Introduction & Epidemiology
Proximal clavicle fractures, constituting 2-5% of all clavicular fractures and approximately 1% of all fractures, present unique challenges due to their anatomical location, proximity to vital neurovascular structures, and inherent instability. Historically, these injuries were often managed non-operatively, primarily due to concerns regarding surgical risks in an anatomically complex region. However, this approach frequently led to suboptimal outcomes, including symptomatic malunion, nonunion, pain, and functional deficits, particularly in significantly displaced fractures or those involving the sternoclavicular (SC) joint.
The evolution of orthopedic trauma management, driven by advancements in surgical techniques, imaging modalities, and implant design, has shifted the paradigm towards more aggressive operative intervention for specific fracture patterns. The goal of surgical stabilization is to restore anatomical alignment, provide stable fixation, facilitate early mobilization, and achieve optimal functional recovery while minimizing complications. This comprehensive review aims to outline the current understanding and management strategies for complex proximal clavicle fractures, with a particular focus on the application of the sternoclavicular (SC) hook plate, incorporating detailed anatomical considerations, surgical techniques, and postoperative care protocols.
We consider the case of a 61-year-old male who sustained a right proximal clavicle fracture from a high-energy fall:
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy and biomechanics is paramount for safe and effective surgical management of proximal clavicle fractures. The medial third of the clavicle, approximately 5-6 cm in length, articulates with the manubrium of the sternum to form the sternoclavicular (SC) joint. This joint is the only true articulation between the upper extremity and the axial skeleton.
Medial Clavicle and SC Joint Morphology
The medial clavicle is typically stout and prismatic, distinct from the flattened lateral two-thirds. The articular surface, covered with fibrocartilage, is incongruent, with the clavicular surface being larger than the sternal facet. This incongruence contributes to the inherent instability of the SC joint, which is compensated by a robust ligamentous complex.
Ligamentous Stabilizers
The primary stabilizers of the SC joint include:
*
Anterior and Posterior Sternoclavicular Ligaments:
These are thick, fibrous capsules that envelop the joint, with the posterior ligament being stronger than the anterior. They resist anterior and posterior displacement of the clavicle relative to the sternum.
*
Interclavicular Ligament:
Connecting the medial ends of both clavicles, this ligament provides superior stability and limits upward displacement of the medial clavicle.
*
Costoclavicular (Rhomboid) Ligament:
This strong ligament connects the inferior surface of the medial clavicle to the first rib, acting as the primary restraint against superior and posterior displacement of the clavicle. It also prevents excessive medial clavicle rotation.
Surrounding Vital Structures
The medial clavicle and SC joint are in close proximity to numerous critical neurovascular and mediastinal structures, particularly posteriorly. These include:
*
Subclavian Artery and Vein:
Positioned inferoposterior to the clavicle.
*
Brachiocephalic Veins (right and left):
The left brachiocephalic vein crosses behind the manubrium.
*
Trachea and Esophagus:
Located posteriorly in the superior mediastinum.
*
Apex of the Pleura:
Risk of pneumothorax with deep instrumentation.
*
Recurrent Laryngeal Nerve:
Though less common, can be injured.
Figure: Lateral view illustrating the medial clavicle and its anatomical relationships.
Biomechanics of Injury
Proximal clavicle fractures often result from high-energy direct or indirect trauma to the shoulder or chest. The fracture pattern and displacement are dictated by the mechanism of injury and the pull of surrounding musculature (sternocleidomastoid, pectoralis major). Posterior displacement of the medial fragment is particularly concerning due to the risk of life-threatening injury to the great vessels and mediastinal structures. The stability of the SC joint, reliant on its robust ligamentous complex, is inherently compromised by fractures involving the medial epiphysis or metaphysis. Effective fixation must therefore counteract these deforming forces and restore overall stability.
Indications & Contraindications
The decision for operative versus non-operative management of proximal clavicle fractures is complex, weighing fracture characteristics, patient factors, and potential surgical risks.
Operative Indications
Operative management is generally favored for fractures that compromise function, present a risk to vital structures, or are unlikely to heal well with conservative treatment.
*
Significant Displacement or Angulation:
Fractures with substantial translation (e.g., > 1-2 cm) or severe angulation, particularly those involving the articular surface of the SC joint, leading to instability or impending skin compromise.
