Patient Presentation & History
A 22-year-old collegiate male soccer player presented to the emergency department with acute right knee pain, swelling, and instability following a non-contact injury during a competitive match. The mechanism described was a sudden deceleration with a pivoting motion on a planted foot, followed by a valgus collapse of the knee. He reported hearing a distinct "pop" at the time of injury, experienced immediate severe pain, and was unable to bear weight or continue playing.
His past medical history was unremarkable, with no significant comorbidities. He was highly active, participating in competitive soccer at a Division I collegiate level, and had no prior history of knee injury or surgical intervention. He reported no allergies and was not taking any regular medications. Social history was negative for smoking and he consumed alcohol occasionally. His primary goal was to return to elite-level competitive soccer.
Clinical Examination
Upon initial examination in the emergency department, the patient was in moderate distress dueating to pain.
*
Inspection:
The right knee demonstrated significant effusion, particularly in the suprapatellar pouch. Mild ecchymosis was noted laterally. The knee was held in approximately 15 degrees of flexion, with visible guarding against extension. No gross deformity was observed.
*
Palpation:
Diffuse tenderness was elicited over the medial and lateral joint lines, as well as along the anteromedial aspect of the knee. A significant effusion was ballotable, and the knee felt warm to the touch. No focal tenderness over bony prominences suggested an acute fracture, though this could not be definitively ruled out without imaging.
*
Range of Motion (ROM):
Active range of motion was severely limited due to pain and swelling, ranging from 15 degrees of flexion to approximately 90 degrees. Passive range of motion was similarly restricted, with a painful endpoint on attempts at full extension.
*
Ligamentous Stability Testing:
*
Lachman Test:
Performed at 20-30 degrees of flexion, this test was grossly positive (Grade III), demonstrating significant anterior tibial translation with a soft, indistinct end-point, indicative of a complete anterior cruciate ligament (ACL) rupture.
*
Anterior Drawer Test:
Positive, confirming anterior instability, though often less sensitive than the Lachman test in the acute setting due to hamstring guarding.
*
Pivot Shift Test:
Initially difficult to assess due to pain and muscle guarding, but with gentle manipulation, a definitive clunk was elicited during the reduction phase as the knee was brought from flexion to extension with valgus and internal rotation. This strongly suggested anterolateral rotatory instability.
*
Posterior Drawer Test and Posterior Sag Sign:
Negative, ruling out significant posterior cruciate ligament (PCL) injury.
*
Varus Stress Test:
Stable in full extension and at 30 degrees of flexion, indicating an intact lateral collateral ligament (LCL) complex.
*
Valgus Stress Test:
Stable in full extension, with mild gapping at 30 degrees of flexion, suggesting a Grade I or II medial collateral ligament (MCL) sprain, often concomitant with ACL injuries.
*
Meniscal Testing:
*
McMurray Test:
Positive with a palpable and audible click during internal and external rotation, particularly with valgus stress and extension, suggesting a medial meniscal tear.
*
Apley Grind Test:
Produced pain and a click, further supporting a meniscal lesion.
*
Patellofemoral Joint:
No evidence of patellar apprehension or instability. Patellar grind test was negative.
*
Neurological Assessment:
Distal sensation was intact in all major nerve distributions (femoral, sciatic, peroneal, tibial). Motor function of the ankle dorsiflexors, plantarflexors, and great toe extensors was normal.
*
Vascular Assessment:
Distal pulses (dorsalis pedis and posterior tibial) were strong and symmetrical bilaterally. Capillary refill was brisk in the toes. No signs of vascular compromise were present.
Imaging & Diagnostics
Immediate imaging was crucial to confirm the clinical diagnosis and assess for associated injuries.
-
Plain Radiographs:
Anteroposterior (AP), lateral, and oblique views of the right knee were obtained. These images ruled out acute fractures and dislocations. A moderate joint effusion was noted. Importantly, a small avulsion fracture of the lateral tibial plateau, consistent with a Segond fracture, was identified on the AP view. This finding is highly pathognomonic for an ACL rupture, occurring in approximately 10-15% of cases. No significant osteochondral defects were visible on plain films.
