Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
For a pediatric patient without mechanical symptoms, initial management of an osteochondral defect lesion that is not detached should consist of casting in flexion. Failure to respond to several weeks or months of nonsurgical management may warrant surgical treatment.
Question 2
High Yield
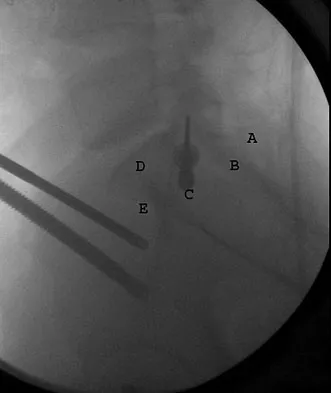
What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?
Explanation
Iliosacral screws cannot always be placed safely due to variations in pelvic anatomy. Transiliac bars are an alternative method for fixation but are placed using an open technique. A screw can be placed percutaneously through both iliac wings posterior to the posterior border of the sacrum. The starting point is visualized using a lateral C arm shot and is located on the posterior iliac crest at about the level of the S1 body where the crest has its largest area posterior to the sacrum. This area is labeled A in the figure, B represents the sacral canal, C is S1, D is the area cephalad to the iliocortical density, and E is the anterior border of the sacrum. The radiograph demonstrates a well-placed sacroiliac screw. Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: Cadaver feasibility study and preliminary clinical results. J Trauma 2007;62:357-364.
Question 3
A patient with rheumatoid arthritis with both ankle and subtalar involvement was treated as shown in Figures 11a and 11b. What complication is unique to this type of fixation?


Explanation
The interlocking screws at the proximal end of the rod can act as a stress riser and lead to fracture. Postoperative pain at this level should prompt inclusion of this diagnosis in the differential. Removing the screws following bone union can decrease the chances of this occurring. A short rod that avoids the diaphyseal area may also be beneficial. Rotatory deformity is controlled by the perpendicularly oriented distal transfixion screws. Talar osteonecrosis would be unusual since the dissection can be minimized with an intramedullary rod. Any type of hardware can fail if the construct does not lead to a solid arthrodesis. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 236-237. Thordarson DB, Chang D: Stress fractures and tibial cortical hypertrophy after tibiotalocalcaneal arthrodesis with an intramedullary nail. Foot Ankle Int 1999;20:497-500.
Question 4
A 25-year-old man has a mass on the medial aspect of the left knee. He reports that the mass has been present for several years, but a recent increase in physical activity has resulted in periodic tenderness. Radiographs are shown in Figures 13a and 13b. What is the most likely diagnosis?


Explanation
The radiographs reveal a sessile lesion projecting from the medial aspect of the distal femur. The lesion shares the cortex with the bone and the base communicates with the medullary space of the femur. This is the classic appearance of an osteochondroma, the most common benign tumor of bone. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 5
What is a common clinical finding in patients with severe hypercalcemia secondary to bony metastasis?
Explanation
Increased levels of calcium are known to cause anorexia, nausea, vomiting, dehydration, muscle weakness, polyuria, and polydipsia. Treatment may include hydration, saline diuresis, and bisphosphonates.
Question 6
Surgical treatment for symptomatic disk herniations is associated with which of the following?
Explanation
The recently published SPORT trial verifies that surgical treatment of symptomatic disk herniations is associated with early and sustained pain relief. The trial also verifies that nonsurgical management is associated with improved symptoms as well. Nerve root injury, recurrent herniation, and diskitis are known complications of surgery, but all are less common than described above.
Question 7
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as

Explanation
The incidence of osteolysis is minimal in studies reporting the use of all polyethylene or monolithic metal-backed tibial components. Osteolysis has been reported in patients with total knee arthroplasties using cementless implants with modular components. Micromotion between the tibial tray and the polyethylene results in backside wear, leading to osteolysis. Osteolysis also has been reported in cemented posterior cruciate-substituting modular components. O'Rourke and associates reported a 16% incidence of osteolysis in patients with a posterior stabilized implant because of the use of modular polyethylene and the subsequent abrasive wear. Oxidation of the polyethylene that is the result of the method of sterilization and shelf life has also been implicated in the high incidence of osteolysis, along with patient factors such as activity level and weight.
Question 8
Figures 49a and 49b show MRI scans of the shoulder. What is the most likely diagnosis?


Explanation
The supraspinatus tendon shows clear detachment and retraction from its greater tuberosity attachment by the absence of the normal dark subacromial signal extending to the attachment on the greater tuberosity. There is no anterior inferior glenoid labral detachment that usually is seen in a Bankart lesion. The acromioclavicular joint shows no evidence of separation. The humeral head is migrated cranially, indicating a chronic rotator cuff tear. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29. Seeger LL, Gold RH, Bassett LW, Ellman H: Shoulder impingement syndrome: MR findings in 53 shoulders. Am J Roentgenol 1988;150:343-347.
Question 9
Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?

Explanation
The peroneus brevis is easily identified by its location behind the fibula and its distal muscle belly. Axial MRI images provide a reliable guide even when one of the peroneals is completely ruptured, subluxated out of the peroneal groove, or absent. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, pp 234-235.
Question 10
A 15-year-old boy reports leg pain after being tackled during football practice. Radiographs and a CT scan are shown in Figures 46a through 46c. The patient has a pathologic fracture through what underlying lesion?



Explanation
The images show a lobulated, eccentric, well-marginated lesion that is typical of a nonossifying fibroma. The lesion is slightly expansile, and the CT scan findings show that the lesion is very well marginated and the cortex is disrupted, which is a common finding. None of the characteristics of this lesion is aggressive in nature. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 11
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?

Explanation
Internal impingement of the shoulder is a leading cause of shoulder pain in the throwing athlete. The primary lesion in pathologic internal impingement is excessive tightening of the posterior band of the inferior glenohumeral ligament complex. To obtain an accurate assessment of true glenohumeral rotation, the scapula is stabilized during examination. A loss of 20 degrees or more of internal rotation, as measured with the shoulder positioned in 90 degrees of abduction, indicates excessive tightness of the posterior band of the inferior glenohumeral ligament complex. Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Question 12
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Question 13
Which of the following is the primary mechanism of polyethylene wear in the hip?
Explanation
Although previous theories on acetabular wear implicated fatigue cracking and delamination as primary wear mechanisms, these have actually manifested as major modes of polyethylene wear in knees. The primary mechanism of wear in polyethylene acetabular components appears to be adhesion and abrasion. In an analysis of 128 components retrieved at autopsy or revision surgery, wear appeared to occur mostly at the surface of the components and was the result of large strain plastic deformation and orientation of the surface layers into fibrils that subsequently ruptured during multidirectional motion. It was also shown conclusively that 32-mm heads displayed significantly more wear (volumetric wear) than either 22-mm or 26-/28-mm heads (1-mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of polyethylene fibrils, and abrasion secondary to third-body wear. Wear rates decreased with longer survival of components, indicating a "bedding in" phenomenon, arguing against oxidative and fatigue wear. Crevice corrosion occurs in fatigue cracks with low oxygen tension (under screw heads, etc). Oscillatory fretting consists of cyclical abrading of the outer surface from small movements. Fatigue and delamination is predominant in total knee arthroplasty where stresses are maximum just below the surface of the polyethylene component, causing fatigue over time with subsequent delamination. In contrast, hip wear occurs primarily at the surface of the polyethylene component. Jasty M, Goetz DD, Bragdon CR, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53. Bell CJ, Walker PS, Abeysundera MR, et al: Effect of oxidation on delamination of ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty 1998;13:280-290.
Question 14
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?

