Patient Presentation & History
A 25-year-old male competitive amateur soccer player presented to the emergency department following a non-contact decelerating injury during a match. He reported planting his right foot to change direction rapidly, experiencing a sudden valgus force to his right knee, followed by a distinct "pop" sensation and immediate onset of severe pain. He was unable to bear weight and subsequently collapsed on the field. The patient described rapid swelling of the knee joint within the first hour post-injury. He denied any direct impact to the knee.
Past medical history was notable for well-controlled asthma, with no history of previous knee injuries or surgical interventions. He was physically active, regularly participating in high-impact sports, and had no known ligamentous laxity or connective tissue disorders. Social history included occasional alcohol consumption and no tobacco use. Review of systems was otherwise unremarkable. He was brought to the emergency department via ambulance, where initial X-rays were performed.
Clinical Examination
Upon initial assessment, the patient was in acute distress with significant pain.
*
Inspection:
The right knee demonstrated a tense, large effusion with diffuse swelling. Mild ecchymosis was noted around the medial and lateral aspects of the knee joint. No gross deformity was evident, but a subtle recurvatum was noted compared to the contralateral limb when fully extended.
*
Palpation:
Diffuse tenderness was elicited around the joint line, particularly over the medial and lateral collateral ligaments, the fibular head, and the anteromedial and anterolateral joint lines. A patellar ballotement test was positive, confirming the large effusion.
*
Range of Motion (ROM):
Active range of motion was severely restricted due to pain and effusion, from approximately 10° of flexion to 70° of flexion. Passive ROM was similarly restricted, with painful apprehension at extremes. Full extension was not achieved, exhibiting a 10° flexion contracture.
*
Ligamentous Stability:
Due to guarding and significant pain, a comprehensive ligamentous assessment was challenging.
*
Anterior Cruciate Ligament (ACL):
The
Lachman test
, performed with the patient supine and the knee flexed to 20-30°, initially demonstrated a firm but increased anterior translation with a soft endpoint compared to the contralateral knee, suggesting an ACL tear. However, the degree of anterior translation felt less than expected for a complete ACL rupture given the mechanism. An
Anterior Drawer test
at 90° of flexion was also positive but again, the endpoint was ambiguous due to guarding. A
Pivot Shift test
was unable to be performed adequately due to pain and muscle spasm.
*
Posterior Cruciate Ligament (PCL):
A subtle
posterior sag sign
was noted when the hips and knees were flexed to 90°, indicating possible posterior tibial translation. The
Posterior Drawer test
at 90° was positive with grade II laxity, but the endpoint was firm, suggesting a partial tear or a combined injury. The
Quadriceps Active Test
showed minimal anterior translation of the tibia, further confounding the PCL assessment.
*
Medial Collateral Ligament (MCL):
A
valgus stress test
at 30° of flexion revealed grade II laxity (5-10 mm opening) with a soft endpoint, consistent with a partial or complete superficial MCL tear. At 0° extension, valgus stress showed mild opening but a firm endpoint, suggesting the deep MCL was intact or minimally involved, or there was a concomitant posteromedial capsule injury.
*
Lateral Collateral Ligament (LCL) / Posterolateral Corner (PLC):
Varus stress testing
at 30° of flexion initially suggested mild-moderate laxity (grade I-II), but the endpoint was difficult to discern clearly due to pain. A
Dial Test
at 30° of flexion showed an asymmetry of external rotation greater than 10-15° compared to the contralateral side. The
External Rotation Recurvatum test
was difficult to interpret due to the flexion contracture but appeared subtly positive. The presence of a subtle recurvatum on inspection raised suspicion for a PLC injury. Tenderness over the fibular head was also noted. The combined presence of a seemingly less dramatic Lachman/Anterior Drawer despite a definite ACL injury mechanism, coupled with the subtle sag sign and positive dial test, strongly indicated a complex, multi-ligamentous injury extending beyond an isolated ACL tear.
*
Neurological/Vascular Assessment:
Distal pulses (dorsalis pedis and posterior tibial) were present and strong bilaterally. Capillary refill was brisk. Sensory examination was intact in the distribution of the superficial and deep peroneal nerves. Motor function of foot dorsiflexion and plantarflexion was intact.
