
Introduction & Epidemiology
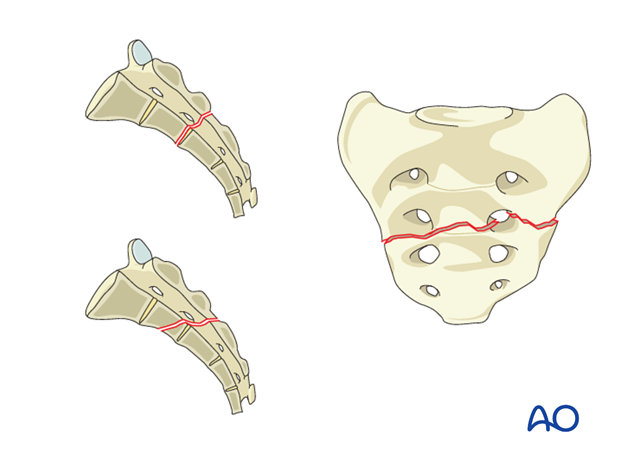
Sacral fractures represent a critical component of pelvic ring injury management, often associated with significant morbidity due to their proximity to vital neurological and vascular structures. This document focuses on nondisplaced transverse fractures, specifically the A2 subtype as defined by the AO/OTA classification, which typically involves the sacrum below the S1-S2 joint.
Sacral fractures are broadly classified based on their anatomical location and morphology. The Denis classification system categorizes sacral fractures into three zones:
*
Zone I (Ala fractures):
Lateral to the sacral foramina, typically involving the sacral ala. Neurological injury risk is lower, primarily involving L5 nerve root impingement.
*
Zone II (Foraminal fractures):
Through the sacral foramina, often extending into the sacral canal. Higher risk of neurological injury, affecting individual sacral nerve roots.
*
Zone III (Central fractures):
Medial to the sacral foramina, involving the central sacral canal. Highest risk of neurological injury, including cauda equina syndrome, due to direct impingement on multiple sacral nerve roots. Transverse sacral fractures, such as the A2 subtype, commonly fall into Denis Zone III.
The AO/OTA classification, particularly for pelvic ring injuries (61-A, B, C), further refines this by incorporating stability. An A2 sacral fracture is characterized as an isolated, stable sacral fracture without involvement of the anterior pelvic ring, often presenting as a nondisplaced transverse fracture. This designation typically implies mechanical stability, dictating a nonoperative management strategy.
Epidemiologically, sacral fractures can result from high-energy trauma (e.g., motor vehicle collisions, falls from height) or low-energy mechanisms in osteoporotic patients. High-energy injuries often involve concomitant pelvic ring or visceral damage, while low-energy fractures in the elderly are increasingly prevalent and may present as isolated injuries. The incidence of neurological deficits associated with sacral fractures varies significantly based on fracture type and displacement, ranging from 0% in some Zone I fractures to over 50% in displaced Zone III fractures. For nondisplaced transverse fractures (A2), the likelihood of cauda equina injury is low, as highlighted by the seed content: "This is a nondisplaced transverse fracture below the SI-Joint with a low likelihood of cauda equina injury."
AO/OTA A2 Sacral Fracture Illustration:
Surgical Anatomy & Biomechanics
A thorough understanding of sacral anatomy and pelvic biomechanics is paramount for managing sacral fractures. The sacrum, a keystone element of the pelvic ring, is formed by the fusion of five sacral vertebrae (S1-S5) and articulates superiorly with L5, laterally with the ilium (forming the sacroiliac joints), and inferiorly with the coccyx.
Key Anatomical Features:
*
Sacral Canal:
Houses the cauda equina and sacral nerve roots (S1-S5). Fractures extending into this canal carry a significant risk of neurological compromise.
*
Sacral Foramina:
Anterior and posterior foramina transmit the ventral and dorsal rami of the sacral nerves, respectively. Fractures traversing these foramina (Denis Zone II) can lead to isolated sacral radiculopathies.
*
Sacroiliac (SI) Joints:
Strong syndesmotic and synovial joints, critical for transferring axial loads from the spine to the lower extremities. Ligamentous structures (anterior, posterior, and interosseous SI ligaments, sacrotuberous, sacrospinous ligaments) provide substantial stability to the posterior pelvic ring.
*
Lumbosacral Junction:
The articulation between L5 and S1, stabilized by the iliolumbar ligaments. Disruption here can lead to spinopelvic instability.
Biomechanics of the Pelvic Ring:
The pelvic ring functions as a closed loop, dissipating forces and enabling load transfer. Its stability depends on the integrity of both anterior (pubic symphysis, rami) and posterior (sacrum, SI joints, associated ligaments) elements.