*
Posterior Displacement:
Any degree of posterior displacement of the medial fragment warrants strong consideration for urgent reduction and stabilization due to the risk of mediastinal compression (trachea, esophagus) or vascular injury (brachiocephalic vessels, subclavian vessels).
*
Open Fractures:
Require surgical debridement and stabilization to prevent infection and facilitate healing.
*
Neurovascular Compromise:
Evidence of compromise to the brachial plexus or subclavian vessels mandates emergent surgical exploration and reduction.
*
Polytrauma Patient:
In the context of multiple injuries, stable fixation of the clavicle can aid in overall patient mobilization and rehabilitation.
*
Pathologic Fractures:
Fractures occurring through bone weakened by tumors or metabolic disease.
*
Nonunion or Symptomatic Malunion:
Failed non-operative treatment resulting in persistent pain, functional limitation, or cosmetic deformity.
*
Fractures with Ligamentous Instability:
Particularly disruption of the costoclavicular or sternoclavicular ligaments, which may require repair or reconstruction in addition to fracture fixation.
Non-Operative Indications
Non-operative treatment remains appropriate for a subset of proximal clavicle fractures.
*
Minimally Displaced or Nondisplaced Fractures:
Fractures that maintain anatomical alignment and have no signs of instability or impending soft tissue compromise.
*
Stable Fractures:
Fractures where the surrounding soft tissues and ligamentous structures remain largely intact, providing sufficient stability for healing.
*
High Surgical Risk Patients:
Individuals with significant comorbidities that contraindicate general anesthesia or extensive surgery.
*
Patient Preference:
When conservative management is a well-informed choice made by the patient, provided it does not pose undue risk.
Contraindications
Absolute contraindications to surgical intervention are rare but include:
*
Active Local or Systemic Infection:
Until adequately treated.
*
Severe Systemic Illness:
When the risks of surgery clearly outweigh the potential benefits.
*
Extensive Soft Tissue Compromise:
Preventing safe wound closure or increasing infection risk (relative contraindication, may require staged approach).
The following table summarizes operative versus non-operative indications:
| Indication Type | Operative Management | Non-Operative Management |
|---|---|---|
| Displacement | Significant displacement (>1-2 cm), angulation, articular step-off, posterior displacement | Minimally displaced, nondisplaced, stable fractures |
| Fracture Type | Unstable Neer Type I, II, III (medial epiphysis, ligament disruption, articular involvement) | Stable Neer Type I (medial epiphysis, minimally displaced) |
| Soft Tissue | Open fractures, impending skin compromise | Closed, stable soft tissue envelope |
| Neurovascular | Any neurovascular compromise | Intact neurovascular status |
| Associated Injury | Polytrauma with need for early mobilization, associated mediastinal injury | Isolated injury, no other critical injuries |
| Healing | Nonunion or symptomatic malunion | Acute fracture with high likelihood of uncomplicated union |
| Patient Factors | Young, active patients seeking full functional recovery; otherwise healthy patients | Elderly, sedentary patients; patients with severe comorbidities precluding surgery |
| Pain/Function | Persistent severe pain or significant functional limitation after initial non-op trial | Mild pain, good functional prognosis with conservative care |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes and mitigating risks in proximal clavicle fracture surgery.
Comprehensive Imaging
-
Plain Radiographs (DR): Standard anteroposterior (AP) and 45-degree cephalic tilt (serendipity) views are essential for initial assessment. These help evaluate fracture displacement, comminution, and SC joint alignment. However, complex anatomy and overlapping structures often limit their diagnostic utility for the medial clavicle.
Figure: Pre-operative DR demonstrating a right proximal clavicle fracture. -
Computed Tomography (CT) Scan with 3D Reconstruction: This is the gold standard for detailed evaluation of proximal clavicle fractures. CT accurately delineates fracture morphology, identifies comminution, assesses articular involvement of the SC joint, and critically evaluates the degree and direction of displacement, especially posterior displacement. 3D reconstructions are invaluable for understanding complex fracture patterns and planning implant placement. Vascular CT may be indicated if vascular injury is suspected.
Figure: Pre-operative CT scan revealing the complex fracture pattern of the right proximal clavicle. -
Magnetic Resonance Imaging (MRI): While not routine, MRI may be considered if concomitant soft tissue injuries, such as disc tears within the SC joint or significant ligamentous disruption, are suspected, particularly in chronic cases or dislocations.
