Identify A1 Fractures: A Coccygealsacral Guide
Introduction & Epidemiology
A1 fractures, within the AO/OTA classification system for sacrococcygeal injuries, refer specifically to coccygeal/sacral compression fractures or ligamentous avulsion fractures . These represent relatively stable, often low-energy patterns affecting the distal sacrum (typically S3-S5 segments) or the coccyx. Understanding the nuances between compression and avulsion, and their implications for clinical management, is paramount.
Compression fractures of the coccyx or distal sacrum typically result from a direct axial load, such as a fall onto the buttocks. The mechanism involves impaction, leading to either a transverse fracture line or comminution, often with anterior angulation of the distal fragment. Ligamentous avulsion fractures, conversely, occur when strong ligamentous attachments, such as the sacrococcygeal ligaments or attachments of the levator ani or gluteus maximus muscles, pull off a small fragment of bone from their insertion points. While less common for the coccyx itself, avulsion injuries can occur at the sacrococcygeal joint or the superior aspect of the coccyx where robust ligaments attach.
The incidence of coccygeal fractures is not precisely documented due to the frequent under-reporting and conservative management of these injuries. However, coccydynia, a symptom often associated with these fractures, is estimated to affect approximately 1% of the population, with a female-to-male predominance of 5:1. This gender disparity is partly attributed to anatomical differences in pelvic shape and the biomechanical stresses associated with childbirth. While A1 fractures are generally considered stable, their impact on patient quality of life can be significant due to chronic pain, termed coccydynia. Associated injuries are rare with isolated A1 fractures but can include soft tissue contusions, hematomas, or in high-energy trauma, other pelvic or spinal injuries. Initial assessment requires a thorough history focusing on mechanism of injury and symptom onset, followed by a meticulous physical examination including inspection, palpation of the coccyx, and potentially a rectal examination to assess coccygeal mobility and exclude other pathologies. Radiographic evaluation typically begins with AP and lateral plain radiographs of the coccyx and sacrum. Dynamic lateral views (flexion and extension) can be invaluable in assessing instability of the sacrococcygeal joint or an angulated coccygeal fracture. Computed tomography (CT) scans with 3D reconstructions are reserved for cases with equivocal plain radiographs, suspected displacement, or when surgical intervention is contemplated, providing superior bony detail. Magnetic resonance imaging (MRI) is less commonly used for pure A1 fractures but can be helpful in identifying soft tissue involvement, ligamentous injuries, or excluding other causes of coccydynia such as tumors or disc pathology.
Surgical Anatomy & Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the sacrococcygeal region is essential for the effective management of A1 fractures, particularly when considering surgical intervention.
Osseous Anatomy
The sacrum is a large, triangular bone forming the posterior wall of the pelvis, articulating superiorly with L5 and inferiorly with the coccyx. For A1 fractures, the focus is typically on the distal sacral segments (S3-S5), which are often partially or completely fused. These segments possess rudimentary transverse processes and contribute to the formation of the sacral hiatus. The coccyx (tailbone) is a small, triangular bone typically composed of 3 to 5 fused or partially fused rudimentary vertebrae. Its apex points inferiorly and anteriorly, and its base articulates with the apex of the sacrum via the sacrococcygeal joint. Anatomical variations in the number of coccygeal segments, degree of fusion, and inherent angulation are common and should be noted during pre-operative assessment.
Ligamentous Anatomy
The stability of the sacrococcygeal joint and the coccyx itself is heavily reliant on a complex network of ligaments:
*
Sacrococcygeal Ligaments:
*
Anterior Sacrococcygeal Ligament:
A continuation of the anterior longitudinal ligament, contributing to anterior stability.
*
Posterior Sacrococcygeal Ligaments:
Superficial and deep layers, analogous to the posterior longitudinal and ligamentum flavum, respectively. These are crucial in preventing posterior displacement.
*
Lateral Sacrococcygeal Ligaments:
Connect the transverse processes of the coccyx to the inferior lateral angle of the sacrum, providing lateral stability.
*
Anococcygeal Ligament (or Raphe):
A fibrous band extending from the coccyx to the external anal sphincter, providing support to the anorectal junction. Its integrity is critical for pelvic floor function.
*
Sacrotuberous and Sacrospinous Ligaments:
While primarily connecting the sacrum to the ischial tuberosity and spine, respectively, and thus more proximal, they contribute to overall pelvic stability and indirect forces on the coccyx. Avulsion injuries (A1) specifically involve the detachment of one of these bony insertions, often with a small bone fragment.