*
Posterior Stability:
Primarily conferred by the sacrum and its robust ligamentous attachments. The posterior sacroiliac ligaments are the strongest, resisting vertical and rotational forces.
*
Sacral Stress Risers:
The sacrum is weakest at the levels of the sacral foramina and the central body, making these common sites for fracture. Transverse fractures, particularly those in the lower sacrum (S2-S5), are often a result of direct trauma or avulsion forces.
*
Load Transmission:
During upright posture and ambulation, axial loads are transmitted from the spine through the SI joints to the femoral heads. The sacrum bears significant compressive and shear forces.
*
Neurological Vulnerability:
The sacral canal and foramina make the contained neural elements highly susceptible to injury from fracture displacement, hematoma, or direct compression. Transverse fractures involving the lower sacrum (S2-S5), while often stable mechanically, can still impinge on the lower sacral roots affecting bowel, bladder, and sexual function. Cauda equina syndrome, though less common in nondisplaced fractures, remains a critical concern, especially with any degree of displacement into the canal.
For an A2 nondisplaced transverse fracture below the S1-S2 joint, the primary biomechanical insult is localized disruption of the sacral cortex and trabeculae. Crucially, the absence of significant displacement implies the overall integrity of the pelvic ring is maintained, and there is no overt impingement on the sacral canal, which underpins the low likelihood of cauda equina injury. However, local pain and tenderness can be significant due to periosteal and fracture-site irritation.
Indications & Contraindications
Management of sacral fractures, including nondisplaced transverse patterns, hinges on a meticulous assessment of fracture stability, neurological status, and patient factors. The AO/OTA A2 classification specifically denotes a stable, isolated sacral fracture.
Main Indications for Nonoperative Treatment (A2 Nondisplaced Transverse Fractures):
*
Essentially all closed A2 sacral fractures:
These are mechanically stable and nondisplaced.
*
Intact neurological function:
Absence of cauda equina syndrome, isolated sacral radiculopathy, or other neurological deficits attributable to the fracture.
*
Stable pelvic ring:
No evidence of concomitant anterior or posterior pelvic ring instability on imaging (e.g., symphyseal diastasis, SI joint disruption, significant displacement of other sacral fractures).
*
Patient factors:
Ability to adhere to activity restrictions and participate in rehabilitation.
Main Indications for Operative Treatment (for Sacral Fractures in General,
not
typically for A2 nondisplaced):
While A2 nondisplaced transverse sacral fractures are predominantly managed non-operatively, a comprehensive understanding of sacral fracture care necessitates outlining indications for operative intervention in other sacral fracture patterns, as these may coexist or present differently.
*
Displaced sacral fractures:
Displacement of greater than 1 cm in any plane, particularly translation or angulation that compromises the pelvic ring.
*
Unstable pelvic ring injuries:
Associated with anterior ring disruption (e.g., symphyseal diastasis >2.5 cm, bilateral pubic rami fractures) or other unstable posterior injuries (e.g., vertical sacral fractures, SI joint dislocation, U-type or H-type sacral fractures with significant displacement).
*
Neurological deficit:
Progressive or severe neurological deficits, especially cauda equina syndrome, often warrant urgent surgical decompression and stabilization. This is a critical distinction from the low likelihood in A2 nondisplaced fractures.
*
Open sacral fractures:
Requires debridement and stabilization to prevent infection and facilitate wound healing.
*
Polytrauma patients:
Often require early stabilization to facilitate mobilization, reduce pulmonary complications, and manage other life-threatening injuries.
*
Nonunion or symptomatic malunion:
Late complications that may require surgical intervention.
*
Severe intractable pain:
Unresponsive to conservative measures, particularly if related to mechanical instability or nerve impingement.
Contraindications for Nonoperative Treatment (and thus indications for Operative):
*
Open injury:
Debridement is required, thus nonoperative treatment is contraindicated.
*
Progressive neurological deficit:
Indicates ongoing neural compression.
*
Significant displacement:
Loss of pelvic ring stability or persistent neural compression.
*
Associated unstable pelvic ring injuries:
Requires surgical stabilization of the entire ring.
*
Inability to manage pain or participate in rehabilitation:
Sometimes, operative stabilization can provide better pain control and allow earlier mobilization.
Contraindications for Operative Treatment:
*
Unstable medical comorbidities:
Patients unable to tolerate anesthesia or major surgery.
*
Severe local soft tissue compromise:
Making surgical access or wound closure difficult and increasing infection risk.
*
Established infection:
Requires control prior to implant placement, if possible.
*
Extensive neurological injury (e.g., complete cauda equina syndrome with long-standing paralysis):
While decompression may be considered, the likelihood of neurological recovery diminishes significantly over time, and the focus may shift to palliative care or stabilization without expectation of neurological return. This needs careful multidisciplinary discussion.
