Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Joint contact pressure in normal or artificial joints can best be minimized by what mechanism?
Explanation
Joint contact pressure is a stress and as such is defined as the load transferred across the joint divided by the contact area between the joint surfaces (the area over which the joint load is distributed). Therefore, any mechanism that decreases the load across the joint (eg, a walking aid) will decrease the stress. Similarly, any mechanism that increases the area over which the load is distributed (eg, using a more conforming set of articular surfaces in a knee joint arthroplasty) will also decrease the stress. Other mechanisms that influence joint contact pressure include the elastic modulus of the materials (cartilage in the case of natural joints and polyethylene in joint arthroplasty) and the thickness of the structures through which the joint loads pass. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in UHMWPE components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051.
Question 2
What type of multiple lesions is associated with Maffucci's syndrome?
Explanation
Maffucci's syndrome is a form of enchondromatosis associated with subcutaneous and deep hemangiomas. Similar to Ollier's disease, the risk of malignant transformation of the enchondromas is much higher than that of a solitary enchondroma. Multifocal nonossifying fibromas associated with other clinical findings such as mental retardation and café-au-lait spots is known as Jaffe-Campanacci syndrome. There are two types of multifocal forms of histiocytosis: Letterer-Siwe and Hand-Schüller-Christian disease. Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274. Frassica F: Orthopaedic pathology, in Miller M (ed): Review of Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1996, pp 292-335.
Question 3
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
Explanation
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted. Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Question 4
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of

Explanation
The patient has symptomatic grade IV Brooker heterotopic ossification. Once the bone has matured, it can be excised. Surgical excision should be combined with postoperative irradiation to avoid recurrence. Pharmacologic and irradiation intervention are not successful beyond the perioperative period unless they are combined with surgical excision of mature heterotopic ossification. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 5
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Explanation
Traditional surgeries for anterior cruciate ligament-deficient knees carry the potential risk of premature physeal closure in young athletes. Therefore, most surgeons are reluctant to recommend intra-articular reconstruction using bone tunnels with bone-patellar tendon-bone autografts or hamstring tendons. The current recommendation for young athletes is activity modification, rehabilitation, and functional bracing until the patient is near skeletal maturity. At that time, for the very symptomatic patient, the treatment of choice is intra-articular repair of the anterior cruciate ligament. If a skeletally immature patient continues to have instability despite rehabilitation and bracing, a modification of the femoral tunnel to the over-the-top position will not place the lateral femoral physis at risk for premature closure and deformity. A centrally placed tibial tunnel will minimize the risk of angular deformity and minimize limb-length discrepancy if physeal arrest occurs. Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358. McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484. Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Question 6
Figures 14a and 14b show the initial radiographs of an 18-year-old man who fell while snowboarding. Figures 14c and 14d show the radiographs obtained following closed reduction. Examination reveals that the elbow is stable with range of motion. Management should now consist of




Explanation
The initial radiographs reveal a simple elbow dislocation without associated fractures. After successful closed reduction, the range of stability should be assessed. If the elbow is stable, nonsurgical management should consist of a short period of immobilization followed by range-of-motion exercises. Immobilization for more than 3 weeks results in significant elbow stiffness. Surgical repair is indicated for dislocations that are irreducible, have associated fractures, or where stability cannot be maintained with closed treatment. Cohen MS, Hastings H II: Acute elbow dislocations: Evaluation and management. J Am Acad Orthop Surg 1998;6:15-23.
Question 7
A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of


Explanation
The patient has a high-energy injury with resultant comminution of the distal radius metaphysis. Cast immobilization is likely to lead to radial shortening and angulation due to the comminution. Similarly, while external fixation and pinning has been successful in the past, some loss of radial length and volar angulation is typically noted. Present plate fixation devices for the distal radius employing locking screw technology have a superior ability to resist radial shortening and dorsal angulation. Fixation of the ulnar styloid is warranted when there is distal radioulnar joint instability or significant displacement of the styloid. This is more likely to occur with a fracture at the base of the styloid. In this instance, the distal radioulnar joint does not appear to be disrupted. May MM, Lawton JN, Blazar PE: Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27:965-971.
Question 8
The palmar cutaneous branch of the median nerve (PCBMN) originates from the
Explanation
The PCBMN originates from the median nerve proper between 3 and 21 cm proximal to the wrist with moderate variation. It virtually always originates from the radial side of the nerve and travels distally with the median nerve, radial to the palmaris longus, and ulnar to the flexor carpi radialis. Hobbs RA, Magnussen PA, Tonkin MA: Palmar cutaneous branch of the median nerve. J Hand Surg Am 1990;15:38-43.
Question 9
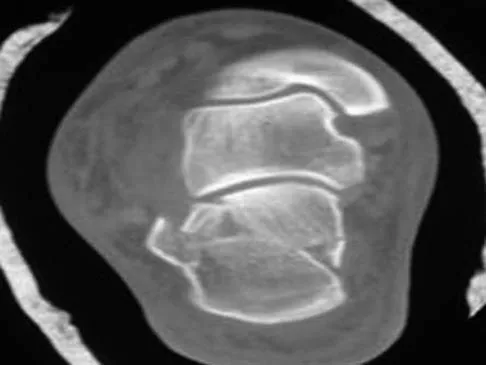
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?

Explanation
If the atlanto-dens interval is greater than 3 mm in an adult, a transverse ligament rupture usually is suspected. The atlanto-dens interval can be seen with CT or in lateral radiographs of the upper cervical spine. Transverse ligament rupture can occur as an isolated entity or in association with an odontoid or a Jefferson's fracture. Patients with this type of injury usually require fusion. Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
Question 10
A 58-year-old man has had a 3-year history of recurrent ulcerations of the left ankle and instability despite multiple attempts at custom bracing, contact casting, and surgical debridement. He has an ankle-brachial index of 0.76. A clinical photograph and radiographs are shown in Figures 16a through 16c. Treatment should now consist of



Explanation
Nonsurgical management has failed to provide relief; therefore, the treatment of choice is arthrodesis with an intramedullary nail. Amputation may be indicated if the arthrodesis fails. The patient does have adequate circulation for an attempt at salvage. Total ankle arthroplasty is not indicated in a neuropathic patient. Pinzur MS, Kelikian A: Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 1997;18:699-704.
Question 11
Mutations of what gene are associated with the subsequent development of osteosarcoma?
Explanation
Patients with a mutation of the retinoblastoma gene (RB) have an increased likelihood for the development of osteosarcoma. The EWS-FLI1 gene is the fusion product of a chromosomal translocation of 11:22. EGF-R and IGF-R are growth factor receptors, but mutations in these genes have not been correlated with osteosarcoma. VEGF is a proangiogenic molecule that is involved in tumor formation in multiple sites but not the development of osteosarcoma. Scholz RB, Kabisch H, Delling G, et al: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;7:265-273.
Question 12
Polyethylene wear of the bearing surface has been recognized as a mode of failure in total knee arthroplasty; therefore, many patients are offered polyethylene exchange. In terms of success rates, this surgical procedure has been reported to have a
Explanation
Engh and associates reported on the results of 63 knees (56 patients) following polyethylene exchange. The mean interval between exchange and the index total knee arthroplasty was 59 months. The mean follow-up after exchange was 7.4 years. Seven of 48 knees with adequate follow-up failed. Greater failure occurred if there was more severe wear before the exchange. Greater undersurface wear also resulted in a higher failure rate. Perioperative osteolysis or intraoperative observation of metallosis did not have an impact on the failure of polyethylene exchange. The risk of infection is no different from other total knee arthroplasty revisions. Wasielewski RC, Parks N, Williams I, et al: Tibial insert undersurface as a contributing source of polyethylene wear debris. Clin Orthop 1997;345:53-59.
Question 13
A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?