Muscular Attachments
Several muscles attach to the coccyx, contributing to its stability and function, and are important during surgical dissection:
*
Gluteus Maximus:
Its most inferior fibers insert onto the lateral aspect of the coccyx.
*
Levator Ani Muscles (Pubococcygeus, Iliococcygeus, Puborectalis):
These muscles form a significant portion of the pelvic floor, with the coccygeal muscle inserting onto the lateral margins of the coccyx. They play a vital role in supporting pelvic viscera and continence.
*
Coccygeus Muscle:
Courses from the ischial spine to the lateral margins of the sacrum and coccyx, synergistically supporting the pelvic floor.
*
External Anal Sphincter:
Attaches anteriorly to the coccyx via the anococcygeal ligament. Its proximity mandates careful dissection.
Neurovascular Anatomy
- Nerves: The sacral nerve roots (S3-S5) and the coccygeal nerve plexus (comprising S5 and coccygeal nerves) provide sensory and motor innervation to the perineum, pelvic floor, and perianal region. Damage to these nerves can lead to perineal numbness, bowel/bladder dysfunction, or persistent neuropathic pain. The pudendal nerve (S2-S4) runs inferior to the sacrospinous ligament and is a significant structure to avoid injury to during deep dissection.
- Vessels: The median sacral artery descends anterior to the sacrum, while the lateral sacral arteries course laterally. While larger vessels are more proximal, careful hemostasis is required during coccygeal dissection due to numerous smaller venous plexuses.
Biomechanics
The coccyx serves several important biomechanical functions:
*
Weight-Bearing:
It acts as a posterior point of support in the sitting position, distributing weight with the ischial tuberosities.
*
Shock Absorption:
Its inherent flexibility and the sacrococcygeal joint allow for some degree of motion, absorbing forces transmitted through the spine.
*
Pelvic Floor Support:
It provides an anchoring point for several pelvic floor muscles and ligaments, crucial for continence and pelvic organ support.
A1 compression fractures typically result from direct axial loading, causing the coccyx to buckle anteriorly. Avulsion fractures occur when abrupt tensile forces exceed the strength of the bone-ligament interface. Disruption of these structures leads to instability, abnormal motion, and irritation of surrounding soft tissues and nerves, manifesting as coccydynia. The integrity of the sacrococcygeal joint is vital; excessive anterior angulation or posterior dislocation can impinge on the pelvic floor structures and nerves.
Indications & Contraindications
The management of A1 coccygeal/sacral fractures is predominantly non-operative. Surgical intervention is reserved for a select group of patients with specific indications, following failed conservative treatment.
Non-Operative Indications
- Stable Fracture Patterns: Most A1 compression or avulsion fractures are inherently stable with minimal displacement or angulation.
- Minimal Displacement/Angulation: Even if fractured, if the overall alignment and integrity of the pelvic floor are maintained, conservative care is preferred.
- Absence of Neurological Deficit: Pure A1 fractures are rarely associated with acute neurological deficits, but their absence reinforces non-operative management.
- Acute Pain Amenable to Conservative Management: Initial treatment for virtually all A1 fractures involves a multimodal conservative approach.
Operative Indications
Operative intervention, most commonly coccygectomy, is considered only after a prolonged trial of conservative management has failed to alleviate intractable symptoms.
*
Persistent, Intractable Coccydynia:
This is the primary indication, defined as severe pain lasting typically >6 months, refractory to at least two distinct, adequately administered conservative modalities (e.g., NSAIDs, activity modification, donut cushions, physical therapy, local injections).
*
Gross Instability of the Coccyx/Sacrococcygeal Joint:
Demonstrated on dynamic lateral radiographs (excessive motion >25 degrees or >25% posterior subluxation during sitting). This instability causes repetitive microtrauma and inflammation.
*
Significant Displacement Leading to Impingement:
Although rare for isolated A1 fractures, a severely angulated or displaced fragment that persistently impinges on adjacent neural or soft tissue structures can warrant excision.
*
Fracture Non-Union or Symptomatic Malunion:
A painful fibrous non-union or a malunited coccyx with severe anterior angulation causing pressure on underlying structures.
*
Associated Neurological Deficit:
Extremely rare for A1 coccygeal fractures but theoretically possible if a fragment causes direct nerve compression. More common with higher energy sacral fractures.