Table 1: Operative vs. Non-Operative Indications for Sacral Fractures
| Feature/Condition | Non-Operative Management (Typically A2 Nondisplaced Transverse) | Operative Management (Other Sacral Fractures) |
|---|---|---|
| Fracture Type | A2 Nondisplaced transverse, isolated Zone I or II without displacement. | Displaced transverse, vertical, U-type, H-type sacral fractures; sacral fracture-dislocations. |
| Pelvic Ring Stability | Stable posterior and anterior pelvic ring. | Unstable pelvic ring (e.g., associated symphyseal diastasis, SI joint disruption). |
| Neurological Status | Intact neurological function, low likelihood of cauda equina injury. | Progressive or significant neurological deficit (e.g., cauda equina, severe radiculopathy). |
| Displacement | Nondisplaced or minimally displaced (<5 mm). | Displacement >1 cm (translation, angulation, rotation) into sacral canal or resulting in gross instability. |
| Open Injury | Closed fracture. | Open sacral fracture. |
| Pain | Localized pain, manageable with analgesics and activity modification. | Severe, intractable pain due to mechanical instability or nerve impingement. |
| Patient Comorbidities | No contraindications for conservative care. | Medically fit for surgery. |
| Associated Injuries | Isolated sacral fracture, or stable associated injuries. | Polytrauma with need for early mobilization; other unstable pelvic or spinal injuries. |
Pre-Operative Planning & Patient Positioning
While A2 nondisplaced transverse sacral fractures are primarily managed non-operatively, robust pre-operative planning is crucial for any sacral fracture assessment, including ruling out the need for operative intervention and preparing for potential complications. For those sacral fractures requiring surgery (which, again, typically excludes A2 nondisplaced), meticulous planning is essential.
Diagnostic Imaging & Assessment:
1.
Initial Radiographs:
AP pelvis, inlet, and outlet views are standard. These provide initial assessment of pelvic ring integrity and gross sacral morphology.
2.
Computed Tomography (CT) Scan:
The gold standard for sacral fracture evaluation.
*
Axial, Coronal, Sagittal Reconstructions:
Essential to precisely define fracture lines, displacement, comminution, and sacral canal compromise.
*
3D Reconstructions:
Aid in understanding the complex fracture pattern and planning fixation.
*
Angiography (CT-A or conventional):
Indicated in cases of hemodynamic instability or suspicion of major vascular injury, particularly with high-energy trauma.
3.
Magnetic Resonance Imaging (MRI):
Crucial for evaluating soft tissue injuries, ligamentous integrity, and discerning neural impingement.
*
T1 and T2 sequences:
Assess for hematoma, edema, direct nerve root compression, and cauda equina status. This is particularly important if there's
any
concern for neurological compromise, even in an apparently nondisplaced fracture.
4.
Neurological Examination:
A thorough baseline neurological assessment (motor, sensory, perianal sensation, anal tone, bulbocavernosus reflex) is critical. Any deficit necessitates urgent investigation.
5.
Multidisciplinary Consultation:
Collaboration with neurosurgery, general surgery, urology, and interventional radiology may be necessary, especially in polytrauma or cases with associated injuries (e.g., bowel/bladder rupture, major hemorrhage).
Nonoperative Planning (for A2 Nondisplaced Transverse Fractures):
*
Pain Management Strategy:
Develop a multimodal analgesia plan, including NSAIDs, acetaminophen, neuropathic agents (gabapentin/pregabalin), and judicious use of opioids. Consider nerve blocks or epidural analgesia for severe initial pain.
*
Activity Modification:
Advise on restricted weight-bearing initially, progressing as pain allows. Avoid prolonged sitting on hard surfaces.
*
Mobility Aids:
Crutches or a walker may be needed temporarily.
*
DVT Prophylaxis:
Assess risk and initiate pharmacologic or mechanical prophylaxis as indicated.
*
Bowel/Bladder Management:
Monitor for retention or incontinence, though less common in nondisplaced fractures, it warrants attention.
*
Patient Education:
Crucial for adherence to restrictions and managing expectations for recovery.
Pre-Operative Planning (for Operative Sacral Fractures):
*
Surgical Approach Selection:
Based on fracture morphology, displacement, and associated injuries (e.g., posterior approach for tension band plating or spinopelvic fixation, percutaneous SI screw fixation for certain patterns).
*
Implant Selection:
Determine type and size of screws, plates, or rods.
*
Fluoroscopy/Navigation:
Confirm availability and plan for use during surgery.
*
Blood Management:
Type and cross-match blood, consider antifibrinolytic agents.
*
Antibiotic Prophylaxis:
Administer pre-operatively.