-
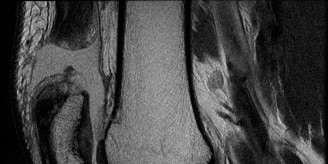
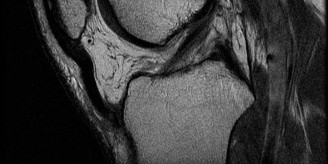
Magnetic Resonance Imaging (MRI): An MRI of the right knee was performed within 48 hours to fully characterize the soft tissue injuries. The findings were as follows:
- ACL: Complete mid-substance rupture of the anterior cruciate ligament, with evidence of fiber discontinuity and hemorrhage within the intercondylar notch. The torn ends were retracted.
- Menisci: A complex, displaced bucket-handle tear of the posterior horn and body of the medial meniscus was identified, with the torn fragment flipped into the intercondylar notch, causing mechanical symptoms. A small, stable radial tear of the lateral meniscus was also noted.
- Collateral Ligaments: A Grade II sprain of the superficial medial collateral ligament (MCL) was confirmed, characterized by signal change and edema within the ligament substance, but without complete fiber disruption. The LCL complex appeared intact.
- Bone Contusions: Significant bone bruising (trabecular microfractures) was evident on the posterior aspect of the lateral tibial plateau and the lateral femoral condyle, consistent with the "kissing lesions" often seen with acute pivot shift injuries. No frank osteochondral defect was identified on the articular surfaces, but the presence of bone contusion warranted careful arthroscopic inspection.
-
Other:
A large knee joint effusion was present. Other knee structures, including the PCL, patellar tendon, quadriceps tendon, and articular cartilage elsewhere, appeared grossly normal.
-
Templating: Pre-operative planning based on MRI and patient anatomy was performed to anticipate graft length and diameter requirements, tunnel placement (e.g., femoral tunnel using an anteromedial portal for anatomic placement), and choice of fixation devices. Femoral and tibial tunnel trajectories were considered to minimize impingement and maximize isometricity.
Differential Diagnosis
The clinical presentation and initial imaging strongly pointed towards an acute ACL rupture with associated meniscal and collateral ligament injuries. However, a comprehensive differential diagnosis is crucial, particularly in a trauma setting, to avoid missing other potentially debilitating conditions.
| Feature | Acute ACL Rupture w/ Meniscal Tear (Primary Dx) | Multi-Ligamentous Knee Injury (e.g., ACL + PCL + MCL/LCL) | Acute Patellar Dislocation w/ Osteochondral Fracture |
|---|---|---|---|
| Mechanism of Injury | Non-contact pivot, deceleration, valgus collapse, hyperextension (often low-to-moderate energy) | High-energy trauma (e.g., motor vehicle accident, severe athletic collision), gross valgus/varus, hyperextension | Twisting injury on a flexed knee, direct blow to patella, forceful quadriceps contraction during valgus/ER moment |
| Presentation | Immediate pain, "pop", acute swelling, feeling of instability, difficulty weight-bearing, limited ROM | Gross instability, severe pain, immediate and often massive swelling, potential neurovascular deficit, significant guarding | Immediate pain, visible deformity (if still dislocated), apprehension to lateral patellar movement, often feeling of "giving way" or "pop" |
| Clinical Exam | Grossly positive Lachman/Pivot Shift, positive McMurray, joint line tenderness, effusion, limited ROM | Multiple positive ligamentous tests (e.g., positive Lachman, posterior sag, varus/valgus gapping), gross instability in multiple planes, possible neurovascular deficit | Patellar apprehension, J-sign (lateral patellar tracking), tenderness over medial patellofemoral ligament (MPFL) insertion, palpable defect if dislocated, effusion |
| Radiographs | Effusion, possible Segond fracture, possible small avulsion fracture (e.g., tibial spine) | Effusion, possible avulsion fractures (e.g., tibial spine, arcuate complex), osteochondral injuries, possible knee dislocation | Lateral patellar subluxation/dislocation (if not reduced), possible osteochondral fragment from patella or lateral femoral condyle |