*
Open Fractures:
While exceedingly rare for coccygeal fractures, any open fracture in this region necessitates surgical débridement and possible fixation/excision depending on contamination and tissue loss.
*
Infection:
In rare instances, a chronic osteomyelitis or abscess involving the fractured segment may necessitate surgical debridement or excision.
Contraindications
- Active Local or Systemic Infection: Relative contraindication; surgery should be delayed until infection is controlled.
- Uncontrolled Coagulopathy: Increases risk of bleeding complications.
- Severe Comorbidities Precluding Surgery: ASA Class III or IV patients with unmanaged cardiac, pulmonary, or other systemic diseases where the risk of surgery outweighs the potential benefit.
- Patient Refusal: Autonomy of the patient.
- Unrealistic Expectations or Significant Psychological Factors: Patients with somatization disorders, significant secondary gain, or unrealistic expectations of complete pain relief often fare poorly post-operatively. A thorough psychological evaluation may be warranted in select cases.
- Lack of Clearly Identifiable Etiology: If coccydynia is not clearly attributable to the fracture, or if multiple pathologies exist, surgical outcomes may be unpredictable.
Summary of Operative vs. Non-Operative Indications
| Feature | Non-Operative Management | Operative Management (Coccygectomy) |
|---|---|---|
| Fracture Type | Stable A1 compression or avulsion, minimal displacement/angulation. | Unstable A1 (dynamic radiographs), symptomatic non-union/malunion, gross displacement/impingement. |
| Symptom Duration | Acute or subacute pain (<6 months). | Chronic intractable coccydynia (>6 months). |
| Conservative Treatment | Initial treatment for all patients. | Failed extensive, multimodal conservative therapy (e.g., injections, PT, NSAIDs, cushions). |
| Neurological Deficit | Absent. | Rarely, associated with a focal neurological deficit attributable to bony impingement. |
| Pain Severity | Mild to moderate, responsive to conservative measures. | Severe, disabling pain significantly impacting quality of life. |
| Comorbidities | Manageable; patient medically stable for non-invasive approaches. | Patient medically fit for surgery; risks outweighed by potential benefits. |
| Patient Expectation | Realistic, understanding that pain may resolve gradually. | Realistic, understanding of potential complications and variability in outcome. |
| Imaging Findings | Fracture visible, but no gross instability or critical impingement. | Clear radiographic evidence of unstable fracture, sacrococcygeal joint hypermobility, or severe angulation. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical to optimize surgical exposure, minimize complications, and ensure a successful outcome for patients undergoing surgical management of A1 coccygeal/sacral fractures, typically coccygectomy.
Pre-Operative Workup
- Detailed History and Physical Examination: Reconfirm intractable coccydynia, document duration, failed conservative treatments, and assess for any neurological deficits (e.g., perianal numbness, bowel/bladder dysfunction, although rare for A1). Assess skin integrity in the gluteal cleft for any pre-existing lesions or infections.
-
Imaging Review:
- Plain Radiographs: AP and true lateral views of the coccyx. Essential for confirming the fracture and assessing angulation.
- Dynamic Lateral Views: Critical for demonstrating instability (e.g., hypermobility or subluxation of the sacrococcygeal joint, or increased fracture angulation with sitting). These views often clinch the decision for surgery.
- CT Scan (if indicated): Provides detailed bony anatomy, identifies comminution or displacement, and helps delineate the relationship to the sacrum. Useful for defining the precise level of planned osteotomy.
- MRI (less common for A1): Primarily used to rule out soft tissue pathologies, tumors, or disc herniation mimicking coccydynia, and to assess for significant inflammation or neuropathy.
- Anesthetic Clearance: Routine pre-anesthetic evaluation to assess patient's fitness for general anesthesia and identify any co-morbidities that may influence surgical risk.
- Informed Consent: Comprehensive discussion with the patient regarding the proposed procedure, expected outcomes, potential complications (e.g., infection, wound dehiscence, persistent pain, nerve injury, rectal perforation), and rehabilitation expectations. It is imperative to manage patient expectations regarding complete pain relief.
Instrumentation & Equipment
- Standard Orthopedic Major Tray: Basic surgical instruments.
- Small Bone Instruments: Osteotomes (various sizes), mallet, small rongeurs (Kerrison, Leksell), bone-holding clamps.
