insufficiency. Toolan BC: Midfoot arthrodesis: Challenges and treatment alternatives. Foot Ankle Clin 2002;7:75-93.
Question 93
A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindfoot deformity. A lateral radiograph is shown in Figure 6. Surgical reconstruction is best accomplished with

Explanation
The patient has posttraumatic subtalar joint arthrosis that developed following a calcaneal fracture. Because there is no hindfoot deformity, in situ subtalar joint arthrodesis is the treatment of choice. Calcaneal osteotomy or distraction bone block arthrodesis is beneficial in patients with severe talar dorsiflexion or malunion of the calcaneal body. Triple arthrodesis is not warranted without changes at the transverse tarsal joint, and typically even with injury into the calcaneocuboid joint, this joint is often asymptomatic. Pantalar arthrodesis is not indicated as the pathology is occurring at the subtalar joint and not in the ankle joint. Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1422-1464. Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 94
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of

Explanation
The patient has a type IIIB patellar fracture (inferior pole fracture with an intact patellar tendon). Nonsurgical management is the treatment of choice if there is little displacement and the extensor mechanism is intact. Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Question 95
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
Alendronate is a second-generation bisphosphonate, and it can cause epigastric distress in up to 30% of patients. This side effect can be minimized by gradually building up to therapeutic doses over a period of 4 to 8 weeks. Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
Question 96
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
The recurrent laryngeal nerve provides innervation to the vocal cords and was the most common neurologic injury reported in a series of 36,000 patients. The nerve is felt to be more vulnerable during a right-sided approach because of its anatomic course. A recent study has also suggested a role for increased endotracheal cuff pressures in this nerve injury. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 97
Consider the theoretic articulation shown in Figure 11 as femoral and tibial components of a total knee prosthesis in which the components fit like a "roller in trough." Which of the following best describes the articulation?

Explanation
The theoretic total knee components will resist anteroposterior motion by making the femoral component "climb the walls" of the tibial component. As drawn, there is no constraint to medial-lateral translation. The cylinder is not rounded on the edges, so varus-valgus motion will impart load from the cylinder to the trough over a small area, thus having a high contact stress.
Question 98
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of

Explanation
The patient requires an arthrodesis of the first metatarsophalangeal joint because of the abnormal neuromuscular forces. The more traditional bunionectomies such as a distal chevron bunionectomy, a proximal first metatarsal osteotomy, and a double osteotomy have a high failure rate because of the underlying Down syndrome. The Keller procedure is indicated for older, sedentary individuals and has little role in the management of a neuromuscular bunion. Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Question 99
A 23-year-old woman falls from a bicycle and sustains a right knee injury. Figures 12a through 12d show radiographs and MRI scans of the knee. What is the most likely diagnosis?




Explanation
The radiographs and MRI scans both show an avulsion of the anterior cruciate ligament, which has been described by Meyers and McKeever in three different fracture patterns. Type I fractures are nondisplaced or have minimal displacement of the anterior margin. Type II fractures have superior displacement of their anterior aspect with an intact posterior hinge. Type III fractures are completely displaced. Although the injury is visible on the radiographs, it is more subtle in adults than children. Thus, MRI is helpful in clarifying this injury in adults. Open or arthroscopic reduction and internal fixation is recommended for type II and type III fractures that do not respond to closed reduction. Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684. Wiss DA, Watson JT: Fractures of the tibial plateau, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults. Philadelphia, PA, Lippincott-Raven, 1996, pp 1920-1953.
Question 100
Joint contact pressure in normal or artificial joints can best be minimized by what mechanism?
Explanation
Joint contact pressure is a stress and as such is defined as the load transferred across the joint divided by the contact area between the joint surfaces (the area over which the joint load is distributed). Therefore, any mechanism that decreases the load across the joint (eg, a walking aid) will decrease the stress. Similarly, any mechanism that increases the area over which the load is distributed (eg, using a more conforming set of articular surfaces in a knee joint arthroplasty) will also decrease the stress. Other mechanisms that influence joint contact pressure include the elastic modulus of the materials (cartilage in the case of natural joints and polyethylene in joint arthroplasty) and the thickness of the structures through which the joint loads pass. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in UHMWPE components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051.