This clinical picture, particularly the combination of anterior and posterolateral laxity findings, raised significant concern for a combined ACL and Posterolateral Corner (PLC) injury, potentially compounded by a PCL injury, which can sometimes mask the true extent of anterior laxity. The initial seemingly "mild" Lachman could be attributed to the posterior translation of the tibia in a PCL-deficient knee, effectively reducing the apparent anterior translation on the Lachman test from its true starting position. Alternatively, a significant PLC injury can influence the kinematic behavior, leading to a complex multiplanar instability that confounds isolated ligament testing.
Imaging & Diagnostics
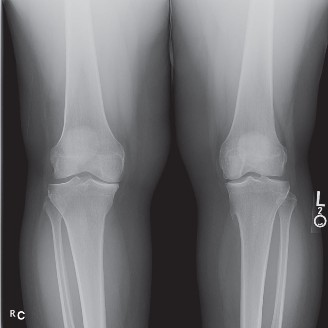
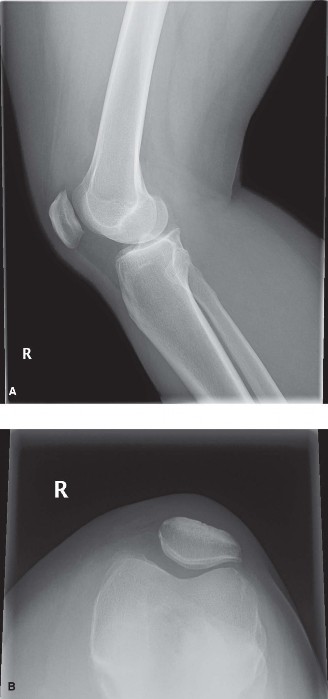
Initial Radiographs
- Anteroposterior (AP) View: Demonstrated no acute fracture or dislocation. Joint space appeared preserved.
- Lateral View: No significant tibial plateau depression or condylar fracture. However, a subtle avulsion fracture from the fibular head was identified, consistent with the "Arcuate Sign," which is highly indicative of a PLC injury. A subtle posterior subluxation of the tibia relative to the femur was also noted, consistent with the posterior sag observed clinically.
- Oblique Views: Confirmed findings from AP and lateral views. No other obvious osseous injury.
- Rosenberg View (Weight-bearing PA flexed 45°): Not obtained initially due to patient's inability to bear weight.
- Sunrise View: Not obtained.
The presence of the arcuate sign on initial X-rays immediately escalated the suspicion of a severe multi-ligamentous knee injury, specifically involving the PLC, despite the initial clinical focus on the ACL tear.
Magnetic Resonance Imaging (MRI)
MRI of the right knee was performed within 24 hours of injury to thoroughly evaluate the soft tissue structures.
- ACL: Complete, mid-substance tear of the anterior cruciate ligament with extensive edema and hemorrhage throughout its fibers. The femoral attachment was retracted.
- PCL: High-grade partial tear of the posterior cruciate ligament at its tibial attachment, with significant interstitial edema and disruption of a large portion of its fibers. This explained the subtle sag sign and posterior drawer laxity.
- MCL: Grade II complete tear of the superficial MCL at its femoral attachment, with surrounding edema. The deep MCL and posteromedial capsule were also noted to have interstitial edema and minor tearing but largely intact continuity.
-
LCL / PLC:
This was the critical finding:
- Complete avulsion of the fibular collateral ligament (FCL) from its femoral attachment.
- Disruption of the popliteus tendon (PLT) at its musculotendinous junction.
- Avulsion of the arcuate ligament complex and the biceps femoris tendon insertion from the fibular head, corresponding to the "Arcuate Sign" seen on X-ray.
- Significant edema and disruption within the posterolateral capsule.
-
(Figure 1: Coronal MRI sequence demonstrating a complete avulsion of the fibular collateral ligament (FCL) from its femoral attachment (arrow), along with surrounding soft tissue edema consistent with a high-grade posterolateral corner injury. Note the associated bone bruise on the lateral femoral condyle.)