Explanation
The patient's symptoms are typical for gouty arthropathy, and the diagnosis can only be confirmed with aspiration and visualization of the crystals. A concomitant infection also must be ruled out; therefore, it is important to obtain a cell count and culture. Colchicine may have a role in gouty management, but the diagnosis must be confirmed. Allopurinol is not effective in acute gouty arthropathy. Measurement of serum uric acid levels is often not helpful in making a definitive diagnosis. Steroid injections should be deferred until cell count and culture results indicate no accompanying infection. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Question 15
A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of


Explanation
The radiographs reveal a scaphoid fracture with displacement and comminution and an unstable fracture pattern. Treatment should consist of open reduction and internal fixation. In displaced scaphoid fractures and fractures with unstable fracture patterns, closed reduction is ineffective and is likely to lead to nonunion. Limited intercarpal fusion and proximal row carpectomy are used to correct a variety of traumatic and posttraumatic problems of the wrist. Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 809-823. Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276. Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
Question 16
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
The association of a nail puncture wound with a gram-negative infection (Pseudomonas aeruginosa) has been attributed to the local environmental factors in shoes. Osteomyelitis is rare, occurring only in about 1% of patients. Tetanus prophylaxis should be given if it is not up to date. While the remaining organisms listed are periodically involved, they are more common in patients who are immunocompromised or who have diabetes mellitus. Therefore, obtaining a culture of the infected wound is appropriate in such individuals because of the multifactorial nature of the infection. Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Question 17
The brachialis muscle is innervated by what two nerves?

Explanation
The brachialis is innervated by two nerves: medially, the musculocutaneous nerve; laterally, the radial nerve. The muscle is split longitudinally to approach the humerus anteriorly. Henry AK: The distal part of the humerus and front of the forearm, in Henry AK (ed): Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 90-115.
Question 18
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
The enthusiasm with which dorsal rhizotomy was received led to the broadening of selection criteria with poorer results. The ideal candidate is an ambulatory 4- to 8-year-old child with spastic diplegia who does not use assistive devices or have joint contractures. The child must be old enough to actively participate in the rigorous postoperative physical therapy program. The use of the procedure in an ambulatory 16-year-old patient is less desirable because joint contractures will most likely have developed to a varying degree. The hemiplegic child is best treated by orthopaedic interventions. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29. Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Question 19
The radiograph shown in Figure 27 shows measurement of what angle?

Explanation
The relationship between the distal articular surface of the first metatarsal head and the long axis of the first metatarsal is called the distal metatarsal articular angle. This angle has been validated by Richardson and associates to measure and determine the congruence of the first metatarsophalangeal joint. This angle is critical in determining the appropriate surgical procedure to perform on a patient with a bunion deformity because a congruent joint requires a procedure to maintain congruence of the articular surfaces following osteotomy. Therefore, a chevron becomes a biplanar chevron, and a Lapidus procedure adds a second osteotomy of the distal metatarsal to tilt the metatarsal head into a congruent location. Coughlin MJ: Juvenile hallux valgus: Etiology and treatment. Foot Ankle Int 1995;16:682-697. Steel MW III, Johnson KA, DeWitz MA, et al: Radiographic measurements of the normal foot. Foot Ankle 1980;1:151-158.
Question 20
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?

Explanation
Radiation therapy is commonly used as an adjuvant in the treatment of soft-tissue sarcomas, but a controversy exists whether it should be preoperative or postoperative. Radiation therapy can be given prior to or following resection of the tumor. Postoperative radiation is usually given in a higher dose to a larger treatment field. This commonly results in a higher incidence of fibrosis and lymphedema. There is no statistical difference in local recurrence rate between the two radiation treatment plans. Neuropathy is more commonly a complication of chemotherapy. Preoperative radiation therapy has been shown to have a higher wound complication rate than postoperative radiation. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Question 21
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?

Explanation
The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 22
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
The term turf toe includes a range of injuries of the capsuloligamentous complex of the first metatarsophalangeal joint with or without osteochondral fracture of the first metatarsal head or one of the sesamoids. The mechanism of injury is hyperextension. Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Question 23
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?

Explanation
Tillaux and triplane fractures occur in adolescents as the result of an external rotation injury of the ankle. As seen on the CT scan, the growth plate starts to close during adolescence; therefore, growth arrest resulting in limb-length discrepancy or angulation is less of a concern in this age group than achieving joint congruity. The joint should be surgically reduced if displacement is greater than 2 mm to minimize the chances of late arthrosis. Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278. Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Question 24
Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient's diagnosis?



Explanation
The more severe the trauma, the higher the rate of subsequent clavicular nonunion. Neither duration nor type of immobilization has been clearly demonstrated to be a causative factor in the development of nonunion. Similarly, closed reduction has not been found to alter the healing course in midshaft clavicular fractures. Lazarus MD, Seon C: Fractures of the clavicle, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, vol 2, pp 1241-1242.
Question 25
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?

Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Question 26
Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?

Explanation
Minimally displaced fractures of the proximal humerus have a good outcome if physical therapy is initiated within 2 weeks of the injury. Results are not affected by age, open reduction and internal fixation, or involvement of the greater tuberosity. Immobilization for longer than 3 weeks will often result in stiffness. Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Question 27
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Explanation
The patient has extensive degenerative changes in both the medial and lateral compartments within the knee; therefore, arthroscopic debridement or an osteotomy will not be helpful. A patellar arthroplasty will not address the medial and lateral compartments. Because the extensor mechanism provides a significant amount of anteroposterior stability, a posterior cruciate-substituting total knee arthroplasty is the treatment of choice for this patient. Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Question 28
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show

Explanation
The radiograph shows the correct tibial tunnel and anterior femoral tunnel; therefore, range of motion will most likely show loss of flexion. Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin Sports Med 1999;18:109-171.
Question 29
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
The patient's neurologic examination is consistent with a C7 radiculopathy on the right side. In a patient with this symptom complex in the absence of trauma, a cervical disk herniation is the most common etiology for a C7 radiculopathy. There are eight cervical nerve roots and the C7 nerve exits at the C6-7 disk space and is most frequently impinged by a disk herniation at this level. Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Question 30
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?