- Power Tools: Small oscillating or reciprocating saw with fine blades (e.g., sagittal saw) for precise osteotomy.
- Fluoroscopy: Intraoperative C-arm fluoroscopy is highly recommended to confirm the level of osteotomy, especially when dealing with the sacrococcygeal joint or distal sacral fractures.
- Diathermy/Bipolar Cautery: For meticulous hemostasis.
- Suture Material: Absorbable for deep layers (e.g., 2-0 or 0 Vicryl), non-absorbable for skin (e.g., 3-0 or 4-0 Nylon).
- Wound Drainage: Closed suction drain (e.g., ¼ inch Penrose or small Hemovac) may be considered, especially in obese patients or those with significant dead space.
Patient Positioning
- Anesthesia: General endotracheal anesthesia is typically employed.
- Prone Position: This is the standard position for coccygeal surgery, providing excellent exposure of the sacrococcygeal region and gluteal cleft.
-
Padding and Support:
- Chest Rolls/Bolsters: Placed longitudinally along the torso, extending from the clavicles to the iliac crests, to support the chest and pelvis. This allows the abdomen to hang freely, minimizing compression of the inferior vena cava, reducing intra-abdominal pressure, and facilitating venous return, thereby decreasing intraoperative bleeding.
- Pillows/Gel Pads: Under the knees and ankles to prevent pressure points (e.g., peroneal nerve palsy, foot drop).
- Head Support: A donut headrest to protect facial structures and maintain neutral cervical alignment.
- Hip Position: Hips should be slightly flexed to open the gluteal cleft and facilitate exposure of the coccyx. This can be achieved by placing a small bolster under the hips or by flexing the operating table.
- Preparation for Draping: Ensure the entire gluteal region, including the perianal area and distal sacrum, is accessible. The anus should be excluded from the sterile field with an impervious drape.
-
Surgical Site Preparation:
- The area is prepped with an antiseptic solution (e.g., povidone-iodine or chlorhexidine-alcohol scrub) extending from the mid-back to the mid-thigh, laterally to both greater trochanters.
- A sterile impervious drape is applied to isolate the anal region, followed by standard surgical draping to expose the sacrococcygeal area.
Detailed Surgical Approach / Technique
Surgical intervention for A1 coccygeal/sacral fractures primarily involves coccygectomy, particularly for symptomatic, unstable coccygeal compression or avulsion injuries refractory to conservative management. The approach emphasizes meticulous dissection and preservation of perianal structures.
Anesthesia and Initial Preparation
- General Endotracheal Anesthesia: Standard.
- Antibiotic Prophylaxis: Administer intravenous antibiotics (e.g., cefazolin) prior to incision.
- Foley Catheter: Generally not required for routine coccygectomy unless prolonged surgery or specific patient comorbidities dictate.
Incision
- Location: A midline longitudinal incision is made directly over the spinous processes of the distal sacrum and coccyx. The incision should be centered over the intended osteotomy site or the most prominent point of the fractured/dislocated coccyx.
- Length: Typically 5-8 cm, extending sufficiently to allow adequate exposure proximally to the sacrococcygeal joint and distally to the tip of the coccyx.
- Skin and Subcutaneous Tissue: The incision is carried through the skin and subcutaneous fat. Careful hemostasis is maintained with electrocautery.
Dissection
- Identification of Anococcygeal Raphe: The anococcygeal raphe (or ligament) is a key anatomical landmark that lies deep to the subcutaneous fat, connecting the coccyx to the external anal sphincter. It must be sharply incised in the midline.
-
Subperiosteal Dissection:
- Using sharp dissection and periosteal elevators (e.g., Cobb elevator), the muscular attachments are carefully detached subperiosteally from the lateral and anterior surfaces of the coccyx and distal sacrum.
- Muscles to Detach: The fibers of the gluteus maximus (laterally), levator ani and coccygeus muscles (laterally and anteriorly), and attachments of the external anal sphincter are meticulously stripped off the bone.
- Crucial Consideration: This dissection must be kept strictly subperiosteal to minimize damage to the muscle bellies and, more importantly, to protect the underlying rectal wall and the delicate sacral nerve roots and neurovascular structures. The anterior surface of the coccyx is intimately related to the rectum and presacral venous plexus, requiring extreme caution.
-
Visualization of the Fracture/Joint: Continue dissection until the entire coccyx and the sacrococcygeal joint are clearly visualized.