Explanation
The patient has osteonecrosis of the humeral head. The radiographs show increased density in the superior subchondral region of the humeral head. The MRI scans reveal a central collapse of the humeral head. The patient's history of severe asthma and long-term prednisone use predisposes her to this condition. The MRI scans show no evidence of a full- or partial-thickness rotator cuff tear. Without a history of fevers, chills, or other systemic signs or symptoms, there is no indication of septic arthritis. The radiographs do not reveal periarticular erosions, commonly seen in rheumatoid arthritis. Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 871-874.
Question 14
Which of the following diagnostic studies best distinguishes Ewing's sarcoma from small cell osteosarcoma?

Explanation
Cytogenetics best demonstrates the 11;22 translocation characteristic of Ewing's sarcoma. The translocation also can be detected with polymerase chain reaction and fluorescent in situ hybridization. The Ewing antibody is used for immunostaining to check for cell membrane (surface) staining of a marker unrelated to the translocation; this could also help distinguish Ewing's sarcoma from small cell osteosarcoma. A bone scan will show increased uptake with both types of tumors. Although most Ewing's sarcoma tumors are diploid, some are polyploid as are most osteosarcomas. Flow cytometry is used to sort cells, sometimes based on antibody binding. LDH can be elevated in both Ewing's sarcoma and osteosarcoma and is a poor prognostic indicator when elevated. Lymph node metastases are uncommon in both of these tumors. Perotti D, Corletto V, Giardini R, Parafioriti A, Fossati-Bellani F, Luksch R: Retrospective analysis of ploidy in primary osseous and extraosseous Ewing family tumors in children. Tumori 1998;84:493-498. Riley RD, Burchill SA, Abrams KR, Heney D, Sutton AJ, Jones DR, et al: A systematic review of molecular and biological markers in tumours of the Ewing's sarcoma family. Eur J Cancer 2003;39:19-30.
Question 15
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?

Explanation
The patient has a large zone of osteonecrosis of the left femoral head. The wedge-shaped zone of decreased signal intensity on the T1 image in the subchondral region of the femoral head is typical. Based on these findings, total hip arthroplasty is the most appropriate treatment. Open reduction and internal fixation will not help this condition. Incisional biopsy is indicated only if the MRI scan shows a probable neoplasm. Resection of the proximal femur is indicated only for aggressive malignancy. Arthrodesis may be considered in a younger patient but not in a 68-year-old individual. Other treatments, not listed, such as core decompression, vascularized fibular transplant, and osteotomy may be options in selected patients. Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.
Question 16
A 13-year-old girl has had pain in her ankle and difficulty with sporting activities for the past 6 months. Nonsteroidal anti-inflammatory drugs and use of a short leg cast have provided minimal relief. A radiograph and MRI scan are shown in Figures 43a and 43b. What is the next most appropriate step in treatment?


Explanation
The MRI scan shows an obvious talocalcaneal coalition of the medial facet. Because nonsurgical management has failed, surgical resection of the coalition is indicated. Arthrodesis would be indicated only if resection fails to relieve pain or if advanced degeneration of the hindfoot joints is present. McCormack TJ, Olney B, Asher M: Talocalcaneal coalition resection: A 10-year follow-up. J Pediatr Orthop 1997;17:13-15.
Question 17
High Yield
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

Explanation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744. Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 18
A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?

Explanation
Cervical myelopathy involves compression of the spinal cord and presents as an upper motor neuron disorder. Patients commonly have extremity spasticity and problems with ambulation and balance. Hoffman's sign is often present and is elicited by suddenly extending the distal interphalangeal joint of the middle finger; reflexive finger flexion represents a positive finding. The extremities are usually hyperreflexic with myelopathy. With cervical radiculopathy (lower motor neuron disorder), reflexes are hyporeflexic, and patients report pain along a dermatomal distribution. A hyperactive jaw jerk reflex indicates pathology above the foramen magnum or in some cases, systemic disease. Flaccid paraparesis suggests a lower motor neuron problem. Sachs BL: Differential diagnosis of neck pain, arm pain and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 741-742.
Question 19
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of

Explanation
The patient has a classic history and examination for an acute compartment syndrome of the foot. CT, MRI, or stress radiographs are not necessary prior to emergent fasciotomies of the foot. These studies can be performed after the initial fasciotomies to determine the best long-term management of the fractures. There are nine compartments in the foot. These are decompressed through three incisions (two on the dorsal foot and one medially). A short leg cast does not address the compartment syndrome and could be limb threatening with excessive swelling in a circumferential cast. It is preferable to splint severe crush injuries rather than apply a cast. Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Question 20
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management?



Explanation
The history, examination, and MRI scan findings are consistent with a midsubstance partial rupture of the rectus femoris muscle. This is an injury masquerading as a "pseudo tumor." The lack of an appreciable mass effect on the T1-weighted MRI scan, the defined fluid signal on the T2-weighted scans, and the lack of significant contrast enhancement after gadolinium are all most consistent with injury rather than a neoplasm. Most of these injuries respond to nonsurgical management; a few will benefit from late debridement and repair if symptoms fail to resolve in 3 to 6 months. The treatment of choice is nonsurgical management with a follow-up MRI scan to verify that the findings are resolving. Hughes C IV, Hasselman CT, Best TM, et al: Incomplete, intrasubstance strain injuries of the rectus femoris muscle. Am J Sports Med 1995;23:500-506.
Question 21
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?

Explanation
In a normal knee, the hard subchondral bone helps to distribute loads across the joint surface. A metal-backed tibial component in total knee arthroplasty decreases the compressive stresses on the underlying, softer cancellous bone by distributing the load over a larger surface area, particularly when one condyle is loaded. Although metallic base plates also increase the tensile forces on the other condyle when one is loaded and may decrease the thickness of the polyethylene tray, these are not benefits. Compressive forces on the polyethylene tray are increased with metal backing. The conformity of the articular surfaces is not affected by metal backing of the tibial component.
Question 22
Figure 2 shows the AP radiograph of an 18-year-old woman with progressive and severe right hip pain. Nonsteroidal anti-inflammatory drugs no longer control her pain. What is the next most appropriate step in management?

Explanation
A concentric hip with acetabular dysplasia in a symptomatic patient is best treated by periacetabular osteotomy. The Salter osteotomy is less optimal because the method has limited correction, is uniaxial, cannot be tailored to the deformity, and lateralizes the entire hip joint, thereby increasing the joint reactive forces. Because the hyaline cartilage of the joint is histologically normal, rotating the hyaline cartilage into an optimal position is preferable to augmenting the acetabulum with a shelf or by Chiari osteotomy. Varus intertrochanteric osteotomy has no significant role in the treatment of acetabular dysplasia. Total hip arthroplasty may be required in the future but should not be the first choice.
Question 23
When converting the knee shown in Figure 20 to a total knee arthroplasty, satisfactory outcome can be expected in what percent of patients?