Explanation
The MRI scans show a paralabral cyst, which is most commonly associated with labral tears. Compression of the suprascapular nerve results in weakness of the supraspinatus and/or infraspinatus depending on the level of compression. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 31
Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no voluntary motor function in her distal upper extremities or lower extremities. She does not have a bulbocavernosus reflex. She has a blood pressure of 80/50 mm Hg with a pulse of 50/min. Her hypotension does not improve with initial fluid resuscitation. Further treatment of her hypotension should consist of

Explanation
The hallmark of neurogenic shock is hypotension without tachycardia. It is associated most commonly with high cervical spinal cord injuries and results from loss of function of the sympathetic nervous system. Because the peripheral vasculature is dilated due to loss of its sympathetic tone, continued rapid administration of fluid corrects the hypotension and can quickly lead to fluid overload and congestive heart failure. Therefore, neurogenic shock is best treated by the use of pressors. Cardioversion or administration of antibiotics or systemic steroids is not appropriate treatment for this patient's hypotension. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Question 32
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
Radiographic findings in patients with rheumatoid arthritis include symmetric joint space narrowing, periacetabular and femoral head erosions, and diffuse periarticular osteopenia. In advanced stages, protrusio acetabuli is a common finding. Ranawat and associates have shown a rate of superior femoral head migration of 4.5 mm per year and medial (axial) migration of 2.5 mm per year. Asymmetric joint space narrowing is a classic radiographic finding of degenerative arthrosis. Sacroiliac joint ankylosis commonly occurs in ankylosing spondylitis. Hip synovitis is a pathologic diagnosis, not a radiographic finding. Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Question 33
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of

Explanation
A semiconstrained prosthesis can provide excellent results in carefully selected patients. Because the radiographs show extensive joint destruction with loss of the capitellum and trochlea, a capitellocondylar total elbow (unconstrained) prosthesis is contraindicated. Elbow fusion is poorly accepted, and the radiographs show too much articular destruction for a radial head excision, synovectomy, or interposition arthroplasty to be effective. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 34
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Explanation
The tenosynovium excised at the time of a carpal tunnel release for idiopathic carpal tunnel syndrome rarely shows signs of acute or chronic inflammation. Fibrosis, edema, and vascular sclerosis are the most common histologic findings. A tenosynovectomy with a carpal tunnel release usually is not necessary in the treatment of idiopathic carpal tunnel syndrome. Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225. Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Question 35
Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing total knee arthroplasty (TKA) prosthesis will have which of the following biomechanical effects?

Explanation
Increasing articular conformity increases the surface area for contact between the polyethylene and the femoral component. Advantages of this include lower peak contact stress within the polyethylene and less risk of polyethylene fatigue failure. Patellofemoral tracking is unchanged by increasing conformity unless gross component apposition is present. A potential disadvantage of increasing conformity includes some restriction in tibial rollback. Modest changes in conformity have not been shown to alter the rate of mechanical loosening. If conformity was increased to the extent of significant constraint, a potential increased risk of loosening would be expected, not a decrease. Design of modern TKAs includes a compromise in achieving enough constraint to lower polyethylene stress, without providing so much constraint as to limit kinematics and stress the fixation interfaces. D'Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop 2001;392:232-238.
Question 36
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?

Explanation
The vertebral artery is contained within the vertebral foramen and thus tethered alongside the vertebral body, making it vulnerable to injury if a drill penetrates the lateral wall. The C5 root passes over the C5 pedicle and is not in the vicinity. The C6 root passes under the C5 pedicle but is posterior to the vertebral artery and is only vulnerable at the very posterior-inferior corner. The carotid artery and the vagus nerve are both within the carotid sheath and well anterior. Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
Question 37
What pharmacologic agents are preferred for the treatment of symptomatic active Paget's disease?

Explanation
Recent medical literature supports the use of bisphosphonates as the treatment of choice for active Paget's disease.
Question 38
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?

Explanation
This view from the lateral portal shows a full-thickness rotator cuff tear. The glenohumeral joint can be visualized through this tear. The glenoid, labrum, and biceps tendon attaching to the superior aspect of the glenoid are easily viewed from this portal, and the arrow is pointing to the biceps tendon. Arthroscopic rotator cuff repair can be performed while visualizing from this portal and using anterior and posterior working portals. Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Question 39
A 48-year-old woman reports bilateral thigh pain that is limiting her function as a librarian. A radiograph and a bone scan are shown in Figures 23a and 23b. What is the most likely diagnosis?


Explanation
The radiograph reveals bilateral severe acetabular protrusio. The bone scan and history confirm involvement of multiple joints, including the knees and the hindfoot. Although the first four choices can all cause the acetabular protrusio, the associated multiple joint involvement suggests the diagnosis of rheumatoid arthritis. Arthrokatadysis, or primary protrusio acetabuli, is often associated with osteomalacia but not other joint disease. Developmental dysplasia is a common cause of bilateral hip pathology but does not have acetabular protrusio. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, pp 956-957. Wheeless' Textbook of Orthopaedics: Acetabular Protrusio. www.wheelessonline.com/ortho/acetabular_protrusio
Question 40
Which of the following factors is most critical to the success of a meniscal allograft transplantation?
Explanation
Success of a meniscal allograft transplantation is strongly dependent on accurate graft sizing, typically within 5% of the native meniscus. Previous studies have established that donor cell viability is not mandatory for the survival of these grafts since they are replaced by the recipient's cells (at least peripherally) within several weeks. Thus, cryopreservation of the graft to ensure cell viability is not necessary. There is a limited immune response to musculoskeletal allografts; therefore, immunosuppression, as is required for visceral organ transplantation, is not indicated. Wirth CA, Kohn D: Meniscal transplantation and replacement, in Fu FH, Harner CD, Vince JG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, vol 1, pp 631-641. Brautigan BE, Johnson DL, Caborn DM, et al: Allograft tissues, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 205-213.
Question 41
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?

Explanation
Excision of the fracture fragment typically leads to rapid return to function. Fixation techniques are difficult to perform because of the size of the bone; hardware prominence is common. Nerve deficits are not typically noted in this injury. The motor branch of the ulnar nerve in Guyon's canal must be protected during the surgical approach. Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Question 42
An axial T1-weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?