| MRI Findings | Complete ACL rupture, meniscal tear (e.g., bucket-handle), bone bruise (lateral femoral condyle/tibial plateau), possible collateral ligament sprain (Grade I/II) | ACL, PCL, MCL, LCL ruptures (complete), capsule disruption, extensive bone bruising, potential neurovascular injury (popliteal artery, peroneal nerve) | Medial patellofemoral ligament (MPFL) tear, patellar subluxation/dislocation, osteochondral lesion (patella or lateral femoral condyle), possible vastus medialis obliquus (VMO) detachment |
| Treatment Indication | Symptomatic instability, athletic demands, associated reparable meniscal tears, young active patient | Almost always operative for multi-ligament reconstruction and stabilization due to severe instability and risk of early arthrosis | Often non-operative for first-time dislocation unless large osteochondral injury or significant recurrent instability |
Surgical Decision Making & Classification
The decision for operative intervention in this patient was straightforward and multifactorial:
- Patient Demographics and Goals: A young, highly active collegiate athlete with a strong desire to return to competitive pivoting sports. Non-operative management would almost certainly result in recurrent instability, secondary meniscal tears, and progressive chondral damage, making a return to his prior level of activity impossible.
- Clinical Instability: The physical examination, with a grossly positive Lachman and Pivot Shift test, clearly demonstrated significant anterolateral rotatory instability, compromising the knee's functional integrity.
- Associated Meniscal Pathology: The MRI revealed a displaced bucket-handle tear of the medial meniscus. Such tears are often reparable, and delaying surgery or opting for non-operative management of the ACL would prevent immediate meniscal repair, potentially leading to excision if the tear becomes chronic or irreparable, with long-term consequences for knee health.
- Concomitant Injuries: The Grade II MCL sprain, while often managed non-operatively in isolation, can benefit from early stability provided by ACL reconstruction to protect its healing. The bone bruising indicated a significant acute trauma to the articular cartilage, emphasizing the need for stability to prevent further injury.
Classification:
*
ACL Rupture:
Classified as a complete, mid-substance rupture (as opposed to an avulsion, though a Segond fracture was present).
*
Meniscal Tears:
Medial meniscus: Complex, displaced bucket-handle tear of the posterior horn and body. Lateral meniscus: Stable radial tear.
*
Collateral Ligament Injury:
Grade II sprain of the superficial MCL.
*
Bone Contusions:
Extensive lateral femoral condyle and posterolateral tibial plateau bone bruising.
Graft Choice:
For a young, high-demand athlete, autograft is generally preferred over allograft due to superior mechanical properties, lower re-rupture rates, and biological integration. The choice between bone-patellar tendon-bone (BPTB), hamstring (semitendinosus and gracilis, HS), or quadriceps tendon (QT) autograft was discussed with the patient.
*
BPTB:
Excellent stiffness, bone-to-bone healing, historical "gold standard." Disadvantages include patellofemoral pain, kneeling pain, and potential for patellar fracture.
*
Hamstring (HS):
Less anterior knee pain, cosmetically preferred. Disadvantages include potential for hamstring weakness (though often transient) and delayed healing in the femoral tunnel with suspensory fixation.
*
Quadriceps Tendon (QT):
Growing popularity, good biomechanical properties, less anterior knee pain than BPTB, potential for larger graft volume. Requires specific harvest technique.
Given the patient's desire to minimize anterior knee pain and the robust nature of quadruple-stranded hamstring grafts, we opted for a quadruple-stranded hamstring autograft (semitendinosus and gracilis) . This choice offers comparable strength to BPTB with potentially fewer donor site morbidity issues for an athlete whose sport involves extensive running and jumping.