- Menisci: A radial tear of the posterior horn of the lateral meniscus was identified, extending to the peripheral rim. The medial meniscus appeared intact.
- Articular Cartilage: Grade I chondral softening was noted on the lateral femoral condyle and lateral tibial plateau, consistent with bone bruising from the impact, but no significant full-thickness defects were identified.
- Bone Edema: Extensive bone bruise patterns were observed in the lateral femoral condyle, lateral tibial plateau, and posterior aspect of the medial tibial plateau, classic for a valgus-external rotation/hyperextension injury.
The comprehensive MRI confirmed a multi-ligamentous knee injury involving the ACL, PCL, MCL (Grade II), and a severe Grade III Posterolateral Corner injury (FCL, popliteus tendon, arcuate complex). This constellation of injuries explains the discrepancies in the initial clinical assessment, where the PCL insufficiency and significant PLC laxity likely altered the mechanical properties of the knee, making isolated ACL testing potentially misleading. The initial "firm but soft" endpoint on Lachman, combined with the subtle posterior sag, indicates a complex instability rather than a simple ACL tear.
Templating and Pre-operative Planning
Based on MRI findings, detailed pre-operative templating was initiated for multi-ligament reconstruction.
*
Graft Selection:
Autografts were prioritized for primary reconstruction due to the patient's age and activity level. Options considered included quadriceps tendon autograft for ACL, ipsilateral semitendinosus/gracilis autograft for PCL, and contralateral semitendinosus/gracilis autograft or Achilles tendon allograft for PLC reconstruction. Given the need for robust grafts for multiple ligaments, the decision was made for a quadriceps tendon autograft for the ACL, and a split hamstring autograft for the PCL (semitendinosus) and a combination of fibular head advancement and Achilles tendon allograft for the PLC.
*
Tunnel Placement:
Careful consideration of anatomical tunnel placement to avoid convergence and ensure isometric graft tensioning for all reconstructed ligaments.
*
Surgical Sequencing:
A staged approach might be considered in some complex multi-ligament injuries, but for this constellation, a single-stage reconstruction was deemed appropriate given the acute nature and patient's athletic demands.
Differential Diagnosis
The acute, high-energy knee injury in a young athlete necessitates a broad differential diagnosis for knee instability. The key is to differentiate between isolated ligamentous injuries and complex multi-ligamentous injuries, as management strategies vary significantly.
| Feature | Isolated ACL Tear with Meniscal Tear | ACL Tear with Concomitant Grade II MCL Tear | ACL Tear with Grade III Posterolateral Corner (PLC) Injury & PCL Partial Tear (Our Case) |
|---|---|---|---|
| Mechanism of Injury | Non-contact deceleration, pivot, hyperextension, valgus (less severe) | Valgus stress, external rotation, often non-contact | High-energy hyperextension, varus, internal/external rotation, direct trauma to anteromedial tibia |
| Clinical Presentation | "Pop," rapid swelling, anterior instability ("giving way"), pain | Similar to ACL, medial pain, valgus instability | "Pop," rapid swelling, multiplanar instability (anterior, posterior, rotational), pain laterally, varus thrust |
| Lachman Test | Positive (grade 2-3), soft or absent endpoint, increased translation | Positive (grade 2-3), soft or absent endpoint | Positive (grade 2-3) but may appear less dramatic due to PCL insufficiency or complex multiplanar laxity; soft/absent endpoint |
| Anterior Drawer | Positive (grade 2-3) | Positive (grade 2-3) | Positive (grade 2-3), potentially confounded by PCL insufficiency |
| Posterior Sag Test | Negative | Negative | Positive (subtle to overt) due to PCL insufficiency or combined PLC/PCL injury |
| Posterior Drawer | Negative | Negative | Positive (grade 1-2) with a firm or soft endpoint |
| Valgus Stress Test | Negative or minor laxity at 30° flexion | Positive at 30° flexion (grade 2, soft endpoint), potentially at 0° (grade 1) | Negative (unless associated MCL tear), but may show medial side opening if valgus vector is applied to an already unstable knee |
| Varus Stress Test | Negative | Negative | Positive at 30° and 0° flexion (grade 3, no endpoint), significant laxity |