Medical Optimization and Neurovascular Assessment
Prior to surgery, patients should undergo thorough medical optimization. A comprehensive neurovascular examination of the upper extremity is mandatory to document any pre-existing deficits and to compare with post-operative status. For posterior dislocations or significantly displaced fractures, a multidisciplinary approach involving cardiothoracic or vascular surgeons should be considered, as reduction maneuvers can lead to further injury, and emergent sternotomy may be required.
Anesthesia and Patient Positioning
- Anesthesia: General anesthesia is typically employed. Careful attention should be paid to airway management, especially in cases of posterior displacement where tracheal compression may be present. A central line may be considered for severe injuries.
- Patient Positioning: The patient is usually positioned supine on a radiolucent operating table, often in a beach chair or semi-recumbent position. A bump placed between the scapulae can help extend the neck and retract the shoulders, improving access to the medial clavicle and SC joint. The head should be turned slightly away from the affected side.
- C-arm Setup: An image intensifier (C-arm) should be positioned to allow for clear AP and lateral views of the medial clavicle and SC joint throughout the procedure. Oblique views (e.g., 45-degree cephalic tilt) may also be helpful.
- Draping: The entire upper extremity, shoulder, and ipsilateral neck/chest should be prepped and draped freely to allow for manipulation of the shoulder and arm for reduction maneuvers. Adequate exposure of the sternum and adjacent ribs is also crucial.
Implant Selection
For proximal clavicle fractures, various fixation options exist, each with its advantages and disadvantages.
*
Sternoclavicular Hook Plate (cc胸锁钩钢板):
This plate, as highlighted in the initial content, is specifically designed for medial clavicle fractures and SC joint instability. Its unique hook configuration allows for engagement with the posterior aspect of the sternum, providing strong superior-inferior and anterior-posterior stability. The main body of the plate is fixed to the clavicle with screws.
Figure: An alternative imaging view of the shoulder/clavicle, potentially useful in pre-operative assessment.
*
Standard Locking Plates:
While possible, standard plates may struggle to achieve robust fixation in the osteopenic medial clavicle or when significant ligamentous disruption necessitates SC joint stabilization.
*
Tension Band Wiring / K-wires:
May be used as an adjunct or for very simple fracture patterns, but often lack sufficient rotational and compressive stability.
*
Transarticular K-wires:
Can be used for SC joint dislocation, but carry risks of wire migration and mediastinal injury, and provide no fracture fixation.
*
Suture Anchor Repair / Ligament Reconstruction:
For chronic instability or complete ligamentous avulsion without significant fracture comminution.
*
Intramedullary Devices:
Less common for proximal clavicle due to complex morphology and proximity to SC joint.
The choice of implant depends on fracture type, bone quality, surgeon preference, and patient factors. The SC hook plate provides robust fixation, particularly in cases where the fracture extends into the SC joint or when associated ligamentous instability requires direct joint stabilization.
Detailed Surgical Approach / Technique
Surgical treatment of proximal clavicle fractures requires meticulous technique to achieve stable reduction, secure fixation, and minimize the risk of injury to vital mediastinal structures. This section focuses on the open reduction and internal fixation (ORIF) approach, specifically utilizing the sternoclavicular hook plate.
1. Incision and Exposure
- Incision: A transverse incision (Langer's lines) approximately 5-7 cm long is typically made over the medial clavicle, centered over the fracture site and extending across the SC joint. Alternatively, a longitudinal incision can be used, particularly in cases requiring extensive exposure or when a posterior dislocation necessitates greater access to the mediastinum. The platysma muscle is carefully incised in line with the skin incision.
- Subplatysmal Dissection: Subplatysmal flaps are raised superiorly and inferiorly to expose the medial clavicle, SC joint, and a portion of the manubrium. Care must be taken to identify and preserve the supraclavicular nerves to minimize post-operative sensory deficits.
- Identification of Critical Structures: The sternal head of the sternocleidomastoid muscle is typically retracted superiorly. The anterior SC joint capsule and ligaments are exposed. The jugular notch and the superior border of the manubrium are important landmarks. Extreme caution is exercised during any deep dissection posterior to the clavicle and sternum, as this area harbors the great vessels and pleura. A blunt instrument can be used to palpate behind the sternum to ensure no immediate pulsatile structures are encountered.