Explanation
Naranja and associates reviewed 37 knees (35 patients, with 28 women and 7 men) without any motion that were converted to total knee arthroplasties. After an average follow-up of 90 months, the patients lacked an average of 7 degrees of extension and had 62 degrees of flexion. Results showed a short-term complication rate of 24% (stiffness requiring manipulation, delayed wound healing, and recurrent hemarthrosis), a major complication rate of 35% (patellar tendon or tibial tubercle avulsion, persistent pain requiring arthrodesis, loosening, and joint stiffness requiring arthrotomy for excision of scar tissue), and an infection rate of 14%. The total complication rate was 57%. A satisfactory outcome (no pain and an unlimited ambulation distance) was obtained in only 10 patients (29%). There was no relationship between results and the angle at which the knee was ankylosed preoperatively. This study revealed that although success in reconstructing a previously ankylosed or arthrodesed knee is possible, the lack of consistent adequate motion and the complication rate may suggest that the surgeon reconsider the risks and benefits of this difficult procedure.
Question 24
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70 degrees of the right knee. The active arc of motion is from 70 degrees to 90 degrees, and the opposite knee has a flexion contracture of 10 degrees. Both hips are dislocated with flexion contractures of 10 degrees, passive hip motion is from 10 degrees to 90 degrees of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
Most children with amyoplasia are ambulatory and when a decrease in function occurs because of a severe contracture, it must be addressed. A radical posterior soft-tissue release, including the posterior knee capsule and often the collateral ligaments and the posterior cruciate ligament, is needed to obtain extension. After the age of 1 year, aggressive physical therapy will do little to correct a contracture. Botulinum toxin A is indicated for spasticity and is contraindicated with severe contractures. Supracondylar femoral extension osteotomy works well, but will remodel at an average rate of 1 degree per month, which is not considered ideal in a young patient. Gradual correction with a circular ring external fixator is an option, but a soft-tissue release will also most likely be needed for a contracture of this severity. Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469. DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Question 25
Which of the following methods most reliably detects mechanical loosening of the hip?
Explanation
Mechanical loosening of the hip is best revealed by serial radiographs of the prosthetic joint. None of the other methods of evaluation is considered reliable in diagnosing mechanical loosening. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Question 26
A 36-year-old man has a moderate-sized left paracentral L5-S1 disk herniation with compression of the S1 nerve. Examination will most likely reveal sensory changes at what location?
Explanation
Because the left paracentral L5-S1 disk herniation is compressing the left S1 nerve root, the patient will have numbness along the lateral border and plantar surface of the foot. Numbness along the anterior thigh stopping at the knee is consistent with an L3 radiculopathy. Sensory changes at the dorsum of the foot and great toe normally signify an L5 distribution; the medial leg signifies an L4 distribution. Perianal numbness involves the S2-S5 nerve roots. Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman and Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, vol 1, pp 629-634.
Question 27
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?

Explanation
Glomus tumors are rare vascular lesions typically occurring about the nail of the distal phalanx of the hand. The diagnostic "triad" of glomus tumors consists of local pain, sensitivity to cold, and paroxysmal pain. They tend to present with pain as the most typical symptom and this can be exacerbated by changes in temperature that is felt to cause a vascular response within the lesion. The biopsy specimen confirms a glomus tumor showing the typical vascular spaces surrounded by glomus epithelioid glomus cells. Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
Question 28
Figure 20 shows the clinical photograph of a man who has had diabetes mellitus controlled with oral medication for the past 10 years. He wears soft-soled shoes and only uses leather-soled shoes for important business meetings. Examination reveals palpable dorsalis pedis and posterior tibial pulses, although they are somewhat diminished. He is insensate to pressure with the Semmes-Weinstein 5.07 monofilament. The ulcer heals after treatment with a full contact cast. What is the best course of action at this time?

Explanation
The patient has not undergone a trial of foot-specific patient education and accommodative/therapeutic shoe wear. He must use therapeutic shoe wear at all times, as even the occasional use of pressure-concentrating shoe wear has a high likelihood of leading to the development of a diabetic foot ulcer. Pinzur MS, Kernan-Schroeder D, Emmanuele NV, et al: Development of a nurse-provided health system strategy for diabetic foot care. Foot Ank Int 2001;22:744-746. Pinzur MS, Shields N, Goelitz B, et al: American Orthopaedic Foot & Ankle Society shoe survey of diabetic patients. Foot & Ankle Int 1999;20:703-707.
Question 29
Collagen orientation is parallel to the joint surface in what articular cartilage zone?
Explanation
The collagen orientation changes from parallel in the superficial zone to a more random pattern in the middle zone and finally to perpendicular in the calcified zone. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 498-499.
Question 30
Figure 41 shows the MRI scan of a 39-year-old man who has severe left groin and anterior thigh pain. What is the most likely diagnosis?

Explanation
The MRI scan shows near complete involvement of the femoral head with bone marrow changes and some collapse of the necrotic segment. This is most suggestive of osteonecrosis.
Question 31
Metal-on-metal articulation has been reintroduced because of concern about polyethylene wear. This type of articulation is considered favorable because
Explanation
The improvements in metal-on-metal bearing surfaces come from the nonlinear wear rate and smaller particle size of the high carbon wrought material. Extremely low rates of wear have been demonstrated with high carbon metal-on-metal implants. There is no significant electrochemical effect of mating two like materials in vivo.
Question 32
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of




Explanation
Scapular body fractures in children are rare and are often associated with other injuries of the chest and thorax. Management is generally nonsurgical, unless the injury is open, and usually consists of support with a sling and gentle range-of-motion exercises to minimize shoulder stiffness. Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Question 33
A 60-year-old woman with rheumatoid arthritis has atlanto-axial instability and basilar invagination. What MRI findings would suggest the need for cervical fusion?
Explanation
The cervical medullary junction should be 135 degrees or greater. An angle of 125 degrees suggests compression of the cervical medullary junction. Other findings supporting surgical intervention include a cord diameter in flexion of less than 6 mm or less than 13 mm of space available for the cord. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 700-701. Monsey RB: Rheumatoid arthritis of the cervical spine. J Am Acad Orthop Surg 1997;5:240-248.
Question 34
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?


Explanation
Osteolysis in the trochanteric bed can result in weakening of the bone and fracture. Nonsurgical management will provide reasonable clinical and radiographic results in patients with limited fracture displacement. Claus MC, Hopper RH, Engh CA: Fractures of the greater trochanter induced by osteolysis with the anatomic medullary locking prosthesis. J Arthroplasty 2002;17:706-712.
Question 35
The posterior approach to the proximal radius uses what intermuscular interval?

Explanation
Knowledge of intermuscular and internervous planes allows safe exposures throughout the body. The posterior (Thompson) approach to the proximal forearm uses the interval between the extensor carpi radialis brevis and extensor digitorum communis. The anterior (Henry) approach to the proximal forearm uses the interval between the brachioradialis and the flexor carpi radialis. Spinner M: Injuries to the Major Branches of Peripheral Nerves of the Forearm, ed 2. Philadelphia, PA, WB Saunders, 1978, pp 66-77.
Question 36
Figure 16 shows the clinical photograph of a 3-month-old infant with a foot deformity that has been nonprogressive since birth. Examination reveals that the deformity corrects actively and with passive manipulation. There is no associated equinus. Management should consist of

Explanation
The patient has bilateral metatarsus adductus deformities. In a long-term follow-up study by Farsetti and associates, deformities that were passively correctable spontaneously resolved and no treatment was required. More rigid deformities were successfully treated with serial manipulation, with good results in 90%. There were no poor results. Therefore, observation is the management of choice for passively correctable deformities. In feet that are more rigid, serial manipulation and casting is the management of choice.
Question 37
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?