| Dial Test | Negative | Negative | Positive (>10-15° difference in external rotation at 30° and 90° flexion compared to contralateral) |
| External Rotation Recurvatum | Negative | Negative | Positive (subtle to overt) |
| Imaging (X-ray) | May show Segond fracture (ACL avulsion) or bone bruise | May show bone bruise, rarely avulsion | Arcuate sign (fibular head avulsion), lateral capsular avulsion, posterior tibial subluxation |
| Imaging (MRI) | ACL tear, meniscal tear(s), bone bruise | ACL tear, MCL tear (femoral/tibial), meniscal tear, bone bruise | ACL tear, PCL tear (partial/complete), FCL tear, popliteus tear, arcuate complex disruption, LCL tear, significant bone bruise, meniscal tears (often lateral) |
| Treatment Strategy | ACL reconstruction, meniscal repair/debridement | ACL reconstruction, MCL management (non-op or repair), meniscal repair/debridement | Multi-ligament reconstruction (ACL, PCL, PLC), meniscal repair, comprehensive rehabilitation |
Surgical Decision Making & Classification
The decision for surgical intervention was unequivocally indicated for this patient due to:
1.
High-grade multi-ligamentous injury:
Complete ACL tear, high-grade partial PCL tear, Grade II MCL tear, and a severe Grade III PLC injury.
2.
Patient demographics and activity level:
A young, active competitive athlete with high demands on knee stability.
3.
Mechanical instability:
Documented gross multiplanar instability on clinical examination and confirmed by MRI, rendering the knee functionally unstable for daily activities, let alone sports.
4.
Concomitant meniscal tear:
A reparable radial lateral meniscal tear.
Non-operative management for this constellation of injuries would invariably lead to chronic instability, premature osteoarthritis, and inability to return to sports. While isolated Grade I-II MCL tears can often be managed non-operatively, the severe PLC injury, combined with ACL and PCL pathology, necessitated comprehensive surgical reconstruction.
Classification Systems Applied:
- ACL Tear: Mid-substance tear.
- PCL Tear: High-grade partial tear, Type II according to Fanelli classification (posterior translation 6-10 mm).
- MCL Tear: Grade II tear (5-10 mm opening at 30° valgus stress).
- Posterolateral Corner (PLC) Injury: Classified as a Grade III injury based on significant laxity (varus stress, dial test, external rotation recurvatum) and MRI findings showing complete disruption of the FCL, popliteus tendon, and arcuate complex. According to the LaPrade classification , this would involve disruption of at least three primary posterolateral structures (FCL, popliteus tendon, popliteofibular ligament). This requires surgical repair or reconstruction for restoration of stability.
- Meniscal Tear: Radial tear of the posterior horn of the lateral meniscus, which was deemed amenable to repair.
The comprehensive nature of the injury mandated a staged, systematic surgical approach to address each component and restore overall knee stability.
Surgical Technique / Intervention
The patient underwent a single-stage multi-ligament reconstruction approximately 10 days post-injury to allow for some subsidence of acute inflammation and effusion, while still being within the optimal window for acute PLC repair/reconstruction.
Patient Positioning:
The patient was placed supine on the operating table with a leg holder. A tourniquet was applied high on the thigh. The knee was prepped and draped in the usual sterile fashion, allowing full range of motion. Examination under anesthesia (EUA) was performed prior to incision. This confirmed the grade III PLC injury, grade II MCL, and complete ACL and partial PCL tears.
Arthroscopic Assessment and Meniscal Repair:
Diagnostic arthroscopy was performed through standard anteromedial and anterolateral portals.
1.
Arthroscopic Survey:
A systematic review of all knee compartments confirmed the ACL rupture, the high-grade PCL tear, and the lateral meniscal radial tear. Chondral surfaces were inspected and found to be intact apart from minor bruising.
2.
Lateral Meniscus Repair:
The radial tear in the posterior horn of the lateral meniscus was addressed first. An all-inside technique was utilized, with two suture anchors placed across the tear, achieving stable reduction and compression of the meniscal fragments.