2. Fracture Reduction
- Mobilization: The fracture fragments are carefully mobilized, and hematoma is evacuated. Care is taken to avoid devascularization of smaller fragments.
-
Reduction Maneuvers:
Reduction can be challenging due, to muscle pull and fracture comminution.
- For anterior displacement, direct pressure or a bone clamp may be used.
- For superior displacement, inferior traction on the shoulder may help.
-
For posterior displacement:
This is critical and requires careful technique.
- The arm on the affected side is often pulled posteriorly and superiorly with abduction, while an assistant applies traction to the arm.
- A towel clamp or reduction clamp may be carefully placed on the medial fragment to manipulate it anteriorly.
- In cases of severe posterior displacement or impaction, a small, blunt, curved instrument (e.g., Hohmann retractor or Doyen rib elevator) can be carefully passed behind the medial clavicle or manubrium to lever the fragment anteriorly. This maneuver must be performed with utmost vigilance to avoid mediastinal injury. The posterior SC ligament may need to be incised.
-
Temporary Fixation:
Once anatomical or near-anatomical reduction is achieved, it can be maintained with provisional K-wires, bone clamps, or joystick manipulators. Intraoperative fluoroscopy confirms the reduction in multiple planes (AP, lateral, serendipity view).
Figure: Intraoperative view during open reduction and internal fixation, showing temporary fixation and exposure.
3. Sternoclavicular Hook Plate Application
The "cc胸锁钩钢板" or SC hook plate is particularly suitable for these complex fractures.
*
Plate Contouring:
The hook plate must be carefully contoured to match the superior and posterior curvature of the medial clavicle and the sternum. Pre-bending to the appropriate angle is crucial for optimal fit and minimizing soft tissue irritation.
*
Hook Placement:
1. The distal part of the plate is first secured to the clavicle with screws to ensure proper alignment.
2. The hook component is then carefully advanced inferiorly and posteriorly, aiming to engage the posterior cortex of the manubrium, just inferior to the clavicular notch.
3. A small, blunt instrument or finger can be used to protect the retrosternal structures while the hook is advanced. This is the most critical step due to the proximity of mediastinal structures. The depth of hook penetration must be precise – sufficient to provide stable anchorage but not excessive to impinge upon or penetrate vital organs.
4. The hook should sit snugly against the posterior sternal cortex. The original design allows the hook end to pass through a perforation in the sternum and be secured with a screw cap. Newer designs may simply hook over the posterior sternal cortex.
5. Once the hook is properly seated, the remaining screws are inserted into the clavicle, ensuring bicortical purchase where possible and avoiding penetration into the SC joint or adjacent soft tissues.
Figure: Close-up intraoperative view of sternoclavicular hook plate application, demonstrating the hook engaging the sternum.
*
Advantages of SC Hook Plate:
As noted in the seed content, the SC hook plate offers robust stability by anchoring to the sternum, thereby stabilizing both the fracture and the SC joint. This helps maintain reduction and allows for early, controlled motion, potentially preventing implant fatigue failure by distributing stress. It can preserve the micro-motion of the SC joint, which is advantageous biomechanically.
*
Disadvantages of SC Hook Plate:
The seed content accurately highlights concerns:
*
Risk of Sternum Cut-out/Erosion:
Prolonged loading or insufficient bone quality can lead to erosion or cutting out of the sternal hook, potentially leading to loss of fixation.
*
Risk of Mediastinal Injury:
The most serious risk is injury to retrosternal structures (great vessels, pleura, trachea) during hook insertion or subsequent migration. Meticulous technique and intraoperative imaging are crucial.
*
Implant Prominence/Pain:
The plate and hook can be palpable and cause local irritation, discomfort, or pain, often necessitating hardware removal after fracture union.
*
Local Bone Resorption:
Localized bone resorption around the hook tip can occur over time.
4. Intraoperative Fluoroscopy
Prior to closure, fluoroscopic images (AP, lateral, and serendipity views) are taken to confirm fracture reduction, implant position, screw length, and integrity of the SC joint.
5. Wound Closure
The wound is irrigated thoroughly. The platysma and subcutaneous tissues are closed in layers. The skin is closed with standard techniques. A drain may be placed if significant bleeding or dead space is present.