Explanation
The obturator vessels and nerve pass along the lateral pelvic wall along the true pelvic brim (nerve lies anterior to the vessels and lies on the obturator internus muscle) and descend into the obturator groove at the upper portion of the obturator foramen. Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Question 43
When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
Explanation
Exposure of polyethylene to radiation and then heating it to quench the free radicals leads to a cross-linked material. It converts a high molecular weight polyethylene macromolecule to an interpenetrating network structure of polymer chains. The ductility of the material is decreased, hence the greater risk of fracture. While the wear rate (measured as fewer and smaller particles) against a smooth counterface is markedly reduced, cross-linked polyethylene has shown a larger increase in wear rate when a rougher counterface is used compared to noncross-linked material. Due to reduced mechanical strength, highly cross-linked polyethylene is less resistant to abrasive wear.
Question 44
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?

Explanation
The MRI scan reveals a L4-L5 foraminal disk herniation originating from the L4-5 disk space that has migrated up into the foramen, compressing the left L4 nerve root. There is normal distribution of the roots in the cerebrospinal fluid, excluding arachnoiditis as a diagnosis, and disk herniation in this location would not result in cauda equina syndrome or myelopathy.
Question 45
Figures 39a and 39b show the MRI scans of a 25-year-old man with right shoulder pain. Figure 39c shows the arthroscopic view from a posterior portal in the beach chair position. What is the most likely diagnosis?



Explanation
The MRI scans show coronal oblique and sagittal oblique views of a partial articular surface supraspinatus tear or tendon avulsion (PASTA lesion). The arthroscopic view is a posterior portal of the glenohumeral joint viewing the articular surface of the supraspinatus. These tears are a common source of shoulder pain and are often amenable to transtendon arthroscopic repair without detachment of the intact bursal surface. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the shoulder. Am J Sports Med 2005;33:1088-1105. McConville OR, Iannotti JP: Partial-thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
Question 46
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?

Explanation
The most common deleterious side effect of ketamine is increased salivation and tracheobronchial secretions. For this reason, an antisialagogue agent should be given. While lack of sufficient respiratory depression is one of the major advantages of using ketamine, apnea can occur if the drug is given too rapidly intravenously. Emergence phenomena is common in adults but relatively rare in children. Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63. White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
Question 47
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of

Explanation
Although this is a fracture of the medial and lateral malleoli, the degree of displacement and comminution of the medial dome indicate that this injury is similar to a pilon fracture. Initial management should consistent of stabilization to allow for soft-tissue healing. The use of temporizing spanning external fixation should be the initial step, followed by limited or more extensive open reduction and internal fixation when the soft-tissue status will allow. Initial placement in either a short or long leg cast does not provide the needed stability and does not allow for care and monitoring of soft tissues. In addition, maintaining reduction of the talus may be very difficult. Immediate open reduction and internal fixation through an injured soft-tissue envelope adds the risk of difficulties with incision healing and a higher risk of deep infection. In the acute setting, a primary ankle fusion through this soft-tissue envelope is not indicated. Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509. Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 48
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
Conus medullaris syndrome most frequently occurs as a result of trauma or with a disk herniation at L1, resulting in a lower motor neuron syndrome but with a poor prognosis for recovery of bowel and bladder dysfunction. The conus region, as the termination of the spinal cord, contains the motor cell bodies of the sacral roots. The syndrome is usually a sacral level neural injury; therefore, lower extremity weakness is uncommon. Haher TR, Felmly WT, O'Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Question 49
Duchenne's muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?

Explanation
Patients with Duchenne's muscular dystrophy show progressive muscular weakness because of the absence of dystrophin and have the clinical picture of progressive muscle weakness. The condition is an X-linked genetic disease. Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Question 50
A 38-year-old marathon runner has had Achilles tendon pain for the past 2 months. Examination reveals that the tendon is thickened and tender proximal to the calcaneal insertion. The tendon sheath is not thickened or tender. The pathophysiology of the tendon is best described as
Explanation
Atraumatic Achilles tendon disease can be differentiated into Achilles tendinosis and peritendinitis. Thickening and tenderness of the Achilles tendon are present in both, but thickening and tenderness of the tendon sheath indicates peritendinitis. Histologic examination of Achilles tendinosis reveals an absence of acute and chronic inflammatory cells. Radiologists often diagnose partial tendon rupture by MRI and there may be microscopic longitudinal tears present, but there is no mechanical compromise as would be implied by a partial rupture. The thickening typically occurs in the portion of the tendon with the poorest blood supply, and biochemical analysis detects high levels of lactate and other products of anaerobic glycolysis. Astrom M, Rausing A: Chronic Achilles tendinopathy: A survey of surgical and histopathologic findings. Clin Orthop 1995;316:151-164. Ohberg L, Lorentzon R, Alfredson H: Neovascularisation in Achilles tendons with painful tendinosis but not in normal tendons: An ultrasonographic investigation. Knee Surg Sports Traumatol Arthrosc 2001;9:233-238.
Question 51
Figures 45a through 45c show the radiograph, CT scan, and MRI scan of a 15-year-old boy who has lateral ankle pain. What is the most likely diagnosis?



Explanation
The elongated anterior process of the calcaneus reaching distally toward the navicular is an abnormal finding. Instead of viewing the rounded, blunt distal anterior process of the calcaneus, a bridge extends to the navicular, albeit incomplete. These findings are consistent with a fibrous coalition. CT can reveal a stress fracture of the calcaneus, arthritis of the subtalar joint with subchondral cysts, or an os peroneal bone disruption in the peroneus longus, but those entities are not shown here. The plantar fascia is intact. Richardson EG: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 702-732.
Question 52
What is the most appropriate surgical treatment for a stage III symptomatic scapholunate advanced collapsed (SLAC) wrist?
Explanation
SLAC is the end result of chronic scapholunate instability. The arthritis follows a predictable pattern. Stage I disease involves cartilage loss between the waist of the scaphoid and the radial styloid. In stage II, the arthritis progresses to include the proximal pole of the scaphoid and the scaphoid fossa of the radius. Finally, stage III goes on to include arthritis of the capitolunate joint. The only treatment option that addresses all of the sites of arthritis is the scaphoid excision and four corner fusion. Ashmead DT IV, Watson HK, Damon C, et al: Scapholunate advanced collapse wrist salvage. J Hand Surg Am 1994;19:741-750.
Question 53
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?

Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 54
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
There is a negative change of calcium balance with a decrease in intestinal absorption and an increase in urinary calcium loss. The reduction of intestinal absorption is accompanied by reduced circulating concentrations of total, but not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial. Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Question 55
A 30-year-old woman has pain in her right hand. The radiograph, CT scan, and biopsy specimen are seen in Figures 38a through 38c. What is the most likely diagnosis?