3.
Debridement:
The torn remnants of the ACL and PCL were debrided to facilitate anatomical reconstruction.
ACL Reconstruction:
- Graft Harvest: A quadriceps tendon autograft was harvested from the ipsilateral knee through a 3-4 cm incision proximal to the patella. A 10mm wide, 70-80mm long bone block was taken with the central quadriceps tendon, ensuring adequate length and robust tissue. The harvest site was closed in layers.
- Femoral Tunnel: An anteromedial portal technique was used to create an anatomical femoral tunnel for the ACL. A guide pin was placed at the footprint of the native ACL, typically at the 10:30 position in the right knee. Reaming was performed to the appropriate depth matching the graft diameter and bone block length.
- Tibial Tunnel: A tibial guide was used to place the tibial tunnel anterior to the PCL, aiming for the native ACL footprint. Over-reaming was avoided to prevent tunnel convergence with the PCL graft.
- Graft Passage and Fixation: The quadriceps tendon graft was passed antegrade through the tibial tunnel into the femoral tunnel. Femoral fixation was achieved with an interference screw placed through the femoral bone block. Tibial fixation was achieved with an interference screw after appropriate tensioning, with the knee in approximately 20-30° of flexion.
PCL Reconstruction:
- Graft Harvest: A semitendinosus autograft was harvested from the contralateral knee to avoid excessive ipsilateral donor site morbidity. This was prepared in a four-strand configuration.
- Femoral Tunnel: A transtibial approach was used to drill the femoral tunnel for the PCL. The guide pin was placed on the medial femoral condyle, superior to the origin of the native PCL. Reaming was performed to a depth matching the graft.
- Tibial Tunnel: A posterior approach (posterior capsule visualization portal via posteromedial portal) was used to identify the PCL footprint on the tibia. A guide pin was drilled from anterior tibia, exiting at the PCL footprint. Care was taken to avoid neurovascular structures in the posterior compartment.
- Graft Passage and Fixation: The semitendinosus graft was passed through the tibial tunnel, then through the femoral tunnel. Both ends were secured with interference screws, with the knee flexed to 90° and a posterior drawer applied to reduce the tibia, ensuring proper tensioning.
Posterolateral Corner (PLC) Reconstruction:
Given the Grade III PLC injury, a reconstruction using the LaPrade anatomical technique was chosen.
1.
Incision and Exposure:
A curvilinear incision was made over the lateral aspect of the knee, extending from the lateral epicondyle to the fibular head. Full thickness flaps were raised to expose the distal IT band, biceps femoris tendon, fibular head, and lateral femoral epicondyle.
2.
FCL Repair/Reconstruction:
The avulsed FCL was identified. Given its complete avulsion and quality, an Achilles tendon allograft was chosen for reconstruction.
*
Fibular Tunnel:
A 7mm tunnel was drilled through the fibular head from anterior to posterior, perpendicular to the long axis of the fibula.
*
Femoral Tunnel:
A guide wire was placed at the isometric femoral attachment of the FCL (proximal and posterior to the lateral epicondyle), and a 7mm tunnel was drilled.
*
Graft Passage:
The Achilles allograft was passed through the fibular head tunnel from posterior to anterior, then through the femoral tunnel.
3.
Popliteus Tendon Reconstruction:
A small tunnel was drilled at the popliteus sulcus on the lateral femoral condyle. The free end of the Achilles allograft was routed to recreate the popliteus tendon.
4.
Fixation:
The grafts were fixed in a tensioned manner. The FCL graft was tensioned with the knee in 20° flexion and neutral rotation, and fixed with an interference screw. The popliteus component was then tensioned with the knee in 70° flexion and fixed with a staple or interference screw. The fibular head was also advanced slightly medially and anteriorly to further tension the PLC structures and minimize posterior subluxation.
*
(Figure 2: Intraoperative image illustrating the reconstructed Posterolateral Corner (PLC) with an allograft. The Achilles tendon allograft (white arrows) is secured to the fibular head and routed to the lateral femoral epicondyle, recreating the FCL and Popliteofibular Ligament attachments. Note the meticulous attention to anatomical tunnel placement.)