Surgical Technique / Intervention
The surgical procedure was performed in a meticulous, stepwise fashion.
-
Patient Positioning and Anesthesia:
- The patient was placed supine on the operating table.
- A high-thigh tourniquet was applied to the right leg.
- A lateral post was positioned just proximal to the knee to allow valgus stress and facilitate exposure.
- The operative leg was prepped and draped in a sterile fashion, ensuring full range of motion of the knee was possible.
- General anesthesia was administered, with a femoral nerve block providing adjunctive post-operative analgesia.
-
Diagnostic Arthroscopy and Assessment of Concomitant Injuries:
- Standard anteromedial (AM) and anterolateral (AL) portals were established.
- Initial diagnostic arthroscopy confirmed the complete ACL rupture with fraying of the stump.
- The articular cartilage surfaces were meticulously inspected. No significant chondral flaps or defects requiring intervention beyond débridement were noted, aligning with the MRI findings of bone contusions without full-thickness defects.
- The medial compartment was assessed. The displaced bucket-handle tear of the medial meniscus was identified. The torn fragment was reduced back into its anatomical position and found to be stable, with a vascularized peripheral rim suitable for repair.
- The lateral compartment was assessed. The radial tear of the lateral meniscus was found to be stable and peripheral; given its small size and stable nature, it was débrided minimally to prevent future propagation.
-
Meniscal Repair:
- The medial meniscal bucket-handle tear was repaired using an all-inside technique (e.g., Fast-Fix, Meniscal Cinch devices). This involved placing multiple absorbable sutures across the tear, securing the torn fragment to the stable meniscal rim, ensuring robust compression and stability. The repair was confirmed to be stable under probing.
-
Graft Harvest:
- A 3-4 cm oblique incision was made over the pes anserinus tendon insertion, approximately 3 cm distal and 2 cm medial to the tibial tubercle.
- The sartorius fascia was incised, and the semitendinosus and gracilis tendons were identified.
- Using an open-ended tendon stripper, the semitendinosus and gracilis tendons were harvested high from their musculotendinous junctions.
- The tendons were cleaned of muscle fibers and measured. They were then quadruple-stranded using a whipstitch technique with a high-strength braided suture (e.g., FiberWire) to create a robust graft of approximately 8-9 mm in diameter and appropriate length (typically 75-80 mm). Both ends of the graft were pre-tensioned on a graft board for 10 minutes at 80 Newtons to remove creep.
-
Tunnel Preparation:
- Femoral Tunnel: An anteromedial portal approach was utilized to create an anatomic femoral tunnel. A guide wire was placed through the AM portal, aiming for the center of the native ACL femoral footprint, ensuring appropriate orientation for both the anteromedial and posterolateral bundles of the ACL. A cannulated reamer (e.g., 8.5 mm or 9 mm, matching graft diameter) was used to create the femoral tunnel to a depth of 25-30 mm, ensuring a cortical bridge of at least 10 mm.
- Tibial Tunnel: A tibial guide was used to position the guide wire in the center of the native ACL tibial footprint, anterior to the PCL, avoiding impingement in full extension. Careful consideration was given to the guide's angle to create a tunnel that would not impinge on the intercondylar notch in extension and would allow for sufficient graft length. The tibial tunnel was then reamed to the appropriate diameter matching the graft.
-
Graft Passage and Fixation:
- A retrograde suture was passed from the femoral tunnel out the anterolateral thigh, followed by the graft sutures. The quadruple-stranded hamstring graft was then pulled through the tibial tunnel and into the femoral tunnel.
- Femoral Fixation: A cortical suspension device (e.g., EndoButton CL) was used for femoral fixation. The EndoButton was deployed over the lateral femoral cortex, securing the graft within the femoral tunnel.