Patient Positioning (for Operative Sacral Fractures):
*
Prone Position:
The most common position for posterior sacral fixation.
*
Supports:
Use bolsters or a specialized surgical frame (e.g., Jackson table) to allow free abdominal excursion, reducing intra-abdominal pressure and epidural venous bleeding.
*
Padding:
Meticulous padding of pressure points (shoulders, iliac crests, knees, ankles) to prevent nerve palsies and skin breakdown.
*
Neuro-Monitoring:
Consider somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) during high-risk cases for real-time neural integrity assessment.
*
Lateral Decubitus Position:
Less common for direct sacral fixation but may be used for combined approaches or if other injuries dictate.
*
Supine Position:
Used for anterior pelvic ring fixation but rarely for sacral fixation alone.
Detailed Surgical Approach / Technique
As established, nondisplaced transverse fractures (A2) of the lower sacrum are overwhelmingly treated nonoperatively. Therefore, describing a "detailed surgical approach/technique" for this specific fracture would be incongruous with established best practices. Instead, to fulfill the requirement for an "exhaustive, high-yield surgical reference guide," this section will detail operative approaches and techniques for other types of sacral fractures where intervention is indicated, providing a comprehensive overview of sacral surgical management. It is crucial for orthopedic surgeons to understand these techniques, even if not directly applied to A2 nondisplaced fractures.
General Principles of Operative Sacral Fracture Management:
1.
Decompression (if neurological deficit present):
Release of neural elements from direct compression by fracture fragments, hematoma, or displaced bone. This is often urgent for cauda equina syndrome.
2.
Reduction:
Restoration of anatomical alignment of the sacrum and pelvic ring, particularly for displaced fractures.
3.
Stabilization:
Rigid internal fixation to maintain reduction, promote healing, and allow early mobilization.
I. Decompression of Neural Elements (for displaced fractures with neurological compromise):
*
Approach:
Typically a posterior midline approach for central sacral canal decompression.
*
Dissection:
Incise skin and subcutaneous tissue. Subperiosteal dissection of paraspinal muscles (erector spinae) from the sacrum to expose the laminae and spinous processes.
*
Laminectomy/Foraminotomy:
Careful removal of bone fragments impinging on the cauda equina or individual sacral nerve roots. This may involve partial sacral laminectomy or unroofing of the sacral foramina. High-speed burr and Kerrison rongeurs are used meticulously to avoid neural injury.
*
Dural Inspection:
If the dura is torn, repair if possible. Evacuate epidural hematoma.
*
Nerve Root Assessment:
Gently probe nerve roots to ensure free passage.
II. Reduction Techniques (for displaced sacral fractures):
*
Direct Reduction:
For overtly displaced fragments, direct manipulation with reduction clamps, bone hooks, or osteotomes can be used.
*
Indirect Reduction:
Often achieved through traction and counter-traction, or through manipulation of associated pelvic ring components (e.g., reduction of SI joint dislocation can indirectly reduce certain sacral fractures).
*
Intraoperative Imaging:
Essential (fluoroscopy, 3D imaging if available) to confirm reduction quality in multiple planes.
III. Fixation Techniques (for unstable or displaced sacral fractures):
A. Iliosacral (IS) Screw Fixation:
*
Indications:
Common for vertical sacral fractures (Denis Zone I, II), SI joint disruptions, and certain U-type/H-type fractures. Less common for transverse fractures unless there's significant associated vertical instability.
*
Patient Positioning:
Prone on a radiolucent table.
*
Approach:
Percutaneous, small incisions over the posterior iliac crest for entry point.
*
Technique:
1.
Entry Point:
Typically on the posterior ilium, aiming into the S1 or S2 body. Specific entry points vary based on sacral morphology and desired trajectory (S1 corridor is safest for first two sacral segments).
2.
Trajectory:
Screws are aimed from the posterior ilium across the SI joint into the sacral body. The S1 superior body corridor is the largest and safest. S2 corridor is smaller.
3.
Fluoroscopic Guidance:
Crucial for safe placement.
*
Inlet View:
Ensures screw is anterior to the S1/S2 neural foramen and within the sacral body, avoiding anterior cortical breach.
*
Outlet View:
Confirms cephalad/caudad trajectory and avoidance of the neural foramen.
*
Lateral View:
Essential to confirm penetration of both ilium and sacrum, and adequate depth without breaching anterior cortex.
*
Oblique Views (Teardrop, Obturator Outlet):
May be used to visualize the S1 and S2 corridors clearly.
4.
Drilling:
A guide wire is placed, followed by drilling over the wire.
5.
Screw Insertion:
Fully threaded cannulated screws are typically used. Multiple screws (e.g., 2 S1 screws, or 1 S1 and 1 S2) may be placed for enhanced stability.