MCL Management:
The Grade II MCL tear was managed non-operatively, relying on the stability provided by the ACL, PCL, and PLC reconstructions, and post-operative bracing. Primary repair was not deemed necessary given its inherent healing capacity and grade.
Closure:
All incisions were closed in layers. A sterile dressing was applied, and a hinged knee brace was placed, locked in extension.
Post-Operative Protocol & Rehabilitation
The post-operative rehabilitation protocol for multi-ligament knee reconstruction is significantly more conservative and prolonged than for isolated ACL reconstruction, prioritizing protection of all reconstructed ligaments, especially the PLC.
Phase I: Maximum Protection (Weeks 0-6)
- Weight Bearing: Non-weight bearing (NWB) for 4-6 weeks with crutches. Partial weight-bearing may be initiated for ambulation if tolerated and no instability.
- Bracing: Hinged knee brace locked in full extension for ambulation and sleep for the first 4-6 weeks to protect the PLC. The brace may be unlocked for controlled ROM exercises in the prone position.
-
Range of Motion (ROM):
- Weeks 0-2: Passive ROM 0-30° of flexion. Avoid active hamstring contraction.
- Weeks 2-4: Passive ROM 0-60° of flexion.
- Weeks 4-6: Passive ROM 0-90° of flexion.
-
Exercises:
- Early Quadriceps Activation: Quad sets, straight leg raises (SLR) with brace locked.
- Ankle pumps to prevent DVT.
- Patellar mobilizations.
- Gentle, passive knee flexion to avoid stress on PLC and PCL grafts. Avoid active resisted knee flexion (hamstrings) to protect PCL graft. Avoid open-chain terminal knee extension (0-30°) to protect ACL graft.
- Precautions: Avoid varus stress, external rotation beyond neutral, and active hamstring contraction. No active PCL engagement (e.g., hamstring curls).
Phase II: Moderate Protection (Weeks 6-12)
- Weight Bearing: Progressive weight-bearing, transitioning to full weight-bearing by week 8-10, as tolerated. Crutches discontinued once gait is normalized without a limp.
- Bracing: Brace worn for ambulation, unlocked for ROM and exercises. Brace may be discontinued for specific activities once adequate muscle control and stability are achieved, typically around week 10-12.
- Range of Motion (ROM): Progress towards full knee flexion (120-130°).
-
Exercises:
- Initiate closed-chain exercises: Mini-squats, leg presses (limited depth), calf raises, wall slides.
- Submaximal isometric hamstring exercises.
- Gentle proprioceptive drills: Weight shifts, balance board (bilateral then unilateral).
- Stationary cycling with low resistance (brace on initially).
- Avoid valgus stress and aggressive external rotation exercises.
Phase III: Strengthening and Neuromuscular Control (Months 3-6)
- Weight Bearing: Full weight-bearing.
- Bracing: Typically discontinued for daily activities, but may be used for sport-specific training or higher-risk activities.
- Range of Motion (ROM): Full, pain-free ROM expected.
-
Exercises:
- Progressive closed-chain strengthening: Lunges, step-ups, increased resistance on leg press/squats.
- Open-chain strengthening for quadriceps (avoiding 0-30° extension).
- Core stability exercises.
- Advanced proprioceptive training: Single-leg balance, dynamic balance.
- Initiate light plyometrics (e.g., double leg hops) and agility drills (straight line only).
- Gradual introduction of sport-specific movements but no cutting or pivoting.
Phase IV: Return to Activity/Sport (Months 6-12+)
- Functional Progression: Gradual progression of sport-specific drills, including cutting, pivoting, jumping, and landing mechanics.
- Strength & Endurance: Achieve full strength and endurance comparable to the contralateral limb.
-
Return to Sport Criteria:
- No pain or swelling.
- Full, symmetrical range of motion.
- Isokinetic strength testing >90% of contralateral limb for hamstrings and quadriceps.
- Passing a battery of functional tests (e.g., single-leg hop test, crossover hop, triple hop) at >90% of contralateral limb.
