The diagnosis of fractures and principles of treatment

11 Palpation The sharp edge of a fracture may be palpable. Note also the presence of localised oedema. This is a particularly useful sign over hair-line and stress fractures. The development of oedema may, however, take some hours to reach detectable proportions.

12 Other signs If the fracture is mobile, moving the part may produce angulation or crepitus from the bone ends rubbing together. In addition, the patient will experience severe pain from such movement. These signs may be inadvertently observed during routine examination of the patient, but should not be sought unless the patient is unconscious and the diagnosis is in doubt.
13 Radiographic examination In every case of suspected fracture, radiographic examination of the fracture is mandatory. Radiographs of the part will generally give a clear indication of the presence of a fracture and provide a sound basis for planning treatment. In the case where there is some clinical doubt, radiographs will reassure patient and surgeon and avert any later medicolegal criticism.
Radiographers in the United Kingdom receive thorough training in the techniques for the satisfactory visualisation of any suspect area, but it is essential that they in turn are given clear guidance as to the area under suspicion. The request form must be quite specific, otherwise mistakes may occur. At its simplest, the request must state both the area to be visualised and the bone suspected of being fractured. It is desirable to include the joints above and below the fracture. It need hardly be stressed that a thorough clinical examination should precede the completion of the radiographic request if repetition and the taking of unnecessary films are to be avoided.
The following table lists some of the commonest errors made in the filling in of request forms

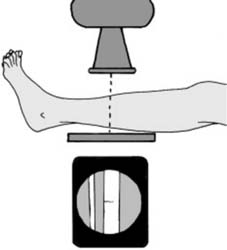
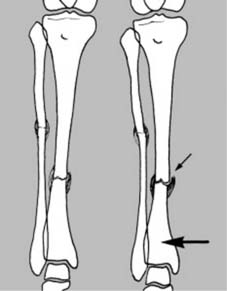
14 The standard projections: These are an anteroposterior (AP) and lateral. Ideally the beam should be centred over the area of suspected fracture, with visualisation of the proximal and distal joints. This is especially important in the paired long bones where, for example, a fracture of the tibia at one level may be accompanied by a fibular fracture at another
15 Comparison films: Where there is some difficulty in interpreting the radiographs (e.g. in the elbow region in children where the epiphyseal structures are continually changing, or where there is some unexplained shadow, or a congenital abnormality) films of the other side should be taken for direct comparison
16 Oblique projections In the case of the hand and foot, an oblique projection may be helpful when the lateral gives rise to confusion due to the superimposition of many structures. Such oblique projections may have to be specifically requested when they are not part of an X-ray department’s routine
17 Localised views Where there is marked local tenderness, but routine films are normal, coned-down localised views may give sufficient gain in detail to reveal for example a hair-line fracture: if such films are also negative, the radiographs should be repeated after an interval of 10–14 days if the symptoms are persisting (see also Hair-line Fractures in Ch. 1/Frame 13)
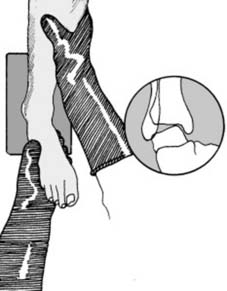
18 Stress films (a) Stress films can be of value in certain situations: (i) When a complete tear of a major ligament is suspected, e.g., where the lateral ligament of the ankle is thought to be torn, radiographs of the joint taken with the foot in forced inversion may demonstrate instability of the talus in the ankle mortice. (Local or general anaesthesia may be required in fresh injuries.)
19 Stress films (b) (ii) Stress films may also be used where there is some doubt as to stability of a uniting fracture. They may also be employed where the possibility of refracture arises.
Other visualisation techniques
1 CT (CT) scans
2 AP and lateral tomography
3 Technetium bone scans
Technetium tagged methylene diphosphate (99Tcm-methylene diphosphate (MDP)) can be used 48 hours after an injury to demonstrate bone activity at a fracture site, and confirm the presence of a fracture when other methods of detection have failed.
4 MRI scans
5 Bone scanning with SPECT (single-photon-emission computed tomography)
6 Ultrasound
Pitfalls
Treatment of fractures
Primary aims
Initial management
Some general principles in the initial management of cases of multiple injuries are well established, and may be summarised with the mnemonic ABCDE(F)
A = Airway