*
Internervous Planes:
Percutaneous approach minimizes muscle dissection, preserving surrounding tissue.
*
Pitfalls:
Neural injury (S1, S2 nerve roots), superior gluteal artery injury, anterior cortical breach with visceral/vascular injury.
B. Trans-sacral Bar/Tension Band Plating:
*
Indications:
For certain transverse sacral fractures (e.g., Denis Zone III U-type or H-type fractures) with significant instability or kyphosis.
*
Approach:
Posterior midline incision, wide subperiosteal exposure of the sacrum and posterior ilium.
*
Technique:
1.
Exposure:
Expose posterior aspect of sacrum, SI joints, and medial iliac wings.
2.
Plate Application:
A long, thick plate (e.g., reconstruction plate, sacral plate) is contoured to the posterior sacral anatomy.
3.
Fixation:
Screws are placed bicortically into the ilium and sacral segments. The plate acts as a tension band, resisting distracting forces and maintaining reduction.
4.
Lumbar-Pelvic Fixation (Spinopelvic Fixation):
If the sacral fracture results in significant spinopelvic dissociation (e.g., U-type, H-type fractures with L5-S1 instability), fixation often extends from the lumbar spine (L4 or L5 pedicle screws) to the ilium (iliac screws or S2-alar-iliac (S2AI) screws).
*
L4/L5 Pedicle Screws:
Placed into the lumbar vertebrae.
*
S2AI Screws:
A newer technique, screws are placed into the S2 pedicle and angled into the ilium. This avoids prominent iliac crest hardware and provides a strong construct.
*
Rods:
Connect the lumbar pedicle screws to the iliac/S2AI screws, creating a rigid construct that bridges the unstable lumbosacral junction and sacrum.
C. Sacral Plating (Direct Anterior/Posterior):
*
Indications:
Less common as a primary method for sacral fractures, but may be used in conjunction with other techniques or for specific fracture patterns. Direct anterior plating of the sacral promontory for anterior sacral instability is rare. Posterior plating is more common, similar to tension band plating.
*
Approach:
Posterior midline.
*
Technique:
Plates are applied directly to the sacral body, bridging fracture lines, with screws engaging sacral segments. Often combined with iliosacral screws or spinopelvic fixation for robust constructs.
D. Anterior Pelvic Fixation (for associated anterior ring injuries):
*
Indications:
For concomitant anterior pelvic ring instability (e.g., symphyseal diastasis) with an unstable sacral fracture.
*
Technique:
Pubic symphysis plating or external fixation is performed first, which can aid in indirect reduction of the posterior pelvic ring. This then allows for more precise posterior fixation.
Crucial Considerations for All Operative Approaches:
*
Hemostasis:
The sacral region is highly vascular. Careful hemostasis is critical.
*
Neurological Monitoring:
Essential for all high-risk sacral surgeries.
*
Soft Tissue Coverage:
Adequate closure to prevent infection.
*
Intraoperative Fluoroscopy/Navigation:
Absolutely essential for accurate and safe implant placement, especially for IS screws.
Image related to Nonoperative Treatment:
This illustration broadly depicts a nonoperative care setting or patient interaction, reinforcing the nonoperative nature of A2 nondisplaced sacral fractures, which rely on conservative management and progressive mobilization rather than surgical intervention.
Complications & Management
Even with meticulous management, sacral fractures, including nondisplaced transverse types, can lead to a spectrum of complications. Understanding these and their management is crucial for optimal patient outcomes.
I. Complications of Nonoperative Management (Relevant for A2 Nondisplaced Transverse Fractures):
-
Persistent Pain:
- Incidence: Common, especially in the initial weeks to months. Local pain and tenderness can be significant and interfere with sitting, walking, and standing.
- Management: Multimodal analgesia (NSAIDs, acetaminophen, neuropathic agents, short-term opioids). Physical therapy for core strengthening and mobility. Steroid injections (e.g., caudal epidural, nerve blocks) or radiofrequency ablation if nerve irritation is suspected and localized. Consideration of a sacral corset or cushion for sitting comfort.
-
Nonunion/Delayed Union:
- Incidence: Rare for nondisplaced transverse fractures, but can occur, especially in osteoporotic patients or those with poor nutritional status.
- Management: Conservative management with extended activity restrictions. Bone stimulators (electrical or ultrasonic) may be considered. If pain is intractable and radiographic nonunion is confirmed, surgical stabilization and bone grafting might be considered.
-
Pressure Sores/Skin Breakdown:
- Incidence: Increased risk with prolonged bed rest or limited mobility, especially over the sacrum.
- Management: Regular skin inspection, repositioning, pressure-relieving mattresses, wound care. Early mobilization is key.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: Varies with patient risk factors and duration of immobility.