Complications & Management
Despite careful surgical technique, complications associated with operative management of proximal clavicle fractures, particularly with SC hook plate fixation, can occur. Early recognition and appropriate management are crucial.
General Complications
- Infection: Superficial or deep surgical site infection can occur. Incidence is generally low (1-5%). Management involves antibiotics, wound debridement, and potentially implant removal in deep infections after union or for persistent infection.
- Nonunion/Malunion: Failure of bone healing or healing in an unacceptable anatomical position. Risk factors include severe comminution, poor bone quality, infection, and inadequate fixation. Incidence varies but can be higher in complex patterns. Management may involve revision ORIF, bone grafting, or osteotomy for symptomatic malunion.
- Neurovascular Injury: Direct injury to the subclavian vessels, brachial plexus, or other mediastinal structures during dissection or instrumentation. Incidence is low but carries high morbidity. Prevention through careful dissection and imaging is paramount. Management is often emergent multidisciplinary repair.
- Pneumothorax: Injury to the apical pleura, particularly during deep dissection or hook/screw placement. Manifests as respiratory distress. Management involves chest tube insertion.
- Implant Failure: Plate breakage or screw pullout due to insufficient fixation, premature loading, or nonunion. Management is typically revision surgery.
Specific Complications of Sternoclavicular Hook Plate
-
Sternum Cut-out / Erosion:
The hook can erode through the posterior sternal cortex due to continuous motion, implant prominence, or osteopenia, leading to loss of fixation.
- Incidence: Varies, reported in several case series.
- Management: Revision with different fixation, bone grafting, or removal of symptomatic hardware after union.
-
Posterior Mediastinal Injury / Vascular Injury:
The most catastrophic complication. The hook or drill bit can penetrate vital structures like the brachiocephalic vessels, trachea, or esophagus during insertion or subsequent migration.
- Incidence: Rare but life-threatening.
- Management: Immediate surgical exploration (potentially sternotomy), vascular repair, tracheobronchial repair, management of pneumo-/hemothorax. Prevention is key through careful technique and intraoperative fluoroscopy.
-
Implant Irritation / Pain:
The hook or plate can be prominent under the skin, causing local pain, tenderness, or discomfort, especially with arm movements or pressure.
- Incidence: High, often leading to planned hardware removal.
- Management: Symptomatic relief, and typically elective hardware removal after fracture union (usually 6-12 months post-op).
-
Loss of Reduction:
Despite stable fixation, severe comminution or persistent deforming forces can lead to some degree of reduction loss.
- Incidence: Varies with fracture complexity and bone quality.
- Management: If minor and asymptomatic, may be observed. Significant loss requiring functional impairment may necessitate revision.
-
Local Bone Resorption:
Bone around the hook tip can resorb over time, potentially leading to loosening or loss of stability.
- Incidence: Variable, often identified at hardware removal.
- Management: Usually not problematic if fracture has united; if symptomatic or associated with nonunion, revision.
The following table summarizes common complications and their management:
| Complication | Incidence | Management / Salvage Strategies |
|---|---|---|
| Surgical Site Infection | 1-5% | Superficial: Oral antibiotics, local wound care. Deep: IV antibiotics, surgical debridement, implant retention if stable and infection controlled, or implant removal after union. Persistent deep infection: Implant removal. |
| Nonunion | 5-15% (higher for complex) | Revision ORIF with debridement of nonunion site, rigid internal fixation (e.g., locking plate, if hook plate insufficient), autogenous bone grafting, electrical stimulation. |
| Symptomatic Malunion | Variable | Osteotomy to correct deformity, revision fixation if required. Soft tissue release. |
| Neurovascular Injury | Rare, but critical | Emergent surgical exploration, vascular repair (e.g., patch graft, end-to-end anastomosis), nerve repair/grafting. Multidisciplinary team approach. |
| Pneumothorax | Rare | Chest tube insertion, observation, respiratory support. |
| Implant Failure | 5-10% (depending on type) | Revision surgery with stronger fixation, different implant type, or bone grafting if nonunion is present. |
| Sternum Cut-out / Erosion | Variable (SC hook plate) | If symptomatic or unstable: Implant removal. If fracture united: Symptomatic management. If nonunion: Revision surgery with alternative fixation or bone grafting. |
| Posterior Mediastinal Injury | Rare, life-threatening | Emergent thoracic/vascular surgery consultation, median sternotomy if needed, direct repair of injured structures (vessels, trachea, esophagus). |
| Implant Irritation / Pain | High (especially SC hook plate) | Symptomatic management (NSAIDs, activity modification). Elective hardware removal typically 6-12 months post-operatively once fracture union is confirmed and patient symptoms warrant removal. |
| Loss of Reduction | Variable | If minor and asymptomatic: Observation. If significant and symptomatic (pain, dysfunction): Revision surgery, potentially with stronger implant or bone graft. |
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is essential for optimizing functional recovery and preventing complications after surgical fixation of proximal clavicle fractures. The protocol aims to protect the repair, facilitate bone healing, restore range of motion (ROM), and regain strength.