Explanation
Distraction interposition arthroplasty is indicated for the treatment of both rheumatoid and posttraumatic arthritis and is reserved for younger patients who are not suitable candidates for total elbow arthroplasty. Although less reliable than prosthetic replacement, distraction interposition arthroplasty is a useful option in the treatment of young, high-demand patients with elbow arthritis. It is rarely indicated in the presence of polyarticular inflammatory arthritis but may be of value in those patients in whom the disease is limited primarily to the elbow. Isolated radiocapitellar arthritis can be successfully treated with radial head resection, although caution should be exercised if there is evidence of instability. Osteoarthritis is best treated with ulnohumeral arthroplasty. Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 38
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?


Explanation
Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 39
A 4-year-old boy with arthrogryposis has little active motion of his knees or elbows. Both elbows are in full extension with good triceps strength, but he is unable to bring his hand to his face or feed himself. Management should consist of
Explanation
Elbow release and triceps transfer to restore motion can be performed in children who are age 4 years and older. The ability to flex the elbow either actively or passively is of great assistance in activities of daily living. Van Heest A, Waters PM, Simmons BP: Surgical treatment of arthrogrypsosis of the elbow. J Hand Surg Am 1998;23:1063-1070.
Question 40
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?

Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve. Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Question 41
Figure 41a shows the AP radiograph of a 15-year-old boy who reports lateral knee pain. Figures 41b and 41c show a radiograph of the distal femur that was obtained 5 years ago and a current CT scan. The indication for surgery in this patient would be



Explanation
In a young person with solitary osteochondroma, the best surgical indication is symptoms that limit activity. A growth deformity is unlikely to occur at this age. Malignant degeneration is exceptionally rare and noted most commonly in adults. Growth is expected until skeletal maturity. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1626-1659.
Question 42
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Prior to transport, the face mask should be removed so that the airway can be easily accessible. If serious injury is suspected, the helmet and shoulder pads should be left in place until he is assessed at the hospital and radiographs are obtained. Leaving the helmet and shoulder pads in place helps to keep the spine in the most neutral alignment. Removal of the helmet will result in extension of the neck, whereas removal of the shoulder pads will most likely result in flexion of the neck. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347. Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med 2001;11:82-86. Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Question 43
A study is designed that examines fractures in children with osteogenesis imperfecta after being treated with bisphosphonates compared with a placebo. A difference is found for which the P value is greater than what is considered to be statistically significant. What is the next appropriate statistical analysis?
Explanation
When a study yields a negative result between treatment groups, the next step is to perform a power analysis. The power, by definition, is the probability of rejecting the null hypothesis: in this example the null hypothesis would be that children treated with bisphosphonates would have fewer fractures than the untreated control population. The power analysis helps answer the question as to whether the null hypothesis should be rejected and the finding is real, or whether the sample size was too small or the effect of treatment too subtle to demonstrate a difference between the treatment and control groups. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 7.
Question 44
A 7-year-old girl has had a painful forearm for the past 2 months. Examination reveals fullness on the volar aspect of the forearm. Radiographs and an MRI scan are shown in Figures 42a through 42c. Biopsy specimens are shown in Figures 42d and 42e. What is the most likely diagnosis?





Explanation
The radiographs reveal phleboliths on the volar side of the forearm consistent with hemangioma. The MRI scan reveals a rather well-circumscribed in size, irregular in shape, intramuscular soft-tissue mass in the volar aspect of the distal right forearm within the flexor group musculature. The mass demonstrates heterogeneous mixed signal intensity in both T1- and T2-weighted sequences with increased signal intensity on the T1, suggesting fat within the tumor, typical of hemangioma. The postgadolinium-enhanced sequences demonstrate heterogeneous enhancement. The MRI findings are consistent with a soft-tissue hemangioma. Garzon M: Hemangiomas: Update on classification, clinical presentation and associate anomalies. Cutis 2000;66:325-328.
Question 45
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the

Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235. Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Question 46
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?

Explanation
Despite the relatively few problems with porous-coated cementless stems, stress shielding and thigh pain do occur. One design feature of proximally coated stems that has been associated with a higher incidence of distal osteolysis is the presence of noncircumferential proximal porous coating. Tapered, modular with sleeve, and hydroxyapatite proximally porous-coated stems have all performed well. Fully porous-coated straight stems have a high survivorship rate as well. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 47
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of

Explanation
The radiograph reveals an atrophic nonunion of the diaphysis of the clavicle. Electrical or ultrasound stimulation may be an option in diaphyseal nonunions that have shown some healing response with callus formation, but these techniques are not successful in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions of the clavicle. Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Question 48
A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is the most likely diagnosis?


Explanation
Posterior ankle impingement or os trigonum syndrome is well described in dancers, and it is often associated with flexor hallucis longus tendinitis. High-quality MRI imaging will reveal the inflammation about the os trigonum and flexor hallucis longus tendinitis. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont IL, American Academy of Orthopaedic Surgeons, 1998, pp 315-332.
Question 49
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?



Explanation
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function. Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Question 50
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury. Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Question 51
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
The enthusiasm with which dorsal rhizotomy was received led to the broadening of selection criteria with poorer results. The ideal candidate is an ambulatory 4- to 8-year-old child with spastic diplegia who does not use assistive devices or have joint contractures. The child must be old enough to actively participate in the rigorous postoperative physical therapy program. The use of the procedure in an ambulatory 16-year-old patient is less desirable because joint contractures will most likely have developed to a varying degree. The hemiplegic child is best treated by orthopaedic interventions. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29. Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Question 52
A 45-year-old man who sustains a medial subtalar dislocation while playing basketball undergoes immediate closed reduction. No fractures or osteochondral defects are noted on postreduction radiographs. The next most appropriate step in management should consist of

Explanation
Most subtalar dislocations can be easily reduced by closed methods. If no fractures or defects are seen on the postreduction radiographs, then the success rate with cast immobilization is good. Medial dislocations have a better prognosis than lateral dislocations. Late instability is rare; therefore, the duration of immobilization should not be excessive. Most subtalar dislocations result in some stiffening of the hindfoot, and painful degenerative arthrosis is the most common serious complication.
Question 53
A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
Explanation
Following any closed fracture, the most important determinant for the timing of surgery is the condition of the soft tissues and especially the skin. The best determinant of appropriate soft-tissue condition is the presence of wrinkling of the skin (wrinkle sign) at the site of the incision. A wrinkle sign is present when all the interstitial edema has left the skin; this may take up to 14 to 21 days of elevation. Any abrasion must be epithelialized so that there are no bacteria left at the site. To date, no other method of soft-tissue viability measurement has been shown to be of any clinical benefit. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Question 54
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?





Explanation
The radiographs and CT scans show a displaced intra-articular calcaneal fracture, with loss of calcaneal height and length. Recent multicenter, randomized, prospective studies suggest that surgical treatment of displaced intra-articular calcaneal fractures is associated with an almost six-fold decrease in the risk of posttraumatic subtalar arthritis (necessitating subtalar arthrodesis) compared to nonsurgical treatment. Despite ongoing controversy, surgical treatment has not been shown to be advantageous with respect to activity, time to return to work, or subtalar joint range of motion. A nonunion of a calcaneal fracture is exceedingly rare regardless of the treatment method. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 55
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?