- Management: Pharmacological prophylaxis (low molecular weight heparin or direct oral anticoagulants) and mechanical prophylaxis (sequential compression devices) according to institutional protocols, initiated upon admission. Early ambulation is the most effective preventative measure.
-
Bowel/Bladder Dysfunction:
- Incidence: Low in truly nondisplaced fractures, but any change warrants immediate investigation. May present as constipation or urinary retention.
- Management: Bowel regimen (stool softeners, laxatives). For urinary retention, temporary catheterization may be needed. Referral to urology/gastroenterology if persistent. Neurological evaluation to rule out subtle cauda equina involvement.
-
Malunion:
- Incidence: Extremely rare for nondisplaced fractures by definition.
- Management: Typically observed if asymptomatic. Symptomatic malunion would require reconstructive surgery.
II. Complications of Operative Management (for Displaced/Unstable Sacral Fractures, not typically A2 nondisplaced):
-
Neurological Injury:
- Incidence: 1-10% depending on fracture type and surgical complexity. Can include cauda equina syndrome (new or worsened), individual sacral nerve root deficits (e.g., S1 radiculopathy from an errant IS screw).
- Management: Immediate re-evaluation with imaging (CT, MRI). Urgent surgical exploration for decompression and hardware revision/removal if impingement is confirmed. Intraoperative neuro-monitoring (SSEP, MEP) can reduce incidence.
-
Infection:
- Incidence: Superficial (2-5%), deep (1-3%). Higher in open fractures or prolonged surgeries.
- Management: Superficial infections respond to oral antibiotics and wound care. Deep infections require surgical debridement, intravenous antibiotics, and potentially hardware removal (though often delayed until fracture healing).
-
Hardware Failure (Fracture, Loosening, Pull-out):
- Incidence: Varies based on bone quality, construct rigidity, and patient activity. More common in osteoporotic bone.
- Management: Revision surgery with stronger fixation, cement augmentation, or alternative constructs. May require extended non-weight-bearing.
-
Malunion/Nonunion:
- Incidence: 5-15% for complex sacral fractures. Risk factors include severe comminution, inadequate reduction/fixation, infection, and patient comorbidities.
- Management: For symptomatic malunion or nonunion, revision surgery (osteotomy, bone grafting, re-fixation) is often required. Asymptomatic malunion may be observed.
-
Vascular Injury:
- Incidence: Rare but potentially catastrophic (e.g., superior gluteal artery injury with IS screw placement, iliac artery/vein injury).
- Management: Urgent angiographic embolization or open surgical repair. Meticulous fluoroscopic guidance during IS screw placement is critical.
-
Pain at Implant Site:
- Incidence: Common, especially with prominent hardware or irritation of nerve endings.
- Management: Analgesia, physical therapy. If persistent and debilitating, hardware removal after fracture healing is complete.
-
Heterotopic Ossification (HO):
- Incidence: Can occur after pelvic trauma and surgery, especially in the sacroiliac region.
- Management: Prophylaxis with NSAIDs or low-dose radiation in high-risk patients. Excision if symptomatic and mature.
Table 2: Common Complications of Sacral Fractures (Non-Operative & Operative)
| Complication | Incidence (Approx.) | Primary Management Strategies |
|---|---|---|
| Persistent/Intractable Pain | High (early phase) | Multimodal analgesia (NSAIDs, acetaminophen, neuropathics, opioids); physical therapy; activity modification; local injections (nerve blocks); RFA; sacral cushions. |
| Deep Vein Thrombosis (DVT) / PE | 1-5% | Pharmacological prophylaxis (LMWH, DOACs); mechanical prophylaxis (SCDs); early ambulation. |
| Pressure Sores/Skin Breakdown | 5-15% (immobilized) | Regular repositioning; pressure-relieving surfaces; meticulous skin care; early mobilization. |
| Bowel/Bladder Dysfunction | Low (<5% for A2) | Neurological reassessment; laxatives/stool softeners; temporary catheterization; specialist referral (urology/GI). |
| Neurological Deficit (new/worsened) | 1-10% (operative) | Urgent neurological reassessment; emergent CT/MRI; surgical exploration for decompression and hardware revision/removal (if operative). |
| Infection (superficial/deep) | 2-5% (superficial) | Superficial: Oral antibiotics, wound care. Deep: Surgical debridement, IV antibiotics, irrigation, potential hardware removal. |
| Hardware Failure | 5-10% (operative) | Revision surgery with stronger/alternative fixation; bone grafting; cement augmentation; extended non-weight-bearing. |
| Malunion/Nonunion | 5-15% (operative) | Symptomatic: Corrective osteotomy, re-fixation, bone grafting. Asymptomatic: Observation. (Rare for A2 nondisplaced, if so, conservative measures first, then potential surgery). |
| Vascular Injury | <1% (operative) | Urgent angiographic embolization or open surgical repair; meticulous surgical technique and imaging guidance during placement of screws (e.g., IS screws). |
| Heterotopic Ossification (HO) | 5-10% | Prophylaxis (NSAIDs, low-dose radiation) in high-risk patients; surgical excision if symptomatic and mature. |
| Pain at Implant Site | Common (operative) | Analgesia, physical therapy; hardware removal (after fracture union) if persistent and debilitating. |
This image tag, although referencing a local path, is included as requested. Its specific contextual meaning without visual content is limited, but it aligns with general recovery illustrations.