- Tibial Fixation: With the knee in approximately 20-30 degrees of flexion, and with an anterior drawer applied to restore stability, the graft was tensioned. A bioabsorbable interference screw (e.g., 9x23 mm BioComposite screw) was inserted alongside the graft in the tibial tunnel, compressing the graft against the tunnel wall. The remaining graft limbs were tied over a post on the anteromedial tibia to provide additional back-up fixation and aid initial stability.
-
Final Assessment and Closure:
- Full range of motion was demonstrated, confirming no impingement of the graft in the intercondylar notch.
- Lachman and Pivot Shift tests were performed, showing a stable knee with a firm end-point, significantly improved from the pre-operative state.
- All portals were closed with interrupted nylon sutures. The hamstring harvest site was closed in layers. Sterile dressings were applied, and a hinged knee brace was placed, locked in full extension for initial weight-bearing protection.
Post-Operative Protocol & Rehabilitation
A structured, progressive rehabilitation protocol is paramount for successful ACL reconstruction outcomes. The protocol is typically criteria-based, with specific milestones for progression.
-
Phase I: Protection and Early Motion (Weeks 0-2)
- Weight-Bearing: Touch-down weight-bearing (TDWB) with crutches, with the brace locked in full extension. Gradual progression to partial weight-bearing (PWB) as tolerated.
- Range of Motion (ROM): Continuous Passive Motion (CPM) machine initiated immediately post-op, aiming for 0-90 degrees by the end of week 2. Passive extension is prioritized.
- Exercises: Quadriceps setting, straight leg raises (SLR) in multiple planes, ankle pumps, gluteal sets. Focus on controlling swelling (RICE protocol). No active hamstring strengthening or stretching initially with hamstring autograft to protect healing at the harvest site.
- Goals: Control pain and swelling, achieve full passive knee extension, 90 degrees of flexion, and establish quadriceps control.
-
Phase II: Intermediate Motion and Strength (Weeks 2-6)
- Weight-Bearing: Progress to full weight-bearing (FWB) and discontinue crutches by week 4-6, with the brace unlocked for gait.
- ROM: Achieve full active and passive range of motion (0-125+ degrees) by week 6.
- Exercises: Stationary cycling (light resistance), gentle closed-chain exercises (mini-squats, leg press 0-60 degrees), core strengthening, proprioceptive exercises (balance board, single-leg stance). Begin light hamstring strengthening (e.g., prone hamstring curls with minimal resistance) after week 4 for hamstring grafts, focusing on control.
- Goals: Restore full ROM, normalize gait, improve muscular strength, and enhance proprioception.
-
Phase III: Advanced Strengthening and Neuromuscular Control (Weeks 6-12)
- Brace: Discontinued as quadriceps control and stability improve.
- Exercises: Increased intensity of closed-chain strengthening (step-ups, lunges, squats), open-chain quadriceps strengthening (avoid resisted terminal knee extension (0-30 degrees) until week 12-16 to protect the graft). Introduce light jogging on a treadmill or soft surface, agility drills (ladder drills, shuttle runs), and sport-specific non-contact drills.
- Goals: Regain significant strength symmetry, improve cardiovascular endurance, and develop advanced neuromuscular control.
-
Phase IV: Return to Sport (Months 4-12+)
-
Criteria-Based Progression:
Return to sport is based on objective criteria, not simply time. This typically includes:
- Full pain-free range of motion.
- No effusion.
- Isokinetic strength testing (quadriceps and hamstrings) with Limb Symmetry Index (LSI) > 90% compared to the contralateral limb.
- Functional hop testing (single hop, triple hop, crossover hop, 6-meter timed hop) with LSI > 90%.
- Excellent neuromuscular control, agility, and sport-specific movement patterns.
- Psychological readiness assessment.
- Progression: Gradual reintroduction to sport-specific drills, initially without contact, progressing to controlled contact, and finally unrestricted play.