Explanation
An enchondroma is the most common primary tumor of the long bones of the hand. The lesion is usually asymptomatic and often is detected when there is a pathologic fracture. Shimizu K, Kotoura Y, Nishijima N, Nakamura T: Enchondroma of the distal phalanx of the hand. J Bone Joint Surg Am 1997;79:898-900.
Question 56
A 21-year-old pitcher reports shoulder pain with hard throwing. He notes that the pain occurs in the early acceleration phase of his throw. Given his history, what structures are at greatest risk for injury?
Explanation
Internal impingement in the thrower's shoulder occurs in the abducted, externally rotated position as described by Walch and associates. The injury is thought to occur from repetitive contact between the posterosuperior portion of the labrum and glenoid against the articular side of the rotator cuff and greater tuberosity. Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40. Jazrawi LM, McCluskey GM III, Andrews JR: Superior labral anterior and posterior lesions and internal impingement in the overhead athlete. Instr Course Lect 2003;52:43-63.
Question 57
Thermal capsulorrhaphy of the inferior glenohumeral ligament can cause iatrogenic injury to which of the following nerves?
Explanation
The axillary nerve courses from anterior to posterior just below the inferior shoulder capsule. Thermal energy applied to the inferior aspect of the shoulder capsule can result in injury to this nerve. Wong KL, Williams GR: Complications of thermal capsulorrhaphy of the shoulder. J Bone Joint Surg Am 2001;83:151-155.
Question 58
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
Recent articles have looked at the cyclic load failure and ultimate load failure of biceps tenodesis techniques. The interference screw has proved superior to bone tunnel, suture anchor, and soft-tissue tenodesis techniques in laboratory cadaveric testing. Whether this is clinically relevant or not is still unknown. Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Question 59
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
Patient safety and prevention of medical errors is a major focus of recent national advocacy groups. Analysis has shown that the most common sentinel event in spine surgery is surgery on the wrong level. Therefore, it is recommended that every patient have the surgical site signed, the level of surgery marked intraoperatively, and a radiograph taken. Surgery on the wrong level is most likely to occur in single-level decompressive procedures. Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Question 60
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20 degrees. Management should now consist of

Explanation
The history, physical examination, and radiographs indicate that the patellofemoral pain is most likely caused by excessive lateral patellar pressure and patellar maltracking. Because the radiographs reveal the lateral tilt of the patella and lateral subluxation, the treatment of choice is bilateral lateral releases with anteromedialization of the tibial tubercles. This procedure corrects not only the excessive lateral patellar pressure, but also the lateral subluxation. The use of patella-stabilizing braces or taping may provide temporary relief, but these implements are not well-tolerated and they will not change the underlying biomechanics of the knee. Simple lateral release is indicated for isolated lateral tilt, but it does not correct the lateral subluxation. The use of thermal capsular shrinkage for the medial retinaculum has not been proven to provide long-term correction of the deformity. Boden BP, Pearsall AW, Garrett We Jr, et al: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
Question 61
Figures 28a through 28c show the MRI scans of a 30-year-old woman who weighs 290 lb and has low back and left leg pain. She also reports frequent urinary dribbling, which her gynecologist has advised her may be related to obesity. Examination will most likely reveal



Explanation
The patient will most likely exhibit ipsilateral weakness of the tibialis anterior. Gaenslen's test is designed to detect sacroiliac inflammation as a source of low back pain. Beevor's sign tests the innervation of the rectus abdominus and paraspinal musculature (L1 innervation). The extensor hallucis longus is predominantly innervated by L5. The peroneals are predominantly innervated by S1. Hoppenfeld S: Physical Examination of the Spine and Extremities. Appleton, WI, Century-Crofts, 1976.
Question 62
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?

Explanation
Excessive flexion gap tightness can be addressed with a variety of techniques; including: (a) recess and release the posterior cruciate ligament; (b) resect a posterior slope in the tibia; (c) avoid an oversized femoral component that moves the posterior condyles more distally; (d) resect more posterior femoral condyle and use a smaller femoral component placed more anteriorly; and (e) release the tight posterior capsule and balance the collateral ligaments.
Question 63
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Explanation
The term 'spinal shock' applies to all phenomena surrounding physiologic or anatomic transection of the spinal cord that results in temporary loss or depression of all or most spinal reflex activity below the level of the injury. Hypotension and bradycardia caused by loss of sympathetic tone is a possible complication, depending on the level of the lesion. The mechanism of injury that causes spinal shock is usually traumatic in origin and occurs immediately, but spinal shock has been described with mechanisms of injury that progress over several hours. Spinal cord reflex arcs immediately above the level of injury also may be depressed severely on the basis of the Schiff-Sherrington phenomenon. The end of the spinal shock phase of spinal cord injury is signaled by the return of elicitable abnormal cutaneospinal or muscle spindle reflex arcs. Autonomic reflex arcs involving relay to secondary ganglionic neurons outside the spinal cord may be affected variably during spinal shock, and their return after spinal shock abates is variable. The returning spinal cord reflex arcs below the level of injury are irrevocably altered and are the substrate on which rehabilitation efforts are based.
Question 64
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
The annulus fibrosis has a multilayer lamellar architecture mode of type I collagen fibers. Each successive layer is oriented at 30 degrees to the horizontal in the opposite direction, leading to a "criss-cross" type pattern. This composition allows the annulus, which has the highest tensile modulus, to resist torsional, axial, and tensile loads.
Question 65
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?

Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 66
What common cytologic abnormality is associated with Ewing's sarcoma?
Explanation
Cytogenetic abnormalities have been well characterized in a number of tumors. Translocation t (2, 13), (x, 18), (12, 16), and (12, 22) have been characterized in rhabdomyosarcoma, synovial cell sarcoma, myxoid liposarcoma, and clear cell sarcoma, respectively. Translocation t(11:22) can be identified in 95% of patients with Ewing's sarcoma. This was first described by Turc-Carel and associates in 1984. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, pp 105-118. Turc-Carel C, Philip I, Berger MP, Philip T, Lenoir GM: Chromosome study of Ewing's sarcoma (ES) cell lines: Consistency of a reciprocal translocation t(11;22) (q24;q12). Cancer Genet Cytogenet 1984;12:1-19.
Question 67
A 14-year-old boy has had knee pain for the past 2 months. He also has a low-grade fever of 101.3 degrees F (38.5 degrees C). Laboratory studies show a WBC count of 12,100/mm3 and an erythrocyte sedimentation rate of 58/h. A biopsy specimen of a lesion in the distal femoral metaphysis is shown in Figure 38. What is the most appropriate treatment?