- Identify the fracture site in an A1 compression fracture, or the avulsed fragment in an A1 ligamentous avulsion.
- Assess the stability and degree of displacement.
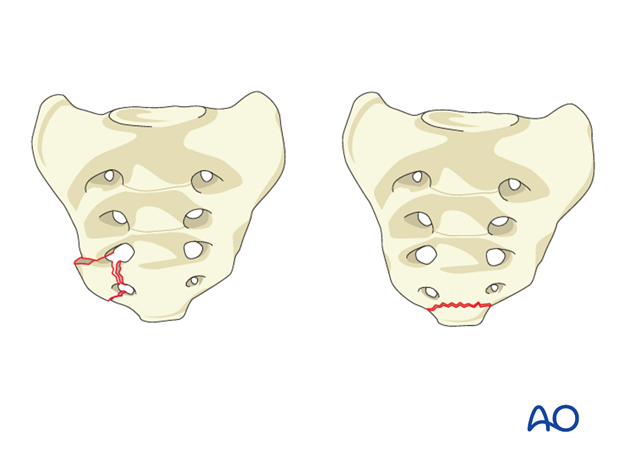
This intraoperative schematic illustrates the distal sacrum and coccyx, highlighting the typical location of A1 compression or avulsion fractures at the sacrococcygeal junction or within the coccygeal segments.
Specific Techniques
For A1 Compression Fractures or Unstable Displacements (Coccygectomy)
- Osteotomy Planning: The decision on whether to remove the entire coccyx or just the fractured segment is made pre-operatively. For most intractable coccydynia cases related to A1 fractures, total coccygectomy or excision of the mobile/fractured segment is performed. The osteotomy is typically performed at the sacrococcygeal joint to excise the entire coccyx, or just proximal to the fracture line.
- Fluoroscopy: Utilize intraoperative fluoroscopy to confirm the precise level of the sacrococcygeal joint or the intended osteotomy site within the coccygeal segments, ensuring complete removal of the pathological segment.
-
Osteotomy:
- Using a fine oscillating saw or sharp osteotome and mallet, perform a clean transverse osteotomy at the chosen level. Ensure the cut is perpendicular to the long axis of the bone.
- Anterior Protection: Crucially, a broad periosteal elevator or a small malleable retractor should be placed anterior to the coccyx/sacrum to protect the rectum during the osteotomy.
- Carefully detach any remaining anterior ligamentous or muscular attachments to free the fractured segment or entire coccyx.
- Fragment Removal: Once completely freed, the fractured coccyx or segment is removed. Inspect the raw bony surface and surrounding soft tissues for any remaining spicules or sharp edges, which should be smoothed with a rongeur or bone file.
For A1 Ligamentous Avulsion Fractures (if requiring fixation - rare for this category)
While most A1 avulsion fractures are managed conservatively, if a large, displaced fragment is the cause of intractable pain and is amenable to repair, the technique would involve:
1.
Fragment Identification:
Clearly identify the avulsed bony fragment and the associated ligamentous tissue.
2.
Reduction:
Gently reduce the fragment to its anatomical position.
3.
Fixation (if applicable):
* If the fragment is sufficiently large, small lag screws or tension band wiring might be considered, though this is technically challenging given the small size of the coccyx and potential for hardware prominence.
* More commonly, suture anchors placed into the coccyx can be used to re-attach the avulsed ligamentous complex. This is often debated due to the high stress environment and risk of re-avulsion. In most cases, if an avulsion fracture is symptomatic, coccygectomy is often a more reliable option for definitive pain relief.
Wound Closure
- Hemostasis: Ensure meticulous hemostasis of all bleeding vessels.
- Irrigation: Copious irrigation of the wound with sterile saline.
- Drain Placement: A small closed-suction drain may be placed in the deep wound cavity, particularly in obese patients or if significant dead space exists, to prevent hematoma and seroma formation. The drain is typically brought out through a separate stab incision.
-
Layered Closure:
- Re-approximate the detached pelvic floor muscles and fascia over the raw sacral surface using absorbable sutures (e.g., 0 or 2-0 Vicryl). This helps obliterate dead space and reconstruct the pelvic floor.
- Close the subcutaneous tissue in layers with absorbable sutures (e.g., 2-0 or 3-0 Vicryl).
- Close the skin with non-absorbable sutures (e.g., 3-0 or 4-0 Nylon) or staples. Special attention is paid to a tension-free closure, especially in the gluteal cleft.