Explanation
The patient has nonunions of the metatarsal fractures and a hallux valgus deformity with arthritic changes. To address all of the findings, management should consist of open treatment of the metatarsal nonunions and hallux metatarsophalangeal arthrodesis. Cast immobilization and a bone stimulator are unlikely to be beneficial at this time. Isolated correction of the hallux valgus deformity will not address the metatarsal nonunions or the arthritis at the hallux metatarsophalangeal joint. Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214. McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Question 56
A 74-year-old man has had worsening left shoulder pain for the past 3 years. Extensive nonsurgical management has provided only minimal relief. Examination reveals limitations in motion due to pain but good rotator cuff strength. Radiographs are shown in Figures 53a and 53b. What surgical procedure is most appropriate?


Explanation
The patient has end-stage shoulder arthritis with posterior glenoid erosion and large humeral osteophyte formation. Since the rotator cuff is likely intact, the reverse total shoulder arthroplasty is unnecessary. All the remaining procedures may provide symptomatic relief in appropriate patients; however, for most patients, total shoulder arthroplasty has been associated with the most predictive pain relief and functional improvements. Bryant D, Litchfield R, Sandow M, et al: A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder: A systemic review and meta-analysis. J Bone Joint Surg Am 2005;87:1947-1956. Edwards TB, Kadakia NR, Boulahia A, et al: A comparison of hemiarthroplasty and total shoulder arthroplasty in the treatment of primary glenohumeral osteoarthritis: Results of a multicenter study. J Shoulder Elbow Surg 2003;12:207-213.
Question 57
What is the most likely late complication associated with cementless total knee replacement?
Explanation
In cementless total knee replacement, the risk of osteolysis is 30% if both components are placed without cement and screws are used for tibial fixation. The risk is 10% when a cemented tibial component is used, and the risk is 0% when both components are cemented. Loss of motion, patellofemoral pain, heterotopic bone formation, and patellar clunk are complications that can occur after cemented or cementless components are placed.
Question 58
Examination of a 45-year-old man with Charcot-Marie-Tooth disease reveals a cavus foot, a tight Achilles tendon, and forefoot callus formation. Radiographs reveal advanced degenerative changes in the hindfoot. Shoe wear modifications have failed to provide relief. Treatment should now consist of

Explanation
The patient has the typical end stage residuals from long-standing Charcot-Marie-Tooth disease. Initial management consisting of shoe wear modifications and orthotic devices is preferred, but these are not successful when the disease process has progressed. Surgical correction with calcaneal osteotomy or Achilles tendon lengthening and Steindler stripping is not indicated in the presence of significant hindfoot arthritis. Because this patient has findings consistent with hindfoot arthritis, a triple arthrodesis with correction of the cavus deformity is the preferred treatment. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth disease. J Bone Joint Surg Br 1989;71:17-20.
Question 59
A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of


Explanation
The patient has an isolated closed injury involving the humeral diaphysis. The lack of wrist and finger extension indicates injury to the radial nerve. Based on these findings, ongoing observation of the nerve is warranted with delayed exploration after 3 to 4 months if there are no signs of progressive return of nerve function. Treatment of the fracture should include external immobilization and fracture bracing. An indication for nerve exploration and surgical stabilization would be an open fracture. Zuckerman JD, Kovil KJ: Fractures of the shaft of the humerus, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1025-1053.
Question 60
Subluxation caused by rheumatoid arthritis is most commonly seen at what level of the cervical spine?

Explanation
Approximately 65% of cervical subluxations occur at C1-C2. Of these, 50% are anterior, with the remainder being lateral and posterior. The second most common type is basilar invagination, occurring in 40% of patients. The third most common type is subaxial, occurring in 20% of patients with rheumatoid arthritis. Subluxation at more than one level is common. Boden S, Clark CR: Rheumatoid arthritis of the cervical spine, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 693. Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 61
A patient with a 5-cm synovial sarcoma located in the distal portion of the rectus femoris muscle undergoes excision of the mass. The procedure is performed through a 10-cm longitudinal incision. Only a portion of the rectus femoris is removed; the vast majority of the muscle is preserved. The plane of dissection is beyond the reactive zone, and the pathology reveals that the margins are negative. This procedure is classified as

Explanation
The patient underwent a wide resection, which involves excision of the tumor along with a cuff of normal tissue that completely surrounds the tumor. The plane of resection is beyond the reactive zone. A radical resection involves removal of the entire affected muscle from origin to insertion. In a marginal excision, the plane of dissection is through the reactive zone of the tumor. A marginal excision is generally considered inadequate surgery for high-grade sarcomas. In an intralesional resection, the plane of dissection is through the tumor. Excision within the reactive zone but beyond the tumor is the same as a marginal excision. Enneking WF: Staging of musculoskeletal neoplasms, in Current Concepts of Diagnosis and Treatment of Bone and Soft Tissue Tumors. Heidelberg, Germany, Springer-Verlag, 1984.
Question 62
Decreased activity of which of the following proteins may be predictive of an aggressive soft-tissue sarcoma?
Explanation
It has been proposed that an imbalance in the proteolytic cascade involving matrix metalloproteinases (MMPs) and their inhibitors (TIMPs) may play a role in the development or progression of malignancy. TIMP activity has been shown to be weak or nonexistent and MMP activity to be high in patients with soft-tissue sarcoma. The level of vascular endothelial growth factor is shown to be a negative prognostic indicator because the expression of this factor is associated with angiogenesis and aggressive growth of many tumors including Ewing' s sarcoma and chondrosarcoma. Stromelysin is a type of MMP. The biology of cytokines in malignancy is complex. A low level of interleukin-1 is not known to be associated with high-grade tumors.
Question 63
A 16-year-old boy has had a painful ingrown nail on his great toe for the past 3 months. When initial management consisting of soaking the foot in Epsom salts and trimming the nail failed to provide relief, his family physician recommended 2 weeks of oral antibiotics. His symptoms persist, and he is now seeking a second opinion. A clinical photograph is shown in Figure 18. Management should now consist of

Explanation
The patient has a chronic ingrown nail on his great toe, which is not an uncommon occurrence in teenagers because of improper nail care. There is local infection and a foreign body reaction because of the nail. Continued conservative management with soaks and antibiotics will not improve the clinical situation. In the presence of local chronic infection, nail matrix ablation is contraindicated. Additionally, in the absence of a history of an ingrown nail, a nail matrix ablation is not medically indicated. The appropriate treatment is partial removal of the nail plate. With nail plate removal, the inflammation and local infection will resolve rapidly. Pettine KA, Cofield RH, Johnson KA, Bussey RM: Ingrown toenail: Results of surgical treatment. Foot Ankle 1988;9:130-134.
Question 64
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of

Explanation
An exercise program to strengthen the deltoid and remaining rotator cuff will most likely offer the best results. Revision rotator cuff surgery yields better results in decreasing pain than improving strength and function, and this patient has only minimal pain. Tendon transfers, involving the use of the latissimus dorsi or teres major, have been used when the rotator cuff is deemed irreparable but are not indicated in elderly patients with minimal symptoms. Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515. DeOrio JK, Cofield RH: Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
Question 65
In children with isolated zone II lacerations of the flexor tendon, poor digital motion is best correlated with
Explanation
In a recent study on restoration of motion following zone I and zone II flexor tendon repairs in children, age was found to have no effect on the results of zone II tendon repairs. Early passive motion offered no better results than immobilization for 3 weeks. Immobilization for more than 4 weeks correlated with poorer results.
Question 66
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?

Explanation
Simple removal of the loose glenoid component or removal of the loose component followed by implantation of a new glenoid component are both appropriate treatment choices, depending on the remaining glenoid bone stock. However, removal and reimplantation appears to provide the most predictable pain relief and better function than removal alone. Antuna SA, Sperling JW, Cofield RH, et al: Glenoid revision surgery after total shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-224.
Question 67
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?