- Satisfactory stability on clinical examination.
- Athlete-specific training with gradual return to practice, then competition.
- Timeline: Return to contact sports typically not before 9-12 months post-surgery, often longer for complex multi-ligament reconstructions (12-18 months). A custom functional brace may be recommended for return to sport.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- High Index of Suspicion: Always suspect a multi-ligamentous knee injury in cases of high-energy trauma, knee dislocation (even if spontaneously reduced), or if initial ACL test results seem incongruous with the mechanism or overall instability.
-
Systematic Clinical Examination:
- Perform a thorough examination after adequate analgesia and muscle relaxation (e.g., in the ED or under anesthesia). Guarding can mask subtle laxity.
- Always compare to the contralateral knee.
- Don't stop at the Lachman test. Test all four primary ligaments and, critically, the Posterolateral Corner (PLC) with varus stress at 0° and 30°, and the Dial Test at 30° and 90°.
- Specifically look for a posterior sag sign, external rotation recurvatum, and a subtle recurvatum.
-
Imaging Interpretation:
- X-rays: Meticulously review for avulsion fractures such as a Segond fracture (ACL), Arcuate sign (PLC), or fibular head avulsion (PLC). Assess for subtle posterior tibial subluxation.
- MRI: Crucial for soft tissue assessment. Look for patterns of bone bruising (e.g., lateral femoral condyle/tibial plateau for ACL/PLC; posterior medial tibial plateau for PCL). Do not focus solely on the ACL; systematically evaluate all ligaments, menisci, and articular cartilage, paying close attention to the PLC structures (FCL, popliteus tendon, PFL, biceps femoris insertion). Specific sequences might be needed for full PLC evaluation.
- Comprehensive Surgical Planning: Address all significant injuries identified. Leaving a significant PLC injury untreated after ACL reconstruction is a recipe for failure, leading to increased graft strain and persistent instability.
- Anatomical Reconstruction: Aim for anatomical placement of all grafts to restore normal knee kinematics.
- Graft Choice: Consider autografts for young, active patients. For multi-ligament injuries, this often necessitates multiple autograft harvest sites or the use of allografts, with careful consideration of their respective advantages and disadvantages.
- Rehabilitation: A prolonged, protected, and carefully staged rehabilitation protocol is paramount, especially for PLC and PCL reconstructions, to allow for graft incorporation and maturation while preventing undue stress.
Pitfalls:
- Missing Concomitant Injuries: The most common pitfall is focusing solely on the "obvious" ACL tear and missing crucial concomitant injuries, particularly of the PLC or PCL. This leads to persistent instability and potential failure of the ACL reconstruction.
- Inadequate Examination: An incomplete or rushed clinical exam, especially in a painful acute knee, can lead to misdiagnosis or underestimation of the injury's severity.
- Over-reliance on a Single Test: The Lachman test, while excellent for ACL, does not tell the whole story, especially in multi-ligamentous injury patterns where other laxities (e.g., PCL sag) can mask the true anterior translation.
- Failure to Recognize "Combined" Laxity Patterns: Understanding how different ligamentous injuries interact is key. A PCL-deficient knee will already have posterior subluxation, which can make the Lachman appear deceptively less positive, as the tibia starts from a more posterior position. Similarly, a PLC injury significantly alters rotational stability, impacting how the knee responds to anterior-posterior tests.
- Premature Aggressive Rehabilitation: Pushing rehabilitation too quickly, especially with unprotected range of motion or weight-bearing, can jeopardize graft integrity, particularly for PLC and PCL reconstructions which require longer protection.
- Tunnel Convergence: In multi-ligament reconstruction, careful planning is required to avoid tunnel convergence, which can compromise graft integrity and fixation.
- Neglecting Rotational Instability: The PLC is critical for posterolateral and external rotational stability. Failure to address this leads to persistent "pivot shift" type instability even after ACL reconstruction.
By maintaining a high index of suspicion, performing a meticulous clinical examination, and critically interpreting imaging studies, orthopedic surgeons can avoid missing the complex pathology that often accompanies apparent isolated ACL injuries, thereby ensuring optimal patient outcomes.