Post-Closure
- Sterile Dressing: Apply a sterile occlusive dressing.
- Anal Exclusion: Emphasize strict wound care and anal hygiene in the post-operative period to prevent contamination.
Complications & Management
Despite meticulous surgical technique, complications can arise following surgery for A1 coccygeal/sacral fractures, particularly after coccygectomy. Anticipation and prompt management are crucial for optimal outcomes.
Common Complications
| Complication | Incidence (Approximate) | Management / Salvage Strategies |
|---|---|---|
| Wound Infection | 5-15% (can be higher) | Superficial: Oral antibiotics, local wound care, daily dressings. Deep: IV antibiotics guided by culture, surgical débridement, wound irrigation, primary or delayed primary closure; may require negative pressure wound therapy. Consider wide débridement if osteomyelitis. Prophylactic antibiotics are standard. |
| Wound Dehiscence | 5-10% | Partial: Local wound care, protective dressings, off-loading pressure (donut cushion). Complete: May require surgical débridement, re-closure, or wound care with packing until secondary closure is feasible. Address underlying factors like infection, excessive tension, or hematoma. |
| Persistent Pain / Coccydynia | 10-30% | Multifactorial. Thorough re-evaluation: Rule out residual bone fragment, heterotopic ossification, nerve entrapment, psychological factors, or alternative diagnoses. Management: Pain clinic referral (injections, nerve blocks, neuromodulation), physical therapy, ergonomic adjustments, psychological support. Revision surgery (e.g., further excision of bone spurs, neurolysis) is rarely indicated. |
| Hematoma / Seroma | 5-10% | Small: Observation, aspiration if symptomatic or growing. Large: Surgical evacuation, irrigation, and re-closure with drain placement. Meticulous intraoperative hemostasis is key. |
| Nerve Injury | <1% (rare) | Perineal Numbness: Usually transient; observation, neuropathic pain medication if bothersome. Bowel/Bladder Dysfunction: Urgent neurological evaluation, MRI to rule out sacral nerve root injury. May require long-term conservative management, urology/gastroenterology referral. Rare for coccygectomy alone, more associated with high sacral fractures. |
| Rectal Perforation | <0.5% (very rare) | Immediate recognition (intraoperative): Primary repair (double-layer closure), proximal diverting colostomy (often temporary), copious irrigation, broad-spectrum antibiotics. Delayed recognition: Surgical exploration, débridement, repair, diverting colostomy, extensive antibiotics, management of sepsis. This is a surgical emergency. |
| Heterotopic Ossification (HO) | 2-5% | Symptomatic HO: Local excision if causing impingement or pain after skeletal maturity. Prophylaxis (for high-risk patients): NSAIDs or radiation post-op, though not routinely used for coccygectomy. |
| DVT / PE | <1% (low risk) | Prophylaxis: Early mobilization, mechanical compression devices. Treatment: Anticoagulation (LMWH, oral anticoagulants). Routine pharmacological prophylaxis is often not indicated for isolated coccygectomy but should be considered in high-risk patients based on institutional guidelines. |
| Sacral Non-Union / Malunion (if not excised) | Varies, can contribute to chronic pain | If the A1 fracture was managed with fixation (rare) and failed, or if an A1 sacral fracture persists with pain: Re-fixation: May involve more robust internal fixation. Excision of symptomatic non-union/malunion: If feasible and related to coccygeal segments. Often challenging. |
Management Principles
- Prevention: The best management is prevention. This includes meticulous surgical technique, strict aseptic precautions, judicious hemostasis, careful handling of tissues, and attention to proper layered wound closure to minimize dead space.
- Early Recognition: High index of suspicion for complications post-operatively.
- Aggressive Treatment: Prompt and appropriate intervention, whether medical or surgical, is crucial to mitigate morbidity and improve patient outcomes.
- Multidisciplinary Approach: For chronic or complex complications (e.g., persistent pain, bowel/bladder dysfunction), a multidisciplinary team including pain specialists, physical therapists, urologists, colorectal surgeons, and psychologists may be beneficial.
- Patient Counseling: Ongoing communication with the patient regarding the nature of complications and the plan for management.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following surgery for A1 coccygeal/sacral fractures, predominantly coccygectomy, is crucial for optimizing functional recovery, minimizing residual pain, and preventing long-term complications. The protocol progresses through acute, subacute, and long-term phases.