- Recommendation: For high-demand pivoting sports like soccer, return to competitive play is generally recommended no sooner than 9-12 months post-surgery , and often later, to allow for optimal graft maturation and integration. Re-rupture rates are significantly higher with earlier return.
-
Criteria-Based Progression:
Return to sport is based on objective criteria, not simply time. This typically includes:
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Thorough Clinical Examination is Paramount: Despite advanced imaging, a detailed history and physical exam can often diagnose an ACL injury and guide subsequent imaging. The Lachman test remains the most sensitive clinical test for acute ACL rupture. Don't rely solely on MRI; correlate with clinical findings.
- Identify Concomitant Injuries: Approximately 50% of ACL injuries have associated meniscal tears, and a significant percentage have chondral or collateral ligament injuries. MRI is crucial, but diagnostic arthroscopy provides the definitive assessment. Address all relevant pathology (e.g., meniscal repair vs. meniscectomy).
- Anatomic Tunnel Placement: Accurate femoral and tibial tunnel placement is critical for restoring knee kinematics, preventing impingement, and maximizing graft longevity. A more vertical femoral tunnel (transtibial technique) can lead to residual rotational instability. Anteromedial portal drilling for the femoral tunnel generally allows for a more anatomic footprint placement.
- Appropriate Graft Tensioning: The graft must be tensioned correctly—not too loose (leading to instability) and not too tight (leading to arthrofibrosis, loss of motion, or early graft failure). This is typically performed with the knee in 20-30 degrees of flexion with an anterior drawer.
- Individualized Rehabilitation: While protocols provide a framework, rehabilitation must be individualized based on the patient's biological healing, graft type, concomitant injuries, and progress. Close collaboration with a skilled physiotherapist is essential.
- Delayed Return to Sport: Emphasize to athletes that a minimum of 9 months, and often up to 12-18 months, is required before returning to high-risk pivoting sports. Objective criteria (strength, functional testing, psychological readiness) should dictate return, not just time. This significantly reduces re-rupture rates.
- Patient Education: Educate the patient pre-operatively about the entire process, including realistic expectations for recovery, potential complications, and the critical role of rehabilitation.
Pitfalls
- Missed Concomitant Injuries: Failing to diagnose or address significant meniscal, chondral, or collateral ligament injuries (especially Grade III MCL/LCL tears, posterior corner injuries) can lead to residual instability, persistent pain, and premature graft failure.
- Non-anatomic Tunnel Placement: The most common technical error. A too-anterior femoral tunnel can lead to graft impingement in extension and loss of flexion. A too-posterior femoral tunnel can result in a more vertical graft, leading to persistent rotational instability. A too-anterior tibial tunnel can cause graft impingement against the roof of the intercondylar notch in extension.
- Graft Impingement: Can occur if tunnels are malpositioned or if the notchplasty is inadequate, leading to graft wear, pain, and eventual failure.
- Inadequate Graft Fixation: Poor fixation can lead to micromotion, graft stretching, tunnel widening, and early failure.
- Aggressive Early Rehabilitation: Pushing too hard, too soon, especially with open-chain quadriceps exercises (0-30 degrees extension) in the early phases, can place excessive stress on the healing graft, potentially leading to stretching or failure. Overly aggressive hamstring strengthening too early can also compromise hamstring graft harvest site healing.
- Premature Return to Sport: The single biggest risk factor for re-rupture, particularly in young athletes returning to pivoting sports before 9 months post-op or without meeting objective strength and functional criteria.
- Arthrofibrosis / Stiffness: Can result from overly conservative rehabilitation, persistent inflammation, or an overtensioned graft. Early, controlled motion is crucial to prevent this.
- Infection: Although rare, surgical site infection is a serious complication that can jeopardize graft survival and knee function. Strict aseptic technique is mandatory.
- Neurovascular Injury: Although uncommon, potential injuries to the saphenous nerve (during medial incision/graft harvest) or peroneal nerve (during lateral approach or excessive traction) or popliteal artery are severe complications. Vigilance during surgery is key.