Phase I: Immobilization & Early Motion (0-6 weeks Post-Op)
- Immobilization: The arm is typically immobilized in a sling for comfort and protection for the initial 2-4 weeks. The duration depends on fracture stability, fixation strength, and patient adherence. The goal is to prevent sudden, uncontrolled movements that could jeopardize the fixation.
- Pain Management: Aggressive pain control with a multimodal approach (NSAIDs, acetaminophen, opioids as needed) to facilitate participation in therapy.
- Early Passive Range of Motion (PROM): Gentle, protected pendulum exercises are initiated within the first week. The uninjured shoulder is also exercised to prevent stiffness.
- Elbow, Wrist, Hand ROM: Active ROM exercises for the elbow, wrist, and hand are encouraged immediately to prevent stiffness and maintain circulation.
- Activities of Daily Living (ADLs): Patient education on safe ADLs, avoiding lifting, pushing, or pulling with the affected arm. Emphasis on maintaining good posture.
- Weight-Bearing Restrictions: Strict avoidance of weight-bearing on the affected upper extremity.
-
Implant-Specific Considerations:
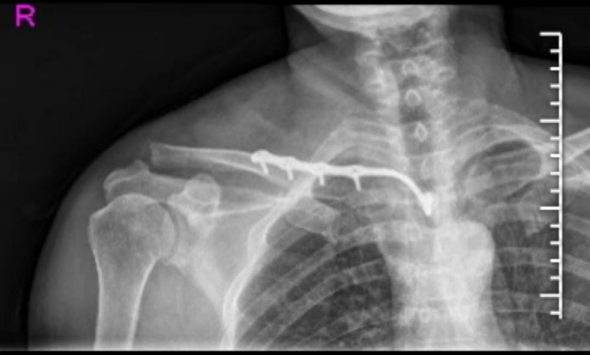
For SC hook plates, excessive abduction or extension may put undue stress on the hook, thus these motions are initially limited.

Figure: Post-operative X-ray demonstrating stable fixation of the proximal clavicle fracture with an SC hook plate.
Phase II: Active-Assisted & Active ROM (6-12 weeks Post-Op)
- Radiographic Assessment: Follow-up radiographs (AP, serendipity views) are obtained around 6 weeks to assess fracture healing. Clinical signs of union (absence of tenderness, pain-free gentle motion) are also monitored.
- Discontinuation of Sling: If union is progressing satisfactorily and pain is controlled, the sling can be discontinued.
- Active-Assisted Range of Motion (AAROM): Therapist-assisted or self-assisted exercises (e.g., pulley exercises, cane exercises) are initiated to gradually restore full shoulder ROM (flexion, abduction, rotation).
- Gentle Active Range of Motion (AROM): As pain allows and bone healing progresses, active exercises are introduced. The goal is to achieve near-full AROM by the end of this phase.
- Isometrics: Gentle isometric strengthening exercises for the shoulder girdle muscles (deltoid, rotator cuff, scapular stabilizers) can be introduced once pain-free.
- Avoidance of Heavy Lifting: Continue to avoid heavy lifting or high-impact activities.
Phase III: Progressive Strengthening & Return to Activity (12+ weeks Post-Op)
- Radiographic Confirmation of Union: Clinical and radiographic evidence of complete fracture union is usually present by 12-16 weeks.
-
Progressive Strengthening:
Once union is confirmed, a comprehensive strengthening program is initiated. This includes:
- Resistance exercises with elastic bands or light weights for all shoulder and scapular muscles.
- Proprioceptive and neuromuscular control exercises.
- Core strengthening to support upper extremity function.
- Functional Training: Sport-specific or work-specific activities are gradually introduced.