Acute Phase (0-2 Weeks Post-Op)
Goals:
* Pain control.
* Wound healing.
* Minimize complications (e.g., infection, wound dehiscence).
* Protect surgical site.
Key Interventions:
*
Pain Management:
* Scheduled oral analgesics (e.g., NSAIDs, acetaminophen) and opioid pain relievers as needed.
* Nerve blocks (e.g., caudal epidural, ganglion impar block) may be considered for severe post-operative pain.
*
Wound Care:
* Keep the surgical site clean and dry.
* Daily inspection for signs of infection (redness, swelling, discharge) or dehiscence.
* Change dressings as prescribed. Educate patient on proper hygiene, especially after bowel movements.
* Drain removal typically within 24-48 hours once output is minimal (<30-50 mL/24h).
*
Activity Modification:
*
Sitting:
STRICT avoidance of direct sitting on the buttocks for the initial 1-2 weeks. Patients should lie on their side or abdomen. When sitting becomes necessary, use a specialized coccygeal cushion (donut cushion, wedge cushion) to offload pressure from the surgical site.
*
Mobility:
Early ambulation encouraged to prevent DVT and maintain general fitness. Avoid strenuous activities.
*
Bowel Management:
Stool softeners and a high-fiber diet to prevent constipation and straining during defecation, which can stress the healing wound.
*
Physical Therapy (PT) – Initial Phase:
* Gentle, non-weight-bearing perineal isometric contractions (pelvic floor muscle activation) to improve circulation and promote healing, without stressing the incision.
* Deep breathing exercises.
Subacute Phase (2-6 Weeks Post-Op)
Goals:
* Gradual increase in activity tolerance.
* Improve strength and flexibility.
* Continue pain management.
Key Interventions:
*
Gradual Sitting:
Begin gradual, short periods of sitting (15-30 minutes) using a coccygeal cushion. Progress duration as tolerated.
*
Physical Therapy:
*
Pelvic Floor Strengthening:
Progressed exercises for levator ani and external anal sphincter. Biofeedback may be used to ensure proper muscle activation.
*
Core Stability:
Initiate gentle core strengthening exercises (transversus abdominis, multifidus) to support the pelvis and spine.
*
Stretching:
Gentle stretching of gluteal muscles and hip flexors to restore flexibility, avoiding direct pressure on the coccygeal region.
*
Posture Education:
Emphasis on proper sitting posture and ergonomic adjustments.
*
Activity Progression:
Gradually increase walking distance and duration. Avoid heavy lifting, impact activities, and direct pressure on the coccyx.
*
Scar Management:
Gentle massage of the incision site once wound is fully closed to prevent adhesions and improve pliability.
Rehabilitation Phase (>6 Weeks Post-Op)
Goals:
* Progressive return to full activity.
* Resolve residual pain and dysfunction.
* Long-term self-management strategies.
Key Interventions:
*
Advanced Physical Therapy:
* Progress to more advanced core and hip strengthening exercises.
* Sport-specific rehabilitation as appropriate.
* Manual therapy for any residual myofascial pain or stiffness in the gluteal or lumbar regions.
* Addressing any compensatory movement patterns developed due to pain.
*
Return to Activity:
* Gradual return to recreational and occupational activities. High-impact sports or activities involving direct sitting trauma (e.g., cycling) should be introduced cautiously and may require continued use of specialized cushions.
* Work hardening programs if required for return to demanding occupations.
*
Long-Term Considerations:
*
Ergonomics:
Continued use of ergonomic aids (cushions) as needed, especially for prolonged sitting.
*
Self-Management:
Empower patients with strategies for managing flare-ups, including stretching, icing, and activity modification.
*
Psychological Support:
Address any persistent chronic pain or fear-avoidance behaviors through cognitive behavioral therapy (CBT) or pain psychology, if indicated.
*
Follow-up:
Regular follow-up appointments with the surgeon to monitor progress and address any concerns. Radiographs are generally not required unless there is a specific concern for recurrence or complication.
The duration of rehabilitation varies significantly among individuals, but a full recovery often takes 3-6 months, with some patients experiencing mild residual discomfort for up to a year. Patient adherence to the protocol and realistic expectations are paramount for a successful outcome.
Summary of Key Literature / Guidelines
The literature concerning the management of A1 coccygeal/sacral fractures, particularly isolated coccygeal injuries, is extensive but often consists of smaller case series and retrospective studies rather than large-scale randomized controlled trials. This reflects the relatively uncommon nature of surgical intervention and the predominance of conservative management.