Post-Operative Rehabilitation Protocols
For nondisplaced transverse fractures (A2) of the lower sacrum, which are typically managed non-operatively, the "post-operative" phase refers to the period following the acute injury and initiation of conservative treatment. The primary goals are pain control, restoration of function, and safe return to activities of daily living (ADLs) and, eventually, sport or work.
Phase 1: Acute Pain Management & Protection (Weeks 0-2/3)
*
Goal:
Control acute pain, protect fracture healing, prevent complications of immobility.
*
Pain Management:
* Multimodal analgesia is paramount: NSAIDs (if no contraindications), acetaminophen, muscle relaxants, judicious short-term opioid use for severe pain. Neuropathic agents (gabapentin, pregabalin) may be considered if nerve irritation is suspected.
* Local pain and tenderness can be significant and interfere with sitting. Patients should be advised to avoid direct pressure on the sacrum (e.g., use a donut cushion or avoid hard seating surfaces).
*
Activity Modification:
* Initially, restricted weight-bearing as tolerated, using crutches or a walker for support. "Walking and standing as well as bed bound activities will soon become tolerable."
* Avoid prolonged sitting, twisting, or bending motions of the trunk.
* Bed mobility training: Log-rolling technique to minimize sacral torsion.
*
Physical Therapy (PT):
*
Early, gentle mobilization:
Range of motion exercises for hips, knees, and ankles to prevent stiffness and DVT.
*
Breathing exercises:
To maintain pulmonary hygiene.
*
Isometric exercises:
For gluteal and abdominal muscles (gentle core bracing) to maintain muscle tone without stressing the fracture.
*
Complication Prevention:
* DVT prophylaxis as indicated.
* Skin care: Regular inspection and repositioning to prevent pressure sores.
* Bowel regimen to prevent constipation and straining.
Phase 2: Gradual Progression & Early Strengthening (Weeks 3-8)
*
Goal:
Increase activity tolerance, improve pain-free range of motion, initiate gentle strengthening.
*
Pain Management:
Gradually wean off stronger analgesics. Continue as-needed use of NSAIDs/acetaminophen.
*
Weight-Bearing:
Progress from partial to full weight-bearing as pain allows and radiographic healing progresses (if imaging is repeated).
*
Physical Therapy:
*
Initiate gentle core and gluteal strengthening:
Pelvic tilts, bridging exercises (single and double leg), supine marches, gentle clam shells. Emphasis on neutral spine and pelvic stability.
*
Balance and proprioception exercises:
Single leg stance, tandem stance.
*
Gait training:
Normalize gait pattern without assistive devices.
*
Postural education:
Emphasize proper sitting, standing, and lifting mechanics.
*
Activity:
Gradually increase duration of sitting and standing. Begin light activities of daily living.
Phase 3: Advanced Strengthening & Return to Activity (Weeks 8-16+)
*
Goal:
Achieve full functional recovery, return to pre-injury activity levels.
*
Pain Management:
Minimal to no pain with ADLs.
*
Physical Therapy:
*
Progressive resistance exercises:
For core, gluteals, and lower extremities. Include lunges, squats, step-ups.
*
Sport-specific drills:
For athletes, gradually reintroduce running, jumping, and agility exercises.
*
Endurance training:
Walking, cycling, swimming.
*
Return to lifting:
Teach proper body mechanics for heavy lifting, emphasizing leg drive and core engagement.
*
Return to Work/Sport:
Gradual return based on functional assessment, pain levels, and fracture healing (if follow-up imaging done). Full unrestricted activity may take 3-6 months or longer.
*
Long-term considerations:
Continue a home exercise program. Address any lingering postural or movement dysfunctions.
Post-Operative Rehabilitation for Operatively Treated Sacral Fractures (General Principles,
not
A2 Nondisplaced):
The rehabilitation protocol for operatively treated sacral fractures (e.g., displaced Denis Zone II/III, unstable pelvic ring) is often more protracted and dictated by the stability of the fixation, the quality of reduction, and the presence of any neurological deficits.