Explanation
The clinical presentation of this patient is consistent with both acute osteomyelitis and Ewing's sarcoma. Both entities can be noted in the distal femoral metaphysis although Ewing's sarcoma is classically noted in the diaphysis. The histology reveals a mixed inflammatory cell infiltrate with neutrophils, plasma cells, lymphocytes, and histiocytes. Ewing's sarcoma would be a uniform population of small round blue cells without an inflammatory component. Eosinophilic granuloma (EG) is characterized by Langerhans histiocytes and eosinophils. Treatment of EG often consists of an intralesional steroid injection. Treatment of acute osteomyelitis includes surgical debridement and antibiotics. McCarthy JJ, Dormans JP, Kozin SH, et al: Musculoskeletal infections in children: Basic treatment principles and recent advancements. Instr Course Lect 2005;54:515-528.
Question 68
Tension force in the anterior cruciate ligament during passive range of motion is highest at
Explanation
Tension forces in the healthy, as well as the reconstructed, anterior cruciate ligament were measured and found to be highest with the knee in full extension and decreased as the flexion increased. Markolf KL, Burchfield DM, Shapiro MM, et al: Biomechanical consequences of replacement of the anterior cruciate ligament with a patellar ligament allograft. Part II: Forces in the graft compared with forces in the intact ligament. J Bone Joint Surg Am 1996;78:1728-1734.
Question 69
What range of motion parameters are required for a patient with posttraumatic elbow stiffness to accomplish all the normal activities of daily living?
Explanation
Activities of daily living such as dressing, eating, and bathing can all be performed with elbow motion through a 100 degrees arc of flexion and extension (30 degrees to 130 degrees) and a 100 degrees arc of forearm rotation (50 degrees pronation, 50 degrees supination). Some patients can accomplish these activities of daily living with 10 degrees less motion at each end point. This is referred to as the functional arc of motion. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 70
What is the most common complication following arthroscopic capsular release in a patient with adhesive capsulitis of the shoulder?

Explanation
Although all of the above are potential complications after arthroscopic capsular release for adhesive capsulitis, the most common problem is the failure to regain normal glenohumeral motion. An immediate physical therapy program is critical to prevent this complication. Ghalambor N, Warner JJP: Arthroscopic capsular release: Evolution of the technique and its applications. Tech Shoulder Elbow Surg 2000;1:52-60.
Question 71
Figures 19a through 19c show radiographs of the cervical spine of an asymptomatic patient with Down syndrome who wants to participate in a Special Olympics running event. The neurologic examination is normal. Management should consist of



Explanation
An atlanto-dens interval (ADI) of up to 4 mm in children is considered normal. Children with Down syndrome have increased ligamentous laxity, with atlantoaxial instability occurring in as many as 15% to 20% of patients. These patients are at risk for catastrophic injury following minor trauma and should be routinely screened for instability, generally beginning when the patient starts to walk. Patients with an ADI of greater than 5 mm should avoid contact sports and high-risk activities such as gymnastics, diving, the high jump, and the butterfly stroke. The American Academy of Pediatrics Committee of Sports Medicine and Fitness guidelines recommend that lateral views of the cervical spine in neutral, flexion, and extension should be obtained in all children with Down syndrome who wish to participate in sports. Patients with normal radiographs and examinations do not need repeat radiographs, although some authors suggest that instability increases with age, and therefore recommend repeat radiographs every 5 years. Cervical spine fusion in patients with Down syndrome has a high rate of complications and should be performed only on patients with symptoms and evidence of myelopathy. American Academy of Pediatrics Committee of Sports Medicine and Fitness: Atlantoaxial instability in Down syndrome. Pediatrics 1995;96:151-154. Copley LA, Dormans JP: Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:204-214.
Question 72
Which of the following definitions best describes Batson's vertebral vein system?

Explanation
The venous plexus was described by Batson and helps to explain the common distribution of metastatic cells to the vertebrae, skull, ribs, and proximal long bones. Batson studied the vertebral vein system extensively by using contrast agents in human cadavers and live monkeys. Batson's plexus is a valveless system that allows retrograde embolism from the major organs such as the breast, prostate, lung, kidney, and thyroid. It is located within the thoracoabdominal cavity and has connections to the proximal long bones and an intercommunicating network of thin-walled veins with a low intraluminal pressure. Batson OV: Function of vertebral veins and their role in spread of metastases. Ann Surg 1940;112:138-149.
Question 73
A 10-year-old child reports acute leg pain after wrestling with his brother. AP and lateral radiographs are shown in Figures 21a and 21b. What is the best course of action?


Explanation
The radiographs show an eccentric metaphyseal lesion with a well-defined reactive rim of bone that is consistent with a nonossifying fibroma. Pathologic fractures through benign lesions should be treated as appropriate for the fracture, allowing the fracture to heal. Biopsy is not needed when the radiographic diagnosis is benign. MRI, in the presence of a fracture, is not particularly helpful because of the hematoma. If radiographic findings reveal that the lesion appears aggressive, a biopsy should be performed, obtaining tissue away from the fracture site. Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377.
Question 74
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?

Explanation
Several studies have shown that sitting ability by age 2 years is highly prognostic of walking. Molnar and Gordon reported that children not sitting independently by age 2 years had a poor prognosis for walking. Wu and associates reported that children sitting without support by age 2 years had an odds ratio of 26:1 of walking compared with those unable to sit. This was far higher than the odds ratios for cerebral palsy location, motor dysfunction, crawling, creeping, scooting, or rolling. Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Question 75
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Explanation
According to a recent study, cemented pegged glenoid components had fewer radiolucent lines initially and at 2-year follow-up when compared to a cemented keeled design. Curve-backed designs have also shown fewer radiolucent lines when compared to flat-backed designs. Oversizing the glenoid can lead to impaired rotator cuff function and decreased range of motion. An off-centered glenoid can lead to early loosening. Gartsman GM, Elkousy HA, Warnock KM, et al: Radiographic comparison of pegged and keeled glenoid components. J Shoulder Elbow Surg 2005;14:252-257. Szabo I, Buscayret F, Edwards TB, et al: Radiographic comparison of flat-back and convex-back glenoid components in total shoulder arthroplasty. J Shoulder Elbow Surg 2005;14:636-642.
Question 76
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
The triad of menstrual dysfunction, disordered eating, and stress fracture is well recognized in women who participate in endurance sports. The best treatment remains to be determined, but at present, the combination of oral contraceptives to regulate menses, an increased intake of calcium and vitamin D, as well as nutritional counseling, is the recommended treatment for decreased bone mass related to exercise-induced amenorrhea. Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
Question 77
A 52-year-old woman with diabetes mellitus has had a plantar foot ulcer under the second metatarsal head for the past week. The patient had a similar ulcer 2 months ago, and total contact casting resulted in healing. Examination reveals no signs of infection. What procedure will best prevent recurrence of the ulcer?
Explanation
The contracted Achilles tendon leads to increased forefoot pressure, thus increasing the risk for ulceration in neuropathic patients. Several studies have shown the benefit of Achilles tendon lengthening to heal and prevent forefoot ulceration in these patients. The flexor hallucis longus transfer is used for chronically torn/deficient Achilles tendons, not a contracted Achilles tendon. The Jones procedure works well for the first ray but does not help to alleviate pressure under the second ray. Peripheral bypass surgery is unnecessary because the ulcer healed during the initial treatment, indicating that the patient has adequate circulation. The posterior tibial tendon transfer is used for foot drop or other neuromuscular conditions to correct deformity and increase function. It is not used for forefoot ulcers in patients with diabetes mellitus. Armstrong DG, Stacpoole-Shea S, Nguyen H, et al: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 78
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?