Classification Systems
- AO/OTA Classification: While primarily used for more complex sacral and pelvic ring injuries, the AO/OTA classification provides a structured framework for all spinal injuries. A1 coccygeal/sacral fractures denote stable injuries of the distal sacrum or coccyx, emphasizing compression or ligamentous avulsion patterns. This distinction helps guide initial decision-making regarding stability.
- Sub-classifications for Coccydynia: Numerous classifications exist for coccydynia and coccygeal morphology (e.g., Postacchini and Massobrio's classification based on coccygeal morphology and mobility). While not directly classifying fractures, these are relevant for understanding the underlying pathology driving symptoms from A1 fractures, particularly instability and hypermobility.
Evidence for Surgical vs. Non-Surgical Management
- Non-Operative Management: The overwhelming consensus in the literature supports conservative management as the first-line treatment for nearly all A1 coccygeal fractures. Studies by Wray et al. (1991), Trollegaard et al. (2002), and others consistently report high success rates (70-90%) with non-operative modalities, including NSAIDs, activity modification, specialized cushions, physical therapy, and local corticosteroid injections. The efficacy of steroid injections around the coccyx or at the ganglion impar is well-documented in reducing pain temporarily, offering diagnostic and therapeutic value.
-
Operative Management (Coccygectomy):
Coccygectomy is reserved for patients with intractable coccydynia refractory to prolonged conservative therapy (typically >6 months).
- Outcomes: Multiple studies (e.g., Doursounian et al., 2004; Perkins and Howell, 2012) report good to excellent pain relief in 60-90% of patients undergoing coccygectomy for chronic coccydynia, including those with unstable fractures or hypermobility. Factors influencing success include patient selection, duration of symptoms, and presence of dynamic instability.
- Indications: Key indications supported by literature include clear evidence of coccygeal hypermobility, instability, or severe angulation on dynamic radiographs, and failure of at least two conservative treatment modalities.
- Complications: While generally effective, coccygectomy is associated with a notable complication rate, particularly wound infection and dehiscence (5-15%), and persistent pain (10-30%). These rates are higher than many elective orthopedic procedures, partly due to the anatomical location and proximity to the perianal region. Careful surgical technique, meticulous hemostasis, and layered closure are emphasized to mitigate these risks.
Landmark Studies and Systematic Reviews
- Wray et al. (1991): Classic paper establishing the efficacy of conservative management and the role of coccygectomy for intractable cases.
- Doursounian et al. (2004) and Perkins and Howell (2012): Reviews and case series on coccygectomy outcomes, highlighting factors predicting success and common complications. They underscore the importance of dynamic radiography for patient selection.
- Systematic Reviews on Coccydynia Management: Several contemporary systematic reviews (e.g., Lin et al., 2020) continue to confirm the effectiveness of non-operative measures for most patients and identify coccygectomy as a viable option for carefully selected individuals with chronic, severe, and refractory pain, often related to instability or fracture. These reviews consistently point to wound complications as the most common adverse events.
Ongoing Research and Controversies
- Role of Injections: The long-term efficacy and ideal type (steroid, local anesthetic, botox, PRP) of injections remain areas of ongoing research.
- Fixation vs. Excision: For unstable A1 coccygeal fractures, the debate between internal fixation (e.g., small plates/screws) and coccygectomy often favors excision due to the small bone size, potential for hardware prominence, and the excellent results with coccygectomy in selected cases. Fixation of coccygeal fractures is rarely reported and often technically challenging.
- Predictors of Outcome: Identifying robust pre-operative predictors of successful surgical outcome beyond dynamic instability continues to be an area of interest to further refine patient selection.
- Minimally Invasive Approaches: While open coccygectomy is standard, exploration of minimally invasive techniques is nascent, but challenging given the anatomical constraints and need for meticulous soft tissue handling.
In summary, A1 coccygeal/sacral fractures primarily require a thoughtful, stepwise approach beginning with comprehensive non-operative management. Surgical intervention, typically coccygectomy, is a proven salvage procedure for a carefully selected cohort of patients with chronic, intractable pain, often related to instability or symptomatic non-union/malunion, following a failed extended course of conservative treatment. A thorough understanding of anatomy, biomechanics, and potential complications is vital for any surgeon considering this procedure.