Explanation
The radiograph reveals an increased first-second intermetatarsal angle and a congruent metatarsophalangeal joint with an abnormal distal metatarsal articular angle. Correction of both of these abnormalities requires a proximal and distal first metatarsal osteotomy. Coughlin M: Juvenile bunions, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 297-339.
Question 68
Which of the following types of ultra-high molecular weight polyethylene has been associated with the poorest clinical performance?
Explanation
Numerous studies have documented the poor performance of heat-pressed ultra-high molecular weight polyethylene used in the porous-coated anatomic tibial inserts of both total knee and unicompartmental arthroplasty. The other processing and sterilization methods have not been associated with significantly high failure rates. Wright TM, Rimnac CM, Stulberg SD, et al: Wear of polyethylene in total joint replacements: Observations from retrieved PCA knee implants. Clin Orthop 1992;276:126-134. Landy MM, Walker PS: Wear of ultra-high molecular-weight polyethylene components of 90 retrieved knee prostheses. J Arthroplasty 1988;3:S73-S85.
Question 69
A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?


Explanation
Rheumatoid arthritis is sometimes associated with radiographic evidence of instability of the cervical spine. In a study by Grauer and associates, radiographs of the cervical spine of patients with rheumatoid arthritis who had undergone total joint arthroplasty over a 5-year period were retrospectively reviewed. Nearly one half of the patients had radiographic evidence of cervical instability on the basis of traditional measurements. While radiographic evidence of cervical instability was not infrequent in this population of patients who underwent total joint arthroplasty for rheumatoid arthritis, radiographic predictors of paralysis were much less common. MRI prior to surgery may also be a consideration if the radiographic appearance of the rotator cuff alters the consideration of surgical treatment. In a series of patients undergoing prosthetic arthroplasty for a variety of shoulder disorders, the presence of a rotator cuff tear has been shown to be associated with a less favorable outcome. Most often, the presence of a rotator cuff tear was associated with a diagnosis of rheumatoid or other inflammatory arthritis and the tears were large and generally irreparable. Some case series demonstrated a higher prevalence of loosening of the glenoid component in patients with a large rotator cuff tear associated with superior migration of the humeral head. However, obtaining an MRI scan of the shoulder is not considered the best response since failure to determine cervical instability may result in anesthetic death. Whereas MRI may be helpful in planning reconstruction, it would be a less important priority. Grauer JN, Tingstad EM, Rand N, et al: Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am 2004;86:1420-1424.
Question 70
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Although technically challenging, the Ganz periacetabular osteotomy offers advantages over other rotational pelvic osteotomies. Posterior column integrity is maintained, as is the acetabular vascular supply. Free mobility of the fragment makes large corrections in the center edge angle possible. Because of the asymmetric cuts and the need to restore anterior coverage, there is a tendency to anterior displacement of the joint while flexing the acetabulum. The procedure is commonly performed through a Smith-Petersen incision. Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 71
In children between the ages of 4 and 8 years, the major blood supply to the femoral head comes from the

Explanation
From birth until the age of 4 years, the primary blood supply to the femoral head is from the medial and lateral circumflex arteries that traverse the femoral neck. After the age of 4 years, the contribution of the lateral femoral circumflex artery, which traverses the anterior portion of the femoral neck, becomes negligible. The posterosuperior and posteroinferior retinacular vessels, branches of the medial femoral circumflex artery, become the primary blood supply to the epiphysis. The contribution of the artery of the ligamentum teres is minimal after the age of 4 years. Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
Question 72
Figure 5 shows the radiograph of a 10-year-old girl who reports chronic shoulder pain after her gymnastics classes. Examination reveals pain on internal and external rotation but no instability. What is the most likely diagnosis?

Explanation
The patient has a very wide humeral growth plate, indicating the presence of a proximal humeral stress fracture, an uncommon diagnosis in gymnasts. Gymnasts are prone to stress fractures of the scaphoid, distal radius, elbow, and clavicle. Proximal humeral stress fractures are more commonly seen in those participating in racket or throwing sports. Stress fractures can lead to growth arrest or inhibition, particularly in the distal radius. The radiograph shows normal findings for the acromion, acromioclavicular joint, scapula, and triceps origin. Fallon KE, Fricker PA: Stress fracture of the clavicle in a young female gymnast. Br J Sports Med 2001;35:448-449. Sinha AK, Kaeding CC, Wadley GM: Upper extremity stress fractures in athletes: Clinical features of 44 cases. Clin J Sports Med 1999;9:199-202. Caine D, Howe W, Ross W, Bergman G: Does repetitive physical loading inhibit radial growth in female gymnasts? Clin J Sports Med 1997;7:302-308.
Question 73
Which of the following tumors is most likely to present with a pathologic fracture in a child?

Explanation
In nearly 50% of patients with a unicameral bone cyst, the lesion remains asymptomatic until a fracture occurs, usually as the result of relatively minor trauma. If the lesion expands, the bone is weakened and may cause pain. Fibrous cortical defects are usually an incidental finding and typically asymptomatic. Malignant bone tumors such as osteosarcoma and Ewing's sarcoma most commonly cause pain, and pathologic fracture occurs in less than 10% of patients. Giant cell tumors are uncommon in children and usually are painful. Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224. Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Question 74
Figure 17 shows the radiograph of a 25-year-old professional football player who has superior shoulder pain that prevents him from sports participation. History reveals that he sustained a shoulder injury that was treated with closed reduction and temporary pinning 3 years ago. The best course of action should be

Explanation
The radiograph shows a complete acromioclavicular separation. Because the patient is a professional athlete who is unable to participate, surgery is indicated. Chronic separations, especially those with previous trauma from joint pinning, should be treated with resection of the distal clavicle and stabilization to the coracoid. Some type of biologic reconstruction of the coracoclavicular ligaments is generally recommended. Open repair of the ligaments is generally not possible in such a delayed fashion. Screw fixation alone will not provide a lasting solution as the screws usually need to be removed, leaving no fixation in place. Reconstruction using the coracoacromial ligament is generally recommended with coracoclavicular fixation to protect the repair while it heals. Nuber GW, Bowen MK: Disorders of the acromioclavicular joint: Pathophysiology, diagnosis and management, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999.
Question 75
A 45-year-old woman has had progressive right shoulder pain for the past 6 months. She notes that the pain disrupts her sleep, she has pain at rest that requires the use of narcotic analgesics, and she has limited use of her left shoulder for most activities of daily living. History reveals the use of corticosteroids for systemic lupus erythematosus. Examination shows diminished range of motion. Radiographs of the right shoulder are shown in Figures 4a and 4b. Treatment should consist of


Explanation
Humeral arthroplasty provides excellent pain relief and function for stage IV osteonecrosis with humeral collapse. In late disease with glenoid involvement (stage V), total shoulder arthroplasty is preferred. Some authors have reported satisfactory results with core decompression of the humeral head for early stages of osteonecrosis, but results for stage IV osteonecrosis are less satisfactory when compared with those for humeral arthroplasty. Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. LePorte DM, Mont MA, Mohan V, Pierre-Jacques H, Jones LC, Hungerford DS: Osteonecrosis of the humeral head treated by core decompression. Clin Orthop 1998;355:254-260.
Question 76
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of

Explanation
Loss of internal rotation is common among overhead throwers and tennis players. Posterior capsular stretching can improve symptoms when accompanied by rest and gradual resumption of throwing. To avoid a false impression of improvement, cortisone injection is not recommended. Pitching through pain can cause further damage to the labrum and capsule. A sling and external rotator strengthening will not improve internal rotation. Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Question 77
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?