- Return to Full Activities: Gradual return to full activities, including contact sports or heavy labor, typically occurs between 4-6 months, depending on functional recovery, strength, and confidence.
- Hardware Removal: For SC hook plates, hardware removal is often planned and recommended due to the high incidence of implant irritation and prominence. This is typically performed 6-12 months post-operatively, after complete radiographic union. The decision for removal is based on symptoms and patient preference. Post-removal, a brief period of protection (e.g., 2-4 weeks in a sling) may be advised, followed by a short course of rehabilitation.
Throughout all phases, patient education regarding activity modification, proper body mechanics, and adherence to the rehabilitation program is paramount for achieving optimal functional outcomes and minimizing the risk of complications.
Summary of Key Literature / Guidelines
The management of proximal clavicle fractures has evolved, with a growing body of literature supporting operative intervention for unstable or significantly displaced injuries. While historical guidelines leaned towards non-operative management, contemporary evidence underscores the benefits of stable fixation for restoring anatomy and expediting functional recovery.
- Shift Towards Operative Management: Early studies documented high rates of unsatisfactory outcomes, including symptomatic nonunion and malunion, with non-operative treatment of significantly displaced medial clavicle fractures. This led to a re-evaluation, with modern consensus favoring surgical stabilization for fractures that are displaced, comminuted, intra-articular, or pose a risk to vital structures.
- Role of Advanced Imaging: The advent and widespread availability of CT with 3D reconstruction have revolutionized the diagnosis and pre-operative planning for these complex fractures. CT provides unparalleled detail regarding fracture morphology, displacement, and relationship to mediastinal structures, guiding surgical decision-making and technique.
-
Sternoclavicular Hook Plate (SC Hook Plate) Efficacy:
The SC hook plate has emerged as a viable and effective option for stable fixation of proximal clavicle fractures, especially those involving the SC joint or with concomitant ligamentous instability.
- Union Rates: Studies have reported high union rates (typically >90%) with SC hook plate fixation, demonstrating its effectiveness in promoting bone healing.
- Functional Outcomes: Patients generally achieve good to excellent functional scores, with restoration of shoulder range of motion and strength. Early mobilization facilitated by stable fixation contributes significantly to these outcomes.
- Complication Profile: While effective, the SC hook plate has a distinct complication profile, as detailed previously. Implant irritation and prominence requiring hardware removal are common, reported in 50-80% of cases in some series. Serious retrosternal complications, while rare, emphasize the need for extreme surgical caution and meticulous technique.
- Comparison to Other Fixation Methods: While direct comparative studies are limited, the SC hook plate offers unique advantages in addressing SC joint instability in conjunction with fracture fixation, which may be difficult to achieve with standard locking plates or intramedullary nails. However, other methods like transarticular K-wires (for SC dislocations without significant fracture) or suture anchor repair of ligaments (for chronic instability) remain relevant in specific scenarios.
- Emerging Techniques: Ongoing research explores newer implant designs, bioabsorbable fixation, and minimally invasive approaches. However, the complexity of the region and the need for robust stability limit the applicability of many of these in routine practice for complex fractures.
-
Current Guidelines Summary:
- Non-operative care remains the standard for non-displaced or minimally displaced, stable fractures.
-
Operative intervention
is strongly indicated for:
- Displaced articular fractures involving the SC joint.
- Significantly displaced or comminuted diaphyseal fractures of the medial clavicle.
- Posteriorly displaced fractures/dislocations (urgent management).
- Open fractures.
- Fractures with neurovascular compromise.
- Symptomatic nonunion or malunion.
- Pre-operative CT is highly recommended for detailed assessment.
- SC hook plates offer robust stability but have a high rate of implant removal due to irritation. Careful surgical technique is paramount to avoid mediastinal injury.
- Structured rehabilitation with early, controlled motion is crucial for optimal functional recovery.
In conclusion, the management of complex proximal clavicle fractures requires a thorough understanding of the anatomy, careful patient selection, meticulous surgical technique, and a comprehensive rehabilitation strategy. The SC hook plate provides a valuable tool for achieving stable fixation in these challenging injuries, enabling early functional recovery, though its unique risks and the high likelihood of subsequent hardware removal must be carefully considered and discussed with patients. Continued research into improved implant designs and surgical approaches will further refine treatment strategies for this complex injury pattern.