Explanation
Varus position of the stem is most commonly associated with failure of the cemented femoral component because of association with an inadequate cement mantle in the proximal medial and distal lateral zones. An inadequate cement mantle and obesity have been associated with increased loosening but not as frequently as a varus deformity. The influences of gender and osteoporotic bone on the outcome of cemented femoral components have not been established. Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Question 79
A 6-year-old girl is referred for the elbow injury seen in Figure 2. What is the most appropriate treatment?

Explanation
The patient has a displaced lateral condyle fracture; therefore, simple immobilization for 3 to 8 weeks is likely to result in malunion or nonunion. Closed reduction of such injuries is rarely successful. The fracture is unstable, so fixation is required after open reduction. Because the fixation must cross the physis, smooth pins are indicated for the skeletally immature elbow. Open reduction with fixation has been shown to reduce the risk of delayed union and malunion. Beaty JH, Kasser JR: The elbow: Physeal fractures, apophyseal injuries of the distal humerus, avascular necrosis of the trochlea, and T-condylar fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 625-703. Rutherford A: Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am 1985;67:851-856.
Question 80
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?

Explanation
There is no identifiable thoracic, abdominal, or long bone source of ongoing bleeding. The patient has a lateral compression Burgess-Young type I pelvic ring injury. This injury does not increase the pelvic volume because it is not unstable in external rotation. Application of a PASG, a pelvic clamp, or an external fixator may be helpful if the patient has a pelvic injury that is unstable in external rotation or translation but would be of little use in this injury pattern. Persistent hemodynamic instability after administration of 4 units of blood is the decision point where most authors would recommend angiography and embolization. If the pelvis is unstable in external rotation or translation, inflation of the PASG trousers or application of an external fixator is recommended before angiography. Attributing the hemodynamic instability to the head injury before ruling out the pelvis as a source is not indicated. Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856. Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Question 81
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?

Explanation
Half pins placed in the AIIS are an alternative to pins placed in the iliac crest. A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated "over the top" of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 82
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?

Explanation
Uneven resection of bone, typically leaving a retained posterolateral corner of the distal clavicle, can lead to failure of arthroscopic distal clavicle excision. The amount of bone resected, the gender of the patient, or the diagnosis (osteoarthritis versus osteolysis) does not appear to affect the results.
Question 83
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include


Explanation
The radiographs do not show significant arthrosis of the hallux metatarsophalangeal joint; therefore, arthrodesis is unnecessary. Orthotics will not correct the deformity. A distally based osteotomy will not achieve sufficient correction of the incongruity of deformity, and a Keller resection is not indicated in the younger population. The treatment of choice is a proximal metatarsal osteotomy with second toe correction.
Question 84
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of

Explanation
Nonsurgical management such as a functional brace, hanging arm cast, or sugar tong splint is the treatment of choice for a fracture of the humeral shaft that is the result of throwing. The fracture surface typically is wide and the degree of displacement is not large; therefore, surgery is not indicated in most patients. Ogawa K, Yoshida A: Throwing fracture of the humeral shaft: An analysis of 90 patients. Am J Sports Med 1998;26:242-246.
Question 85
In a postganglionic brachial plexus lesion at Erb's point (point of formation of the upper trunk by the C5 and C6 nerve roots), which of the following nerves will still function normally?

Explanation
In a postganglionic injury to the brachial plexus, the rhomboid muscle, innervated by the dorsal scapular nerve, would still be expected to function. This is a useful clinical sign that the brachial plexus lesion is postganglionic as opposed to preganlionic. The musculocutaneous, axillary, and suprascapular nerves are all located distal to Erb's point (the most common location of an upper nerve root brachial plexus injury), and all contain fibers from the C5 and C6 nerve roots. Therefore, these nerves are not expected to function normally following a postganglionic C5 and C6 nerve root injury. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29.
Question 86
Which of the following positions of immobilization has been shown to best approximate the anterior labrum against the glenoid rim following anterior dislocation of the shoulder?

Explanation
Following anterior dislocation of the shoulder, the affected arm is typically placed in a sling with the shoulder in adduction and internal rotation. A recent study has shown that placement in this position actually results in laxity of the anterior supporting structures of the shoulder, allowing the postinjury hemarthrosis to push the labrum and capsular ligaments away from the anterior glenoid rim. Thus, immobilization in this position may actually impede healing of these structures. Alternatively, resting the arm in a position of adduction and external rotation allows the anterior supporting structures to abut against the anterior glenoid rim by forcing the hemarthrosis posteriorly. Placing the arm in this position following anterior dislocation is believed to allow for better healing of the anterior labrum and ligaments.
Question 87
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?

Explanation
The infant has a well-positioned hip in the Pavlik harness and treatment should be continued in the current position. The success rate is over 90% with the use of this device for a dislocatable hip. Ultrasound is a useful tool to confirm appropriate positioning of the cartilaginous femoral head during treatment. If the femoral head is not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 88
A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm3. The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?

Explanation
Synovial fluid analysis is a very sensitive tool for detecting infection in total knee arthroplasties. Several studies have demonstrated that an absolute leukocyte count in the synovial fluid of less than 1,700 to 2,500/mm3 is an accurate predictor of absence of infection. Similarly, a differential cell count of the WBCs demonstrating less than 50% to 60% neutrophils is an accurate predictor of absence of infection. If both parameters are normal, it is unlikely that the patient has an infection. The three surgical options are contraindicated based on the normal examination findings and laboratory parameters. Similarly, antibiotics should be avoided. The work-up should include tests to evaluate noninfectious sources of knee pain and sources of referred knee pain. Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562. Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.
Question 89
When using the direct lateral (or Hardinge) approach for hip arthroplasty, three muscles are detached from the femur. In addition to the vastus lateralis, they include the
Explanation
This approach is criticized for the episodic limp associated with the muscle detachment and reattachment. Classically, two thirds of the gluteus medius is detached as a sleeve with the vastus lateralis. This exposes the gluteus minimus and the ligament of Bigelow. These must also be detached to allow dislocation of the hip and osteotomy of the femoral neck. The rectus femoris lies medially and anteriorly and does not need to be addressed. The piriformis and obturator internus are exposed during the posterior approach. Neither the gluteus maximus nor tensor fascia lata attach to the anterior femur. The sartorius and iliopsoas are not exposed during this dissection. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Question 90
Figures 1a through 1c show the radiograph and MRI scans of a 16-year-old patient who has a painful hip. Examination reveals a significant limp, limited abduction and internal rotation, and severe pain with internal rotation and adduction. A biopsy specimen is shown in Figure 1d. What is the deposited pigment observed in this condition?