*
Initial Phase (Weeks 0-6):
Often non-weight-bearing or touch-down weight-bearing on the affected side(s) to protect fixation. Focus on early bed mobility, transfer training, and gentle range of motion of unaffected joints. Strict adherence to weight-bearing restrictions is critical.
*
Intermediate Phase (Weeks 6-12):
Gradual progression to partial and then full weight-bearing as radiographic evidence of healing and clinical stability permit. More aggressive core and hip strengthening, always respecting fixation limits.
*
Advanced Phase (Weeks 12+):
Similar to Phase 3 for non-operatively treated fractures, with emphasis on progressive functional training and return to sport/work, guided by fracture healing status and surgeon's discretion. Neurological recovery, if applicable, would be a major determinant of long-term functional outcome and rehabilitation focus.
Summary of Key Literature / Guidelines
The management of sacral fractures, particularly nondisplaced transverse types, is guided by a combination of established classification systems, biomechanical principles, and clinical outcomes research.
1. Classification Systems:
*
Denis Classification (1988):
Remains a foundational system, categorizing sacral fractures based on their anatomical zone. It provides a strong correlation between fracture zone and the likelihood of neurological injury (Zone III having the highest risk). While useful for understanding injury patterns, it doesn't fully address pelvic ring stability.
*
AO/OTA Classification (2018):
Integrates sacral fractures into the broader pelvic ring injury classification (Type A, B, C). A2 sacral fractures, as discussed, are characterized as isolated, stable posterior injuries. This comprehensive system is increasingly utilized to guide treatment decisions based on stability. A Type A fracture (e.g., A2 sacral fracture) denotes a stable pelvic ring injury, which underpins the nonoperative management paradigm.
*
Isler's Classification (1990):
Specifically for lumbosacral dissociation, highlighting instability at the L5-S1 junction. While not directly for transverse sacral fractures, it emphasizes the importance of spinopelvic stability.
2. Biomechanical Studies:
* Numerous studies have elucidated the biomechanics of the pelvic ring and sacrum. They underscore the critical role of the posterior ligamentous complex (sacroiliac ligaments, sacrotuberous, sacrospinous ligaments) in pelvic stability. Nondisplaced fractures maintain this stability, while displaced or comminuted fractures compromise it, necessitating surgical intervention.
* Biomechanics also inform safe corridors for iliosacral screw placement, minimizing the risk of neurovascular injury. Studies consistently emphasize the larger S1 corridor compared to S2, and the importance of specific fluoroscopic views (inlet, outlet, lateral) for accurate screw trajectory.
3. Clinical Outcomes & Guidelines:
*
Nonoperative Management of Stable Sacral Fractures:
Current literature overwhelmingly supports nonoperative management for stable, nondisplaced sacral fractures, including A2 transverse types. Outcomes generally show good to excellent functional recovery, although protracted pain can be a challenge. The focus is on pain control, early mobilization as tolerated, and gradual return to activity. This aligns with the seed content's emphasis on nonoperative management.
* Studies by authors like Routt, Denis, and Tile consistently demonstrate that stable sacral fractures, when managed conservatively, heal well with low rates of major complications, provided there is no neurological compromise or associated pelvic ring instability.
*
Role of Imaging:
High-resolution CT scanning is universally accepted as the definitive imaging modality for sacral fractures, providing detailed fracture morphology and aiding in classification. MRI is reserved for evaluating neurological compromise or ligamentous injury, especially when clinical suspicion persists despite stable CT findings.
*
Management of Neurological Deficits:
Even minor neurological deficits (e.g., sacral radiculopathy) in sacral fractures warrant careful consideration. Progressive deficits or cauda equina syndrome are strong indications for emergent surgical decompression, irrespective of fracture stability, emphasizing the priority of neural integrity.
*
Consensus on Operative Indications:
Operative intervention for sacral fractures is typically reserved for:
* Unstable pelvic ring injuries (e.g., AO/OTA Type B or C) with sacral involvement.
* Displaced sacral fractures, particularly those with significant translation or rotation.
* Fractures with documented neurological deficits requiring decompression.
* Open fractures.
* Intractable pain due to mechanical instability.
*
Rehabilitation:
Evidence-based rehabilitation emphasizes early weight-bearing and functional mobilization for stable injuries, progressing gradually. For operatively treated unstable injuries, weight-bearing protocols are often more restrictive initially, adhering to the dictates of hardware stability.
In summary, the literature reinforces that an A2 nondisplaced transverse fracture below the S-I joint is a stable injury, typically managed nonoperatively with a good prognosis for recovery, assuming close monitoring for neurological status and effective pain management. Surgical intervention is reserved for more complex, unstable, or neurologically compromising sacral fracture patterns.