Explanation
The risk of synostosis is imminent with any technique for repairing a distal biceps tendon rupture. However, the risk is quite low for all approaches that avoid exposure of the ulna, including the muscle-splitting two-incision technique.
Question 78
What is the dominant component of articular cartilage extracellular matrix by weight?

Explanation
Articular cartilage is a highly organized viscoelastic material, and load transmission depends on the specific composition of the extracellular matrix. Articular cartilage is devoid of neural, lymphatic, and blood vessel tissue. The extracellular matrix consists of water, proteoglycans, and collagen. Water comprises most of the wet weight (65% to 80%). Type II collagen comprises 95% of the collagen. The collagen and proteoglycan (keratan sulfate and chondroitin sulfate) matrix and its high water content are responsible for the mechanical properties of the articular cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Inst Course Lect 1998;47:487-504.
Question 79
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of


Explanation
The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 80
Figure 23 shows failure of the femoral stem in a patient. What is the most likely reason for the failure?

Explanation
A two-dimensional stress analysis has been used to study the effects of some of the factors leading to early fatigue failure of the femoral stem in total hip arthroplasty. It has been demonstrated that loss of proximal stem support at the level of the calcar femorale and subsequent stem stress can lead to fatigue failure. In addition, the role of body weight and range of cyclic stress fluctuation play an important role in fatigue life under conditions where the stem has lost proximal support. These results indicate that stem design could be improved by incorporating some means of adequate support at the calcar femorale where maximum tensile stresses are found to occur. Femoral component fracture is a rare but well-documented complication after total hip arthroplasty. Historically, most stem fractures occur at the middle third of the implant where proximal stem loosening and solid distal stem fixation result in cantilever bending and eventual fatigue failure. The component shown is a modular fluted cementless stem that occasionally fractures at the modular junction in patients with poor proximal bone support. Andriacchi TP, Galante JO, Belytschko TB, et al: A stress analysis of the femoral stem in total hip prostheses. J Bone Joint Surg Am 1976;58:618-624.
Question 81
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of


Explanation
The patient has a nonunion at the subtalar joint because of poor preparation of the arthrodesis site with incomplete removal of the articular cartilage. Clinically, he has arthritis at the transverse tarsal joint. Casting with a bone stimulator is not expected to result in a union of the subtalar arthrodesis. To address both the subtalar nonunion and the transverse tarsal joint arthritis, revision of the subtalar arthrodesis and conversion to a triple arthrodesis is the preferred option. Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362. Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499. Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307. Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
Question 82
What is the most common problem seen following epiphysiodesis for limb-length discrepancy?

Explanation
Errors in timing are by far the most common in this technically safe procedure. Incomplete growth arrest has been reported in up to 15% of patients versus timing errors in 61%. Fracture through the site has been reported rarely. Neurovascular and cartilaginous injury are extremely uncommon but always need to be considered when performing surgery in the vicinity of these structures. Blair VP III, Walker SJ, Sheridan JJ, Schoenecker PL: Epiphysiodesis: A problem of timing. J Pediatr Orthop 1982;2:281-284.
Question 83
Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
Explanation
In secondary amenorrhea, women do not receive the estrogen needed to maintain adequate bone mineralization. This hypoestrogenic state affects bone density, and there is evidence that stress fractures are more frequent in amenorrheic than eumenorrheic athletes. The other conditions are not seen with increased frequency in amenorrheic athletes. Warren MP: Health issues for women athletes: Exercise-induced amenorrhea. J Clin Endocrinol Metab 1999;84:1892-1896.
Question 84
What is the most likely type of pathology seen in Figure 16?

Explanation
The figure shows the missing pedicle or "winking owl" sign that is characteristic of tumor involvement of the cortical bone of the pedicle. None of the other pathologic processes commonly gives this radiographic picture. Thinned, but not missing pedicles, have been described as a normal variant. McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
Question 85
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5 degrees of angulation. When the MCP joint is flexed 30 degrees, a radially directed stress produces 45 degrees of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as "gamekeeper's thumb." The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness. Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Question 86
When compared with cobalt-chromium and stainless steel implants, a titanium implant has what biomechanical properties?

Explanation
Titanium implants are commonly used in spinal surgery, especially when MRI may be needed after implantation. Titanium implants have a lower modulus of elasticity when compared with cobalt-chromium and stainless steel implants. This is felt to allow less stress shielding for these types of implants. The other properties do not apply to titanium implants.
Question 87
Figure 11a shows the AP pelvis radiograph of a 25-year-old man who sustained a spinal cord injury 10 years ago. A bone scan and a CT scan are shown in Figures 11b and 11c. To prevent recurrence after resection, management should consist of



Explanation
The studies reveal significant heterotopic ossification that appears to be mature. Following resection, the most reliable way to prevent recurrence is with low-dose external-beam radiation therapy. Bisphosphonate therapy can be considered; however, when terminated, heterotopic bone may reform. Heterotopic ossification is unrelated to the patient's endocrine status and is not associated with any metabolic abnormalities. Moore K, Goss K, Anglen J: Indomethacin versus radiation therapy for prophylaxis against heterotopic ossification in acetabular fracture. J Bone Joint Surg Br 1998;80:259.
Question 88
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?

Explanation
The patient has a simple fracture pattern that can be reduced anatomically and stabilized with absolute stability by interfragmental compression and protection plating. This will guarantee a 95% to 98% union rate with no radial nerve palsy. Intramedullary nailing does not equal these results in a simple fracture pattern in the humerus. Bridge plating is indicated for multifragmented fracture patterns when anatomic reduction and absolute stability cannot be achieved. External fixation is reserved for severe open fractures. Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166. Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Question 89
A 40-year-old man has had hip pain with increased activity over the past year. Examination reveals restriction of motion and tenderness with combined hip flexion, adduction, and internal rotation. An AP radiograph is shown in Figure 34. What is the most likely diagnosis?

Explanation
Femoral acetabular impingement (FAI) is a pathologic entity leading to pain, reduced range of motion in flexion and internal rotation, and development of secondary arthritis of the hip. There are two types of FAI: cam impingement and pincher impingement. Cam impingement is seen when a nonspherical femoral head produces a cam effect when the prominent portion to the femoral head rotates into the joint. This mechanism produces shear forces that damage articular cartilage. Radiographs reveal early joint degeneration and flattening of the head neck junction (the so-called "pistol grip deformity") as seen in this image. The pincher type of impingement involves abnormal contact between the femoral head neck junction and the acetabulum, in the presence of a spherical femoral head. Beall DP, Sweet CF, Martin HD, et al: Imaging findings of femoraoacetabular impingement syndrome. Skeletal Radiol 2005;34:691-701.
Question 90
A 10-year-old boy reports a gradual onset of weakness; however, he is fully ambulatory. History reveals that he has a 17-year-old brother who has just stopped walking because of a similar condition. Laboratory studies show a creatine kinase level of 5,480 IU/L (normal 25 to 232 IU/L), and examination shows a slightly positive Gower sign. What is the most likely diagnosis?
Explanation
The patient has Becker muscular dystrophy. Patients with this condition have a slower rate of progression of disease compared with patients who have Duchenne muscular dystrophy, and walking may continue into the late teens. The creatine kinase level is not as high as in Duchenne muscular dystrophy, which can range from 20,000 to 30,000 IU/L. Becker muscular dystrophy is allelic to Duchenne muscular dystrophy, resulting in a mutation in the dystrophin gene. Myotonic dystrophy is characterized by a progressive inability to relax the muscles after contracture. The Gower sign is not helpful in this disease. Patients with Charcot-Marie-Tooth disease, one type of which is also known as HMSN type II, do not have elevated creatine kinase levels and usually present with a foot deformity. Spinal muscular atrophy, type II, usually presents with severe weakness in the second year of life. Matsuo M: From molecular diagnosis to gene therapy. Brain Dev 1996;18:167-172. Darras BT: Molecular genetics of Duchenne and Becker muscular dystrophy. J Pediatr 1990;117:1-15.
Question 91
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?