Explanation
Pigmented villonodular synovitis (PVNS) is a synovial proliferative disorder that remains a diagnostic difficulty. The most common clinical features are mechanical pain and limited joint motion. On radiographs, the classic finding is often a large lesion, associated with multiple lucencies. Other findings may include a normal radiographic appearance, loss of joint space, osteonecrosis of the femoral head, or acetabular protrusion. MRI is the imaging modality of choice and will show the characteristic findings of a joint effusion, synovial proliferation, and bulging of the hip. The synovial lining has a low signal on T1- and T2-weighted images, secondary to hemosiderin deposition. Copper deposition occurs in patients with Wilson's disease, which mainly affects the liver. Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Question 91
Examination of a 23-year-old female college basketball player who has had anterior knee pain for the past 3 weeks reveals tenderness and fullness over the inferior patella and proximal patellar tendon. There is no patellofemoral crepitus, patella apprehension sign, or anterior or posterior instability. Initial management should include
Explanation
The patient has patellar tendinitis (jumper's knee). It is a common overuse condition seen in runners, volleyball players, soccer players, and jumpers but can be seen in any activity in which repeated extension of the knee is required. In the acute setting, the pain is well localized and there is tenderness and sometimes swelling of the tendon. MRI is recommended for evaluating chronic cases and for surgical planning. In the acute phases, ice, rest, and avoidance of the offending activity are recommended. Weakness of the quadriceps and hamstring muscle are thought to contribute to this problem; therefore, stretching and isometric exercise in a limited range of motion are important. Complete rest and intratendinous injections of steroids are detrimental to tendon physiology. Stanish WD, Rubinovich RM, Curwin S: Eccentric exercise in chronic tendinitis. Clin Orthop 1986;208:65-68.
Question 92
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of


Explanation
The problem with this reconstruction is the medial protrusion of the base plate. The use of a base plate with an offset stem can prevent the protrusion and thus the impingement and pain. Allograft bone or smoothing the outline with cement would be just as prominent and likely to cause pain. An ingrowth surface may improve soft-tissue attachment but would still leave the implant protruding medially and likely to cause pain. A nonstemmed tibial base plate would lead to less medial protrusion but at the expense of a smaller area for load carriage on the proximal tibia.
Question 93
Osteoporosis is best diagnosed by
Explanation
Risk factors can suggest the existence of osteoporosis. However, definitive testing, based on the use of bone densitometry measurements, uses the T score in which an average score is taken from a normal population of young women. The presence of increased osteoid in lamellar bone is seen in osteomalacia but not osteoporosis. The presence of fractures is evidence of a risk factor for osteoporosis and can predict future fractures, but it does not definitively confirm the diagnosis. The Singh index is a radiographic finding that is not as accurate as bone mineral density scores.
Question 94
A 26-year-old man has had hand pain and progressive swelling in the knuckle for the past several months. He denies any trauma to the hand. The ring finger metacarpophalangeal joint is tender, and there is loss of motion in the digit. Figure 32a shows the radiograph and Figures 32b through 32d show the T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. What is the most likely diagnosis?




Explanation
The radiograph reveals a subchondral lesion in the metacarpophalangeal joint that is lytic and expansile. The MRI scans show a mass that is moderate in intensity on the T2-weighted image and has some gadolinium uptake. There are no cystic components in this lesion. The subchondral location and expansile nature are highly suggestive of giant cell tumor of bone. A lesion with this appearance might also represent an aneurysmal bone cyst, given the amount of expansion present. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 113-118.
Question 95
Where is the watershed zone for tarsal navicular vascularity?

Explanation
The central one third has been established as the watershed zone by angiographic studies, and has been borne out in clinical conditions involving the navicular, such as stress fractures and osteonecrosis. These findings account for the susceptibility to injury at this level. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 239-242.
Question 96
A 55-year-old man underwent cementless total hip arthroplasty for advanced painful osteoarthritis of the hip 2 years ago. The follow-up radiograph shown in Figure 30 shows

Explanation
The radiograph shows a well-osseointegrated tapered stem with a metaphyseal porous coating, spot welds in the porous region, and calcar rounding. Trochanteric stress shielding and distal cortical hypertrophy are also signs of ingrown stems but are seen more frequently in association with extensively porous-coated stems exhibiting diaphyseal ingrowth. There is no evidence of lucent lines or a pedestal, signs that suggest instability. Femoral stem subsidence can be determined only by a review of sequential radiographs. Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990;257:107-128.
Question 97
Why is tendon considered an anisotropic material?
Explanation
Anisotropic materials have mechanical properties that vary based on the direction of loading. The relative values of Young's modulus for tendon, ligament, and bone are not relevant to isotropy. The mechanical properties of tendon do change with preconditioning, but this change is related to viscoelasticity. The intrinsic mechanical properties of tendon do vary with the rate of loading, but this variance is related to viscoelasticity. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Question 98
Which of the following best describes the resultant forces on an increased offset stem when compared with a standard offset stem?

Explanation
The increased emphasis on restoring offset in total hip arthroplasty has implications for the forces applied to the components and the fixation interfaces. Static analysis has shown that with an increased affect, joint reaction force on the articulation is decreased. When the resultant load on the hip is "out of plane" (ie, directed anterior to posterior), there is increased torsion where the stem is turned into more retroversion. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180. Hurwitz DE, Andriaacchi TP: Biomechanics of the hip, in Callaghan J, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven , 1998.
Question 99
A 25-year-old laborer sustains a transverse fracture of the proximal 25% of the scaphoid. CT reconstructions reveal a 1-mm fracture gap. What is the most appropriate treatment?
Explanation
A higher risk of nonunion and the need for prolonged immobilization is seen after nonsurgical management of proximal pole fractures of the scaphoid. Because of the relatively poor blood supply of the proximal pole, surgical treatment with a compression screw is advocated for fractures of the proximal third of the scaphoid. Clay NR, Dias JJ, Costigan PS, et al: Need the thumb be immobilized in scaphoid fractures? A randomised prospective trial. J Bone Joint Surg Br 1991;73:828-832.
Question 100
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?

Explanation
The patient has a large zone of osteonecrosis of the left femoral head. The wedge-shaped zone of decreased signal intensity on the T1 image in the subchondral region of the femoral head is typical. Based on these findings, total hip arthroplasty is the most appropriate treatment. Open reduction and internal fixation will not help this condition. Incisional biopsy is indicated only if the MRI scan shows a probable neoplasm. Resection of the proximal femur is indicated only for aggressive malignancy. Arthrodesis may be considered in a younger patient but not in a 68-year-old individual. Other treatments, not listed, such as core decompression, vascularized fibular transplant, and osteotomy may be options in selected patients. Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.