Explanation
This view from the lateral portal shows a full-thickness rotator cuff tear. The glenohumeral joint can be visualized through this tear. The glenoid, labrum, and biceps tendon attaching to the superior aspect of the glenoid are easily viewed from this portal, and the arrow is pointing to the biceps tendon. Arthroscopic rotator cuff repair can be performed while visualizing from this portal and using anterior and posterior working portals. Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Question 92
Figures 25a and 25b show the radiographs of a 66-year-old man who has had a long history of bilateral painful flatfoot deformities. Examination reveals that his foot is partially correctable passively, albeit with discomfort, and he has an Achilles tendon contracture. An ankle-foot orthosis has failed to provide relief. Treatment should now consist of


Explanation
The patient has a pronounced deformity with pain and degenerative arthritis; therefore, triple arthrodesis is the treatment of choice. Gastrocnemius or Achilles tendon lengthening may be a necessary adjunct to the triple arthrodesis, but alone is inadequate to allow for correction. Because the ankle-foot orthosis has failed to provide relief, a UCBL is not likely to help. Osteotomy procedures are designed for lesser deformities and well-preserved joints. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 115-120.
Question 93
What type of metastatic tumor most often has a lytic radiographic appearance?

Explanation
Lung carcinoma most often has a lytic radiographic appearance. Bladder and prostate carcinoma are usually blastic. Breast carcinoma can be both blastic and lytic. Thyroid carcinoma may be difficult to visualize radiographically and may be seen only on MRI scans. Metastatic osteosarcomas typically produce bone. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 94
A college basketball player is struck in the eye by a player's hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of

Explanation
The athlete has a corneal abrasion. Fluorescein staining identifies the break in the epithelium when examined with ultraviolet light. Topical antibiotics are used as prophylaxis against secondary bacterial infection, and the patch, applied with the lid closed, is used for comfort and to promote epithelial healing. The accompanying symptoms, including pain, tearing, and photophobia, are usually too intense to allow a return to play. Surgery is reserved for a corneal laceration with associated loss of the anterior chamber. While a proper fundoscopic examination may be a consideration, increased intraocular pressure is not typically associated with this injury. Traumatic hemorrhage in the anterior chamber (hyphema) necessitates strict bed rest during the early phases of healing; examination will most likely reveal the red fluid level of blood settling inferiorly in the anterior chamber. It is often associated with increased intraocular pressure. Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Question 95
A 52-year-old man underwent arthroscopic repair of a 1-cm supraspinatus tendon tear 3 weeks ago. He was doing well until he fell down three stairs. One week after the fall he continues to report pain similar to his preoperative pain. An MRI scan reveals a minimally retracted 1-cm supraspinatus tendon tear in the same location as his original tear. Management should now consist of

Explanation
The patient has retorn his rotator cuff repair. This traumatic retear is different from a chronic tear and should be treated similar to an acute rotator cuff tear. Because the patient is younger than age 65 and has a small, single tendon tear, a revision rotation cuff repair is indicated with an expected tendon healing rate of greater than 95%. A physical therapy program is not indicated, and further delay in repair compromises his functional recovery. A cortisone injection is not indicated for this repairable tendon tear. Immobilization will not allow the tendon to heal once it has retorn. A debridement procedure is not indicated on this repairable tendon tear; this procedure is indicated in painful, chronic, irreparable tendon tears. Boileau P, Brassart N, Watkinson DJ, et al: Arthroscopic repair of full-thickness tears of the supraspinatus: Does the tendon really heal? J Bone Joint Surg Am 2005;87:1229-1240. Jost B, Zumstein M, Pfirrmann CWA, et al: Long-term outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 2006;88:472-479.
Question 96
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
Afferent pain fibers to the lumbar facet joints arise from the medial branch nerves originating from the next two cephalad levels. Therefore, innervation of the L3-L4 facet joint arises from the L2 and L3 medial branch nerves. This effect should be taken into account when considering a medial branch block or facet denervation. The medial branch nerve arises from the dorsal ramus of the exiting nerve root. Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
Question 97
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?

Explanation
Combination drugs with activity against both aerobic and anaerobic organisms have been determined to be the best approach. The first-generation cephalosporins do not provide adequate coverage for gram-negative and anaerobic organisms. Gentamicin alone would not provide adequate activity against anaerobes, and there is the risk of renal and auditory toxicity. Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Question 98
The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?

Explanation
Although the original concept of internal fixation was one of anatomic reduction and stable fixation, over the past 10 to 15 years there has been a change based on the advent of intramedullary nailing and bridge plating. It is now appreciated that in a multifragmentary diaphyseal fracture, particularly of the lower extremity, the achievement of axis alignment (mechanical and anatomic axis) is all that is required. Healing will occur by callus. Relatively stable fixation is achieved through intramedullary nailing or bridge plating, providing adequate pain relief for functional aftercare. Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 7-32. deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Question 99
Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?

Explanation
Kramer and associates conducted a retrospective review during an "epidemic" period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound debridement, and an 11% rate of surgical site complications. Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.
Question 100
A 10-year-old girl has been unable to walk for the past 5 days because of bilateral hip pain. Administration of IV morphine has provided some pain relief. She is afebrile. History reveals that she had an upper respiratory tract infection 3 weeks ago that resolved uneventfully. Examination reveals moderate pain with internal rotation and abduction, while log rolling maneuvers do not cause significant pain. An MRI scan shows a small effusion of one hip; however, a bone scan and plain radiographs are normal. Initial laboratory studies showed a markedly elevated WBC count, which subsequently declined to normal levels with IV antibiotics. Current studies show an erythrocyte sedimentation rate (ESR) of 100 mm/h. Aspiration of the hip obtains 3 mL of fluid; Gram stain is negative for bacteria, but a cell count shows a WBC count of 16,500/mm3. Streptozyme titer of the peripheral blood is 200 units (normal is less than 100 units). Management should now consist of

Explanation
This clinical situation requires careful analysis because some data suggest infection and some a noninfectious inflammatory process. Bilateral hip involvement, the absence of significant fluid collection or fever, the streptozyme level, and the history of upper respiratory infection all suggest poststreptococcal toxic synovitis as the most likely cause for the clinical presentation. In the first 24 hours, this type of presentation might warrant incision and drainage given uncertainty of the diagnosis and the risks associated with missing an infection. However, 5 days after onset, surgery is not warranted, especially given that the patient remains afebrile and her symptoms are improving. Cardiology consultation would be appropriate. There is no evidence to suggest slipped capital femoral epiphysis. Treatment with antibiotics is not advised because there is no bacteriologic data on which to base treatment. De Cunto CL, Giannini EH, Fink CW, et al: Prognosis of children with poststreptococcal reactive arthritis. J Pediatr Infect Dis 1988;7:683-686.